Systematic Notchplasty in Primary ACL Reconstruction Using Hamstring Autografts: A Prospective Cohort Study on the Rate of Secondary Arthrolysis
Adrien Saint-Etienne, Alexandre Hardy, Antonio Miele, Nicolas Lefevre, Olivier Grimaud, Alain Meyer, Yoann Bohu

TL;DR
This study found that performing notchplasty during ACL surgery with hamstring grafts did not reduce the need for arthrolysis, suggesting arthrofibrosis has multiple causes.
Contribution
The study is one of the first to prospectively evaluate the effect of systematic notchplasty on arthrolysis rates in ACL reconstruction.
Findings
No significant difference in arthrolysis rates between the notchplasty and non-notchplasty groups.
Functional outcomes and return-to-sport rates were similar across both groups.
Over 90% of patients in both groups reported satisfaction with their surgical outcomes.
Abstract
Background: Arthrofibrosis requiring arthrolysis is a relevant complication after anterior cruciate ligament (ACL) reconstruction. It has been suggested that intercondylar notch impingement may contribute to this outcome. The aim of this study was to evaluate whether systematic notchplasty during primary ACL reconstruction with hamstring autografts reduces the rate of secondary arthrolysis. Methods: Two groups of patients undergoing primary ACL reconstruction were compared: 149 patients without notchplasty and 140 patients with notchplasty, each with a minimum follow-up of 2 years. The incidence of arthrolysis and other complications, functional outcome scores, and return-to-sport data were analyzed. Results: No significant difference was observed in the rate of arthrolysis: Seven patients (4.7%) were in the non-notchplasty group, with seven patients (5.0%) in the notchplasty group (p =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
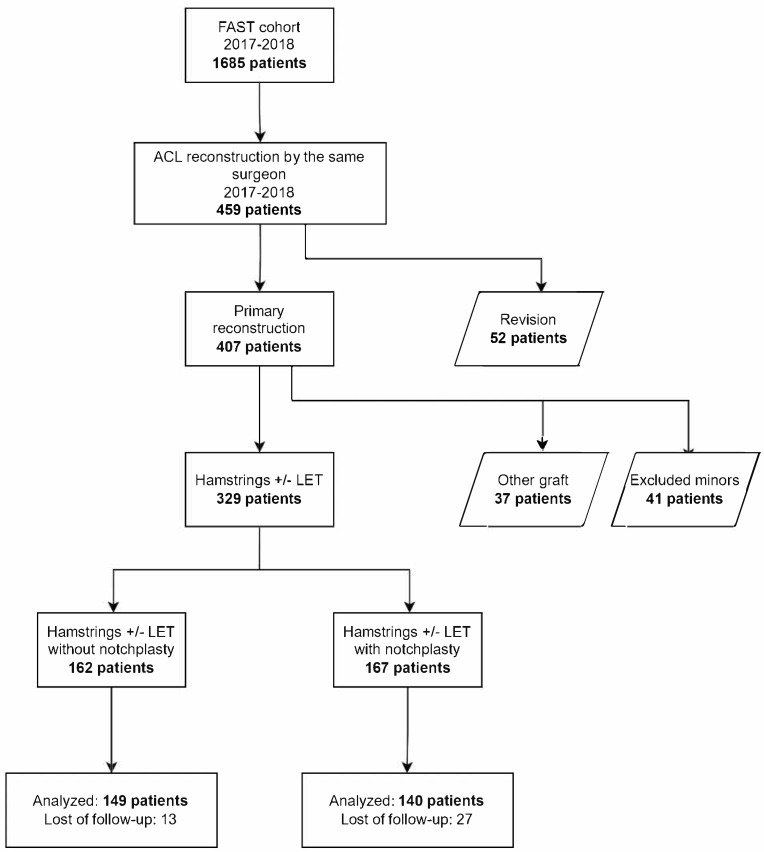 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Electrical Contact Performance and Analysis · Adhesion, Friction, and Surface Interactions
1. Introduction
One of the most frequent complications following anterior cruciate ligament (ACL) reconstruction is a knee extension deficit during the early postoperative period. This limitation may persist for more than 3 months and become chronic [1], with reported rates ranging from 1% to 10.9% depending on the series [2,3,4,5].
Arthrofibrosis, defined as pathological scar tissue formation leading to stiffness and loss of motion, is a complex and multifactorial complication. Among the potential causes of extension loss, intercondylar notch impingement has been suggested as one possible mechanism, although others—such as graft malposition, overtensioning, or extra-articular procedures—are also implicated.
Intercondylar notch impingement occurs when there is an imbalance between the “container” and the “content”: malposition of the tunnels causing graft–femur conflict [6,7], an oversized graft [7], or a congenitally small and narrow notch [8,9].
Notchplasty, a technically simple procedure performed with a motorized shaver or burr, aims to enlarge the intercondylar space to prevent or treat graft impingement. However, some cadaveric studies have reported that notchplasty alters knee biomechanics by increasing tibial translation and graft stresses [10], potentially impairing graft integration [11] and functional outcomes.
Clinical evidence on notchplasty remains limited. Only two clinical studies have specifically evaluated its effect on extension loss and the risk of arthrolysis [12], highlighting the scarcity of data in this under-reported area.
The present study investigated whether systematic notchplasty during primary single-bundle ACL reconstruction using hamstring autografts reduces the rate of secondary arthrolysis. The primary objective was to compare the incidence of arthrolysis between ACL reconstruction alone and ACL reconstruction with notchplasty. Secondary objectives were to compare complications, functional outcomes, and retear rates between the two groups. The rationale for including notchplasty was based on the hypothesis that enlarging the intercondylar notch might reduce graft impingement and subsequent extension deficits.
2. Materials and Methods
A single-center prospective cohort study was initiated in 2012, including all patients operated on by five senior surgeons for ACL reconstruction. The study was approved by the institutional research ethics committee. Informed consent was obtained at enrollment and questionnaire completion.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Comité de Protection des Personnes (CPP) Île-de-France VI, Groupe Hospitalier Pitié-Salpêtrière [on 6 February 2013]. It forms part of the French prospective ACLR cohort study (ClinicalTrials.gov identifier: NCT02511158). This report follows the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines. The study was conducted using data from a cohort established in 2012, for which ethical approval was obtained in 2013. The cohort includes both a retrospective phase (data collected up to 2013) and a prospective phase (data collected thereafter). All patients included in the present analysis were recruited prospectively from 2017 onwards.
2.1. Study Population
One surgeon performed notchplasty in all patients operated in 2018. To create a comparable cohort with ≥2 years follow-up, patients operated in 2017 without notchplasty by the same surgeon were used as controls. Thus, a retrospective single-surgeon analysis of prospectively collected data was performed.
Inclusion criteria were patients ≥18 years, with or without meniscal injury, undergoing primary ACL reconstruction using semitendinosus and gracilis (STG) hamstring autografts. Lateral extra-articular tenodesis was performed in selected cases. Exclusion criteria: other techniques, concomitant ligament surgery, osteotomy, revision ACL, or refusal. In particular, patients requiring concomitant MCL, PCL, or posterolateral corner reconstruction were excluded. Partial sprains or isolated MCL/PCL lesions that did not require surgical treatment were included and managed non-operatively.
Between 2017 and 2018, 1685 patients were in the cohort; 459 underwent ACL reconstruction by the same surgeon. After excluding 52 revisions, 41 minors, and 37 with other grafts, 329 remained. Notchplasty was performed in 167 patients in 2018 (Figure 1).
Forty patients were lost to follow-up, leaving 289 (87.8%). Preoperative characteristics were comparable (Table 1), except for follow-up duration, which was longer in the 2017 non-notchplasty group (mean 35.4 months) vs. the 2018 notchplasty group (mean 27.4 months, p < 0.0001), explained by surgical year. Associated lesions were similar (Table 2). The population was representative of the broader ACL cohort at our institution, supporting external validity.
2.2. Patient Characteristics
Forty of the 329 eligible patients were lost to follow-up or declined participation, leaving 289 (87.8%) for analysis. The preoperative characteristics of the two groups were comparable (Table 1), except for the length of follow-up, which was significantly longer in the 2017 non-notchplasty group (mean 35.4 months) than in the 2018 notchplasty group (mean 27.4 months, p < 0.0001). Since all secondary arthrolysis procedures occurred within the first 6 months postoperatively, the difference in mean follow-up duration (35.4 vs. 27.4 months) is unlikely to have influenced the primary outcome. Both groups had a minimum follow-up of 24 months for functional outcomes.
Associated lesions were similar between groups (Table 2). The study population was representative of the broader ACL reconstruction cohort treated at our institution in terms of age, activity level, and graft type, supporting external validity
2.3. Study Protocol, Surgical Technique
Arthroscopic ACL reconstruction was performed with an STG graft. Grafts were prepared as quadrupled hamstring constructs unless tendon length/quality required a tripled configuration. The femoral tunnel was created via an anteromedial portal (inside-out), fixed with an Endobutton femorally and interference screw tibially.
If necessary (retear risk, pivot shift, high-level athletes), lateral extra-articular tenodesis was performed. This consisted of a modified Lemaire procedure using the iliotibial band.
In 2018, notchplasty was applied systematically as part of the operating surgeon’s standardized protocol, reflecting prevailing practice patterns at the institution at that time and aiming to minimize any potential graft–notch impingement in high-throughput clinical care.
About 3 mm of bone (width and depth, corresponding to burr size) was resected from the medial surface of the lateral condyle and notch roof with a motorized shaver to enlarge the intercondylar space and reduce graft impingement.
The postoperative protocol was standardized: immediate weight-bearing, hinged brace, and physiotherapy from week 1. Rehabilitation emphasized early quadriceps activation, hamstring relaxation, and rapid recovery of extension.
Patients were evaluated at 6 weeks and 8 months. If deficit persisted at 6 weeks, physiotherapy was intensified. At 4 months, persistent >5° deficit triggered MRI (cyclops, arthrofibrosis) [5], and, if confirmed, arthrolysis.
At 6, 12, and 24 months, patients completed online questionnaires (Websurvey.fr^®^). These included validated instruments: ACL-RSI [13], IKDC [14], Lysholm [15], KOOS [16]; plus items on return to running, pivoting, preinjury sport, time to return, and performance level. Automated reminders and follow-up phone calls were used to maximize compliance.
2.4. Statistical Analysis
Sample size was calculated assuming a 10% arthrolysis rate in the non-notchplasty group vs. 2% in the notchplasty group. With α = 0.05 and power = 80%, 138 per group were required.
Student’s t-test or ANOVA were used for quantitative variables; Chi-square or Fisher’s exact test for categorical variables. Analyses were performed in RStudio V1.1.463 (RStudio Inc., Boston, MA, USA).
All analyses were patient-level; no clustering adjustment was required. An intention-to-treat approach was adopted, and patients lost to follow-up were excluded without imputation.
3. Results
3.1. Rate of Arthrolysis and Other Complications
There was no significant difference in the rate of arthrolysis between the two groups: 7 patients (4.7%) in the non-notchplasty group and 7 patients (5.0%) in the notchplasty group (p = n.s.) (Table 3).
Among these 14 patients requiring secondary arthrolysis, intraoperative findings confirmed the presence of cyclops lesions in most cases. All arthrolysis procedures were performed within the first 6 months postoperatively, confirming that differences in mean follow-up duration between groups did not influence the primary outcome.
No additional notch reossification was observed in the notchplasty group, in contrast with the MRI evidence previously described in the literature [17].
MRI performed in these patients showed similar features in both groups, without evidence of progressive bony regrowth within the notch after notchplasty.
There was also no significant difference in the rate of retears, revisions for meniscectomy, or secondary cartilage repair.
One patient in each group developed a postoperative hematoma requiring surgical evacuation. In the notchplasty group, one patient presented with a postoperative popliteal aneurysm that was surgically treated. Additionally, one patient in the notchplasty group required surgery for resection of an intraosseous tibial tunnel cyst associated with a bioabsorbable interference screw (Table 3).
3.2. Functional Outcome and Return to Sport
Functional outcome data were available for 247 patients (128 in the non-notchplasty group, 119 in the notchplasty group). Forty-two patients did not complete the questionnaires despite repeated reminders and were excluded from the analysis without data imputation.
After 36 months of follow-up, there were no significant differences in functional scores (subjective IKDC, KOOS, Lysholm, Tegner, ACL-RSI) between the two groups (Table 4).
A total of 136 patients (91.3%) in the non-notchplasty group and 131 patients (93.6%) in the notchplasty group reported being satisfied or very satisfied (p = n.s.). Subjective instability was absent in 110 patients (73.8%) without notchplasty and in 104 patients (73.4%) with notchplasty.
There were no significant differences in the rate or timing of return to running, return to pivoting sports, or return to pre-injury sport participation. Performance levels were reported as the same or better than before the ACL tear in 109 patients (37.7%), with no significant differences between groups.
Among the 51 patients who stopped or changed sports, 12 did so for personal reasons unrelated to knee function. No association between the decision to stop sport and the presence or absence of notchplasty was observed.
4. Discussion
The main finding of this study was that systematic notchplasty during primary ACL reconstruction did not reduce the rate of secondary arthrolysis. Seven patients (4.7%) in the non-notchplasty group and seven patients (5.0%) in the notchplasty group required secondary arthrolysis, with no significant difference. Thus, our initial hypothesis was not confirmed.
In a series by Koga et al. [17], comparing results with and without notchplasty during double-bundle ACL reconstruction, the notchplasty group unexpectedly showed greater knee hyperextension and higher rates of secondary arthrolysis. The authors suggested that this might be explained by reossification of the notch after notchplasty.
May et al. [18], using MRI in 33 patients, observed an average of 1.5 mm of recortication at the notchplasty site within 6 months, despite a 3 mm resection in 94% of cases.
Similarly, Kitridis et al. [19] demonstrated that bone regrowth can occur after notchplasty over a 2-year CT follow-up.
Kanamiya et al. [20] reported comparable MRI findings after re-notchplasty, while Murray et al. [21] identified MRI predictors of graft maturation.
Morphological variations of the intercondylar notch have also been described by van Eck et al. [22] and Vaswani et al. [23].
Finally, Wang et al. [24] reported that notch morphology may change over time after ACL injury, potentially influencing impingement independently of notchplasty.
Small notch dimensions, as described by van Eck et al. [22] and Zhang et al. [25], are recognized as risk factors for ACL injury and impingement. Fourth, extension deficits and hamstring contracture—both known contributors to cyclops syndrome [26,27]—were not specifically evaluated. Fifth, objective laxity measurements (e.g., KT-1000 ME Dmetric Corp., San Diego, USA) were not performed, so only subjective instability could be assessed. Additionally, the exclusion of patients who did not complete postoperative questionnaires may have introduced a selection bias in the analysis of functional outcomes.
Finally, the follow-up duration differed between groups (longer in 2017 vs. 2018), but since extension deficits were always diagnosed within 6 months, this likely did not bias the main outcome.
Taken together, these findings highlight that arthrofibrosis is a multifactorial problem. Factors such as graft positioning, overtensioning, extra-articular procedures, notch morphology [25], and individual healing responses all contribute, and notchplasty alone cannot be isolated as the determining variable. Nevertheless, selective notchplasty may remain justified in specific clinical scenarios, such as patients with congenitally narrow intercondylar notches or when oversized grafts are at risk of impingement. Future studies should therefore explore targeted indications rather than systematic use.
5. Conclusions
During single-bundle primary ACL reconstruction with hamstring autografts, systematic notchplasty did not reduce the rate of secondary arthrolysis for knee extension deficit and did not alter the overall rate of complications.
Given the underpowered design and methodological limitations, our study should be considered a pilot analysis. Larger, multicenter randomized trials with selective notchplasty indications and robust adjustment for confounders are required to draw definitive conclusions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guerra-Pinto F. Thaunat M. Daggett M. Kajetanek C. Marques T. Guimaraes T. Quelard B. Sonnery-Cottet B. Hamstring Contracture After ACL Reconstruction Is Associated With an Increased Risk of Cyclops Syndrome Orthop. J. Sports Med.20175232596711668412110.1177/232596711668412128203602 PMC 5298440 · doi ↗ · pubmed ↗
- 2Lord L. Cristiani R. Edman G. Forssblad M. Stålman A. One sixth of primary anterior cruciate ligament reconstructions may undergo reoperation due to complications or new injuries within 2 years Knee Surg. Sports Traumatol. Arthrosc.2020282478248510.1007/s 00167-020-06127-w 32602035 PMC 7429539 · doi ↗ · pubmed ↗
- 3Noailles T. Chalopin A. Boissard M. Lopes R. Bouguennec N. Hardy A. Incidence and risk factors for cyclops syndrome after anterior cruciate ligament reconstruction: A systematic literature review Orthop. Traumatol. Surg. Res.20191051401140510.1016/j.otsr.2019.07.00731405748 · doi ↗ · pubmed ↗
- 4Panisset J.C. PailhéR. Schlatterer B. Sigwalt L. Sonnery-Cottet B. Lutz C. Lustig S. Batailler C. Bertiaux S. Ehkirch F.P. Short-term complications in intra- and extra-articular anterior cruciate ligament reconstruction. Comparison with the literature on isolated intra-articular reconstruction. A multicenter study by the French Arthroscopy Society Orthop. Traumatol. Surg. Res.2017103 S 231S 23610.1016/j.otsr.2017.09.00628917520 · doi ↗ · pubmed ↗
- 5Sanders T.L. Kremers H.M. Bryan A.J. Kremers W.K. Stuart M.J. Krych A.J. Procedural intervention for arthrofibrosis after ACL reconstruction: Trends over two decades Knee Surg. Sports Traumatol. Arthrosc.20172553253710.1007/s 00167-015-3799-x 26410093 PMC 4936949 · doi ↗ · pubmed ↗
- 6Hussein M. van Eck C.F. Cretnik A. Dinevski D. Fu F.H. Biomechanical Evaluation of Different Anterior Cruciate Ligament Reconstruction Techniques and Risk of Graft Impingement Am. J. Sports Med.20124081582310.1007/s 00776-009-1417-9 · doi ↗
- 7Orsi A.D. Canavan P.K. Vaziri A. Goebel R. Kapasi O.A. Nayeb-Hashemi H. The effects of graft size and insertion site location during anterior cruciate ligament reconstruction on intercondylar notch impingement Knee 20172452553510.1016/j.knee.2017.02.01028342722 · doi ↗ · pubmed ↗
- 8Sonnery-Cottet B. Archbold P. Cucurulo T. Fayard J.-M. Bortolletto J. Thaunat M. Prost T. Chambat P. The influence of the tibial slope and the size of the intercondylar notch on rupture of the anterior cruciate ligament J. Bone Jt. Surg. Br. Vol.2011931475147810.1302/0301-620X.93B 11.2690522058297 · doi ↗ · pubmed ↗