Ischemia with No Obstructive Coronary Artery Disease (INOCA): A Review
Laura Viola, Megan Masters, Umar Shafiq, Krishnam Raju Jujjavarapu, Suvitesh Luthra

TL;DR
INOCA is a condition where patients experience chest pain and heart issues without major artery blockages, making it hard to treat and diagnose.
Contribution
This review evaluates emerging surgical treatments for INOCA and emphasizes the need for personalized, multidisciplinary care.
Findings
Surgical treatments like TMR and sympathetic denervation may help reduce coronary vasospasm in refractory angina.
Early trials show promise for autologous stem cell therapy and coronary sinus occlusion in INOCA.
Selective surgical cardiac vein retroperfusion remains experimental with limited clinical evidence.
Abstract
Background: Ischemia with no obstructive coronary artery disease (INOCA) is characterized by myocardial ischemia in the absence of significant coronary artery stenosis. Despite the lack of major obstructive lesions, patients often present with chest pain, making diagnosis and management a significant challenge. Materials and Methods: A comprehensive search strategy of electronic databases (2000 to 2024) was used to identify studies assessing pathophysiology, diagnosis, surgical treatments, interventions, and outcomes in INOCA. Clinical trials, observational studies, case-control studies, and cohort studies were included. Results: Emerging surgical treatments may have a role in certain subgroups of INOCA patients, particularly those with severe and persistent symptoms or underlying pathophysiological factors that do not respond adequately to pharmacological therapies. Transmyocardial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
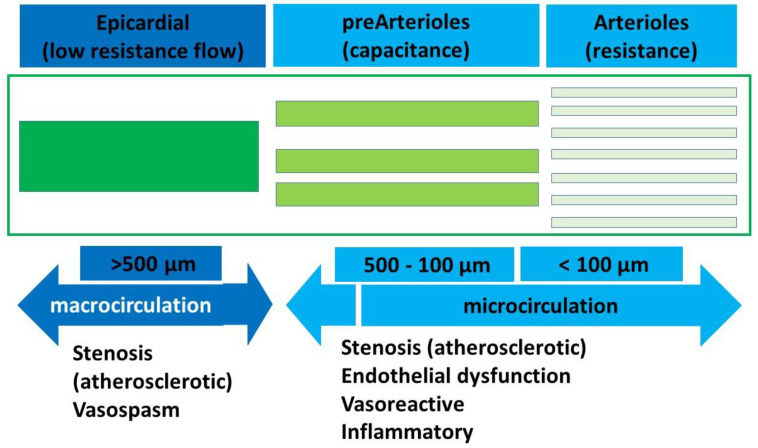 Figure 1
Figure 1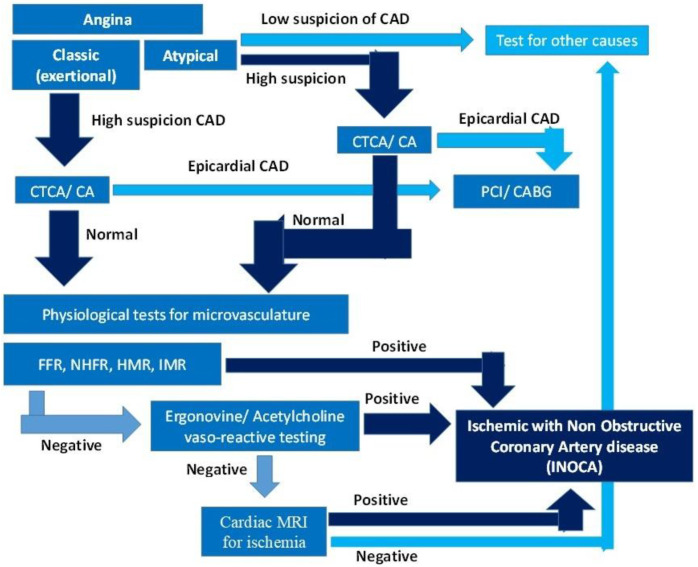 Figure 2
Figure 2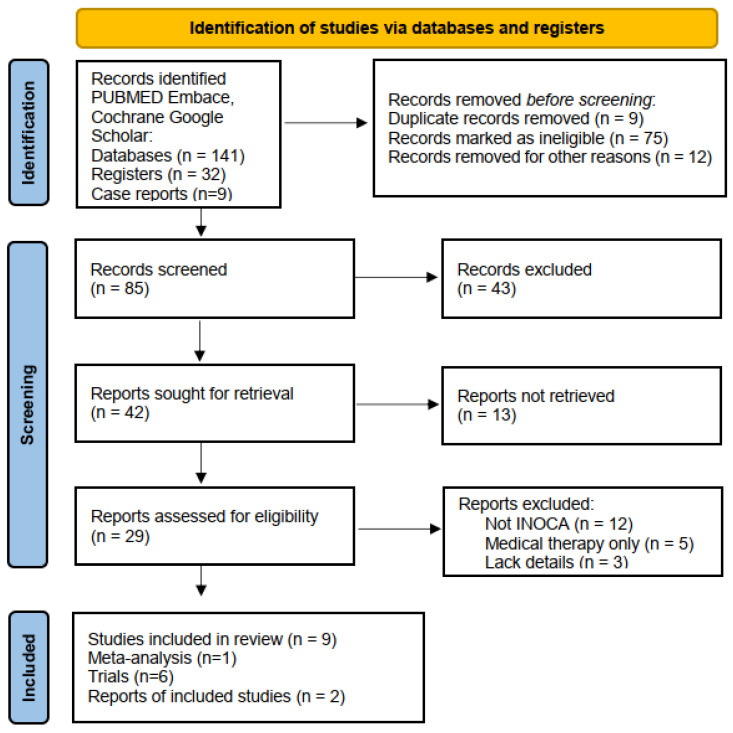 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Cardiovascular Function and Risk Factors · Heart Rate Variability and Autonomic Control
1.
Introduction
Ischemia with no obstructive coronary artery disease (INOCA) refers to a clinical condition characterized by myocardial ischemia in the absence of significant coronary artery stenosis. INOCA represents a challenge, as patients frequently present with typical ischemic symptoms such as chest pain and dyspnoea, but conventional diagnostic tests do not reveal significant lesions in the coronary arteries. These can be caused by underlying pathophysiological mechanisms, such as microvascular dysfunction, coronary vasospasm, or endothelial dysfunction, with reduced myocardial blood supply resulting in acute and chronic symptoms of ischemia [1].
The ACC National Cardiovascular Data Registry estimates that 3–4 million people have signs and symptoms of INOCA annually, with a striking female predominance [2]. Estimates are largely based on negative angiograms in patients with angina. Up to 50% of females and 7–10% of males with typical symptoms lack angiographic evidence of epicardial coronary artery disease and may have INOCA [2,3]. While traditionally overshadowed by obstructive coronary artery disease (CAD), recognition of INOCA has been increasing with advancements in diagnostic imaging techniques for coronary microcirculation and myocardial perfusion. Patients with INOCA may remain undiagnosed, leading to significant workdays lost, increased healthcare costs from further investigations, and repeated clinic/hospital attendance for unresolved symptoms. However, managing INOCA remains difficult: conventional treatments such as pharmacological therapy, lifestyle modifications, and medical management alone often fail to provide adequate relief for many patients. Emerging percutaneous nonpharmacological strategies are being explored in clinical practice and research [4].
This systematic review aims to critically evaluate the available evidence on nonpharmacological treatment options for INOCA and provide an overview of the current role of surgery in managing this complex condition. This may help refine surgical indications and improve patient outcomes in the management of INOCA.
1.1. Pathophysiology of INOCA
Microvasculature typically involves the pre-arteriolar vessels (<500 µm) and arterioles (<100 µm). The pre-arteriolar vessels are conductance vessels, and the arteriolar vessels are the resistance vessels in the coronary circulation. The pathophysiology and endotypes of INOCA can be largely divided into the putative mechanisms affecting these two groups of microvessels as obstruction, vasospasm, or a combination of the two (Figure 1,Table 1). Microvascular dysfunction, coronary vasospasm, endothelial dysfunction, and inflammation are the main recognized underlying causes of INOCA. Other less understood mechanisms include subclinical atherosclerosis, hormonal, autonomic, genetic, and environmental factors. The pathophysiology of INOCA is multifactorial; understanding these underlying mechanisms is essential for improving diagnostic accuracy and developing effective therapeutic strategies [5,6].
1.2. Diagnostic Approach to INOCA
The diagnosis of INOCA is challenging due to the lack of visible obstruction on traditional tests. Advanced diagnostic strategies are needed to assess the functionality of the coronary microcirculation, as well as to detect other possible causes of ischemia such as endothelial dysfunction or vasospasm [7,8]. There is a lack of standardization of the terminology and putative mechanisms, which limits meaningful comparison of different cohorts and treatments.
The diagnostic tools and approaches currently used to diagnose INOCA include imaging modalities and physiological tests of flow and resistance in the microcirculation, which are the mainstay for diagnosis. A diagnostic algorithm is provided in Figure 2, and the list of various tests that are used is shown in Table 2.
2. Material and Methods
A thorough search strategy was developed to locate all relevant studies. The review adhered to the PRISMA guidelines, ensuring transparency and replicability in methodology. The following electronic databases were explored for articles published between 2015 and 2024: PubMed, Embase, Cochrane Library, and Google Scholar. The search terms included various combinations of keywords such as “Ischemia with No Obstructive Coronary Artery Disease,” “INOCA,” “Microvascular Dysfunction,” “Coronary Artery Bypass Grafting,” “Percutaneous Coronary Intervention,” “Transmyocardial Revascularization,” “Stem Cell Therapy,” “Sympathectomy,” “Coronary sinus reducer”, and “Surgical Treatment in INOCA.” We aimed to identify studies that examined surgical treatment interventions, outcomes, and pathophysiology in INOCA. No limitations were applied regarding the study type, but only studies meeting the inclusion criteria were selected for further analysis. Inclusion criteria encompassed studies published in peer-reviewed journals that focused on surgical procedures or interventions for INOCA patients (ESC 2023—PRISMA diagram Figure 3). A narrative synthesis was performed from the included studies due to heterogeneity in study designs and outcomes.
2.1. Conventional Non-Surgical Treatment of INOCA
Medical therapy is the mainstay in the treatment of INOCA and aims to reduce symptoms and improve quality of life.
2.1.1. Pharmacologic Therapy
Pharmacological management of INOCA focuses to improve endothelial function, optimize coronary blood flow, and manage ischemic symptoms (Table 3). The treatment aims to increase myocardial blood supply by reducing spasm, promoting vasodilation, and to reduce myocardial oxygen demand by reducing heart rate/contractility. Preventative therapies aim to reduce the progression of the atherosclerotic burden of obstructive disease.
2.1.2. Lifestyle Modifications
Lifestyle changes help reduce the overall burden on the cardiovascular system and improve coronary microcirculation.
2.2. Nonpharmacological Treatment Options for INOCA
Surgical treatment options can be considered in specific circumstances, in which pharmacological therapy cannot control the symptoms or when microvascular dysfunction is accompanied by other coronary pathology, such as small vessel disease or epicardial vasospasm. Surgical therapy is only used as an adjunct to medical therapy and never as standalone approach due to lack of evidence. Potential surgical treatment options for INOCA are still rarely used compared to medical management. There is a lack of data on their benefits, and most of these treatments carry additional risks and complications associated with surgery, even when performed though minimally invasive approaches. There are no comparative studies to establish that one treatment may be better than another. Key studies of nonpharmacological treatments are summarized in Table 4. The strengths and limitations of the studies and their applicable groups are given in Table 5.
2.3. Transmyocardial Revascularization (TMR)
TMR is a surgical technique designed to improve myocardial perfusion, using a laser (usually a carbon dioxide (CO_2_) laser) to create small channels in the heart muscle, facilitating blood flow from the epicardial coronary vessels directly into the myocardium. TMR denervates the sympathetic nociceptors in the superficial myocardium and increases vascular endothelial growth factor (VEGF) release to induce angiogenesis [18,19]. Over time, the heart may develop collateral circulation, which can help relieve symptoms of angina and improve heart function.
TMR is typically performed with minimally invasive surgery, though it can also be performed with a traditional cardiac surgery approach. TMR has been primarily utilized for patients with advanced obstructive coronary artery disease, where traditional options like PCI or CABG were not possible. There is only limited research specifically investigating its efficacy in INOCA. In the subgroup of diabetics prone to microvascular, diffuse disease, CABG/TMR showed a greater relief of angina than CABG alone (93% vs. 63%, p = 0.02) [20]. Previously, angina relief was attributed to placebo effects, as seen with sham thoracotomies and the Vineberg procedure. Most trials have lacked controls and have focused on refractory angina patients. More research is needed to determine whether TMR has beneficial short- and long-term effects in patients with microvascular dysfunction or endothelial dysfunction associated with INOCA. Improvements in perfusion may be temporary, and it is unclear whether it can reverse the microvascular abnormalities central to INOCA. Autologous bone marrow concentrate injections in conjunction with TMR channels into targeted ischemic tissue have been hypothesized to significantly enhance the angiogenic response compared with TMR alone.
Like any surgical procedure, TMR carries risks, and for INOCA patients those risks must be carefully considered and balanced with the uncertainty of the benefits of TMR. There are additional risks of wound infection, postoperative pain, perioperative myocardial infarction, and stroke, especially in the presence of ungraftable vessels. The initial myocardial inflammation also causes an initial decrease in myocardial function, which can increase mortality in severely impaired ventricles. In the meta-analysis by Brione et al., 30-day mortality as-treated was 6.8% in the TMLR group and 0.8% in the control group (pooled OR was 3.76, 95% CI 1.63 to 8.66), largely due to crossover from standard therapy [10].
2.4. Sympathectomy
The sympathetic nervous system (SNS) plays a crucial role in regulating vascular tone, and excessive activation or dysregulation of sympathetic pathways can contribute to the development of vasospasm [21,22].
Sympathetic denervation is a surgical procedure that targets the sympathetic pathway of the autonomic nervous system to treat specific cardiovascular diseases. Sympathetic denervation blocks the sympathetic nerves in the cervical ganglions innervating the heart, which can reduce coronary artery spasm and improve myocardial perfusion.
Sympathetic denervation can be achieved through a percutaneous sympathetic nerve ablation technique or surgical sympathectomy.
2.4.1. Percutaneous Sympathetic Nerve Ablation
This minimally invasive procedure targets sympathetic nerve fibres near the coronary arteries using radiofrequency ablation or chemical neurolysis. The procedure is typically performed during coronary angiography, which allows the physician to localize the sympathetic nerve clusters and apply targeted energy or chemical agents to ablate the nerve fibres.
Radiofrequency ablation involves applying heat to selectively destroy the sympathetic nerve fibres, while chemical neurolysis uses agents such as phenol or ethanol to remove the nerves.
2.4.2. Surgical Sympathectomy
Thoracic sympathectomy involves surgically cutting sympathetic nerve pathways in the chest. While this approach has been more commonly used in other areas (e.g., for hyperhidrosis or Raynaud’s disease), it has been proposed for refractory vasospastic angina, where vasospasm is a major contributor to ischemia. This procedure is more invasive and typically considered for patients with severe, intractable symptoms that do not respond to medical treatment or percutaneous interventions [23,24].
In some cases, an endoscopic approach may be used to perform sympathetic nerve blockade around the coronary arteries.
Sympathetic denervation can be considered as a treatment option in selected patients with INOCA. Although percutaneous approaches are minimally invasive, sympathetic denervation still carries procedural risks including wound infection, pneumothorax, chylothorax, chronic wound pain, and scarring. Removing or reducing sympathetic tone may result in an imbalance in autonomic regulation, potentially leading to unwanted side effects such as bradycardia, hypotension, or decreased contractility in some cases. The long-term effectiveness of sympathetic denervation in INOCA patients remains unclear. For these reasons, sympathetic denervation for INOCA is still considered experimental and is not yet widely adopted in clinical practice. More studies are needed to validate its efficacy and safety.
2.5. Coronary Sinus Reducer
The coronary sinus reducer is an interventional device that is being explored as a possible treatment option for patients with INOCA. The coronary sinus reducer is a stainless steel, hourglass-shaped endoluminal device, which is percutaneously implanted into the coronary sinus through an expandable balloon, to increase coronary venous pressure in order to mitigate coronary microvascular resistance. The concept behind this new therapy is that elevating pressure in the coronary venous system can cause dilatation of the subendocardial arterioles, resulting in a significant reduction in vascular resistance in this area and a possible redistribution of blood flow.
A double-blind sham-controlled trial (COSIRA trial) conducted in patients with refractory angina and obstructive coronary artery disease demonstrated that the implantation of the coronary sinus reducer alleviated refractory angina symptoms and improved quality of life [11]. These findings appear to be longstanding, as the multicenter observational REDUCER-I registry consistently reported sustained improvement in angina symptoms and quality of life at three years after implantation of coronary sinus reducer in participants from the COSIRA trial [17].
Recent studies have specifically evaluated the coronary sinus reducer implants as a possible treatment for INOCA patients. A case study reported a marked reduction in angina symptoms, as well as improved global myocardial perfusion and overall quality of life in one INOCA patient six months following coronary sinus reducer implantation [13]. Furthermore, a phase II trial published by Tryon D et al. reported significant improvement in coronary blood flow, coronary flow reserve, and angina symptoms in 30 patients with INOCA following coronary sinus reducer implantation [15]. Interestingly, the recent ORBITA-COSMIC trial assessed coronary sinus reducer implants for patients with stable coronary artery disease, ischemia, and no further options for antianginal therapy. This double-blind, placebo-controlled, multicenter study found no improvement in myocardial blood flow six months after implantation, but did report significantly reduced daily angina episodes, as reported via the designated smartphone ORBITA app [16].
Trials of coronary sinus reducer for refractory angina and INOCA, including the REDUCER-I multicenter “real-world” observational registry (refractory angina), have shown sustained improvements in angina class and survival over many years. However, registry and INOCA trial data lack a control arm. INOCA trial data, however, has objective evidence of improvement in physiological tests that are markers of severity.
The ESC (2023) guidelines for chronic angina refractory to other treatments provide a Class 2b recommendation (grade of evidence B) for use of the coronary sinus reducer in experienced centers [25]. There are several ongoing randomized control trials evaluating the use of coronary sinus reducer in ANOCA/INOCA, such as Coronary Sinus Reducer for the Treatment of Refractory Microvascular Angina (COSIMA; NCT04606459), and the Efficacy of the Coronary Sinus Reducer in Patients with Refractory Angina II (COSIRA-II; NCT05102019), that may change recommendations in the future.
2.5.1.
Autologous Stem Cell Therapy
Emerging therapies, such as the use of stem cells to treat coronary microvascular dysfunction, have been investigated as potential interventions for INOCA. The main goal is to use the patient’s own stem cells to promote the repair and regeneration of damaged blood vessels.
Corban et al. (2022) reported promising improvement in coronary flow reserve, angina symptoms, and quality of life with intracoronary infusion of autologous CD34+ cells in patients with INOCA [12]. Outcomes from the IMPROvE-CED trial also demonstrated safety and efficacy, with marked improvements in angina classification and sublingual GTN usage six months following a single infusion of CD34+ cells into the left anterior descending coronary artery of 20 INOCA patients, compared to 51 historic INOCA patients on maximal medical therapy [14].
Ongoing studies such as the ESCaPE-CMD Trial and FREEDOM Trial are currently investigating the therapeutic potential, efficacy, and safety of CD34+ cell therapy.
Most trials are still in early phases, and stem cell therapy remains experimental and is not yet used in clinical practice. It is still unclear whether stem cell therapy will provide long-term benefits for patients with microvascular dysfunction or endothelial dysfunction [3]. However, stem cell therapy may have potential as an adjunct to other treatments for maximum benefit.
2.5.2.
Selective Surgical Cardiac Vein Retroperfusion
Coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) are rarely indicated in the case of INOCA, as there is no significant epicardial coronary artery stenosis.
There have been reports and case series of surgical revascularization with arterial or venous conduits of the coronary veins rather than coronary arteries, to improve myocardial perfusion retrogradely [9]. These were largely related to non-graftable coronary arteries due to diffuse disease or small vessels and did not clearly investigate or identify INOCA as the primary pathophysiology. Initial results in experimental pig models suggested that surgical venous retroperfusion of the vena cordis magna with proximal ligation and global retroperfusion with ligation of the azygous vein could improve long-term survival after acute occlusion of the left anterior descending artery [26,27]. Another similar study in pigs showed that selective cardiac venous arterialization of the left anterior descending vein and its proximal ligation after anastomosing the left internal mammary artery could reduce the infarct size by more than 50%, while protecting cardiac performance [28].
3.
Conclusions
INOCA is a complex condition that is poorly diagnosed and needs multidisciplinary management. Medical management remains the cornerstone of treatment. Selected surgical treatments are emerging as adjuncts for patients refractory to pharmacological therapy.
Among these, the coronary sinus reducer has shown improvement of symptoms and quality of life in promising early trials and may represent a minimally invasive strategy for enhancing microvascular perfusion. TMR offers potential symptomatic relief by promoting collateral circulation but currently lacks strong evidence for INOCA. Sympathetic denervation might be considered to relieve symptoms in patients with vasospastic angina but remains experimental with concerns about long-term efficacy. Targeted stem cell therapies are also emerging as potential therapies for this treatment-refractory cohort.
Most of these treatments remain experimental, and large randomized controlled trials are essential before routine clinical adoption.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kunadian V. Chieffo A. Camici P.G. Berry C. Escaned J. Maas A.H. Prescott E. Karam N. Appelman Y. Fraccaro C. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group Eur. Heart J.202041350435203262690610.1093/eurheartj/ehaa 503PMC 7577516 · doi ↗ · pubmed ↗
- 2Hansen B. Holtzman J.N. Juszczynski C. Khan N. Kaur G. Varma B. Gulati M. Ischemia with No Obstructive Arteries (INOCA): A Review of the Prevalence, Diagnosis and Management Curr. Probl. Cardiol.20234810142010.1016/j.cpcardiol.2022.10142036183980 · doi ↗ · pubmed ↗
- 3Shaw L.J. Shaw R.E. Merz C.N.B. Brindis R.G. Klein L.W. Nallamothu B. Douglas P.S. Krone R.J. Mc Kay C.R. Block P.C. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry Circulation 20081171787180110.1161/CIRCULATIONAHA.107.72656218378615 · doi ↗ · pubmed ↗
- 4Bairey Merz C.N. Pepine C.J. Walsh M.N. Fleg J.L. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade Circulation 20171351075109210.1161/CIRCULATIONAHA.116.02453428289007 PMC 5385930 · doi ↗ · pubmed ↗
- 5Del Buono M.G. Montone R.A. Camilli M. Carbone S. Narula J. Lavie C.J. Niccoli G. Crea F. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review J. Am. Coll. Cardiol.2021781352137110.1016/j.jacc.2021.07.04234556322 PMC 8528638 · doi ↗ · pubmed ↗
- 6Fu B. Wei X. Lin Y. Chen J. Yu D. Pathophysiologic Basis and Diagnostic Approaches for Ischemia With Non-obstructive Coronary Arteries: A Literature Review Front. Cardiovasc. Med.2022973105910.3389/fcvm.2022.73105935369287 PMC 8968033 · doi ↗ · pubmed ↗
- 7Benenati S. Campo G. Seitun S. Caglioni S. Leone A.M. Porto I. Ischemia with non-obstructive coronary artery (INOCA): Non-invasive versus invasive techniques for diagnosis and the role of #Full Physiology Eur. J. Intern. Med.202412715243903901110.1016/j.ejim.2024.07.017 · doi ↗ · pubmed ↗
- 8Montone R.A. CaffèA. Yasumura K. Kini A. Routine diagnosis of ANOCA/INOCA: Pros and cons Euro Intervention 202521 e 293e 29510.4244/EIJ-E-24-0007240091872 PMC 11891916 · doi ↗ · pubmed ↗