Clinical Characteristics, Treatment Approaches, and Survival Predictors in Adult Acute Myeloid Leukemia: Interim Results from the Turkish Society of Hematology AML Registry
Volkan Karakus, Ibrahim Ethem Pinar, Utku Iltar, Emel Merve Yenihayat, Merve Gokcen Polat, Serhat Celik, Umit Yavuz Malkan, Guldane Cengiz Seval, Ali Dogan, Aydan Akdeniz, Demircan Ozbalci, Idris Ince, Ramazan Erdem, Ozgur Mehtap, Hakki Onur Kirkizlar, Murat Kacmaz, Burak Deveci

TL;DR
This study analyzes clinical features, treatments, and survival in adult AML patients in Turkey, highlighting the impact of treatment intensity and patient fitness on outcomes.
Contribution
The paper provides real-world evidence from a nationwide AML registry in Turkey, emphasizing personalized treatment approaches and the role of targeted agents in less fit patients.
Findings
Intensive chemotherapy achieved higher complete remission rates compared to low-intensity regimens.
Targeted agents improved outcomes in low-intensity therapy, particularly in less fit patients.
ELN risk groups and ECOG performance status were strong predictors of survival.
Abstract
Background: Acute myeloid leukemia (AML) is an aggressive and biologically diverse hematologic cancer that disproportionately affects older individuals. Despite advances in molecular profiling and therapy, long-term outcomes remain unsatisfactory. This nationwide registry was established to provide real-world insights into clinical characteristics, treatment strategies, and survival among adult AML patients in Turkey. Methods: The Turkish AML Registry Project (ClinicalTrials.gov Identifier: NCT05979675) combines retrospective and prospective data from 23 tertiary hematology centers. Adult patients diagnosed between January 2008 and July 2023 were included. Baseline demographics, European LeukemiaNet (ELN) 2017 risk groups, Eastern Cooperative Oncology Group (ECOG) performance status, treatment intensity, and targeted therapy use were analyzed. Response and survival outcomes were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
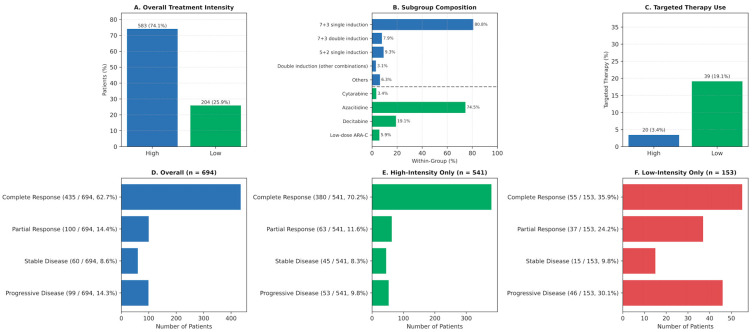 Figure 1
Figure 1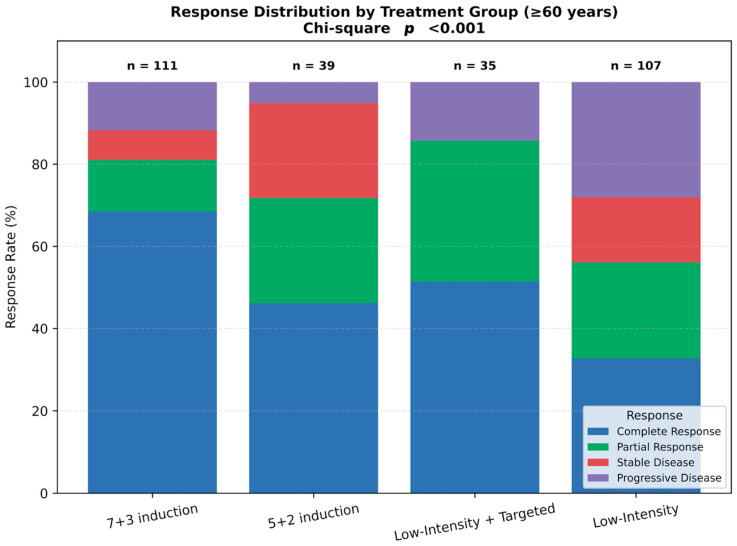 Figure 2
Figure 2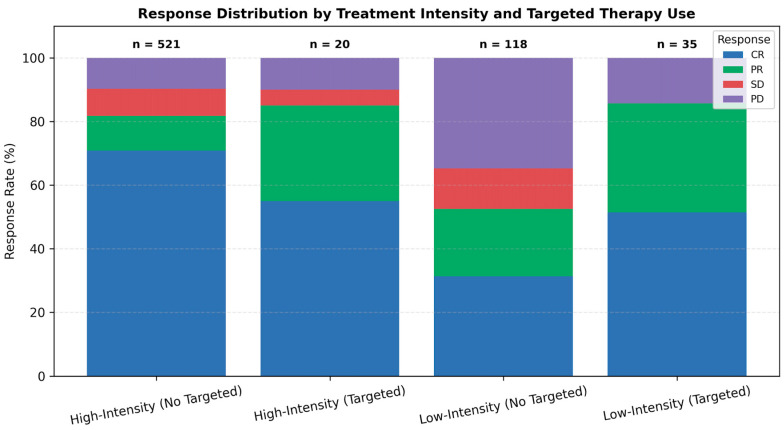 Figure 3
Figure 3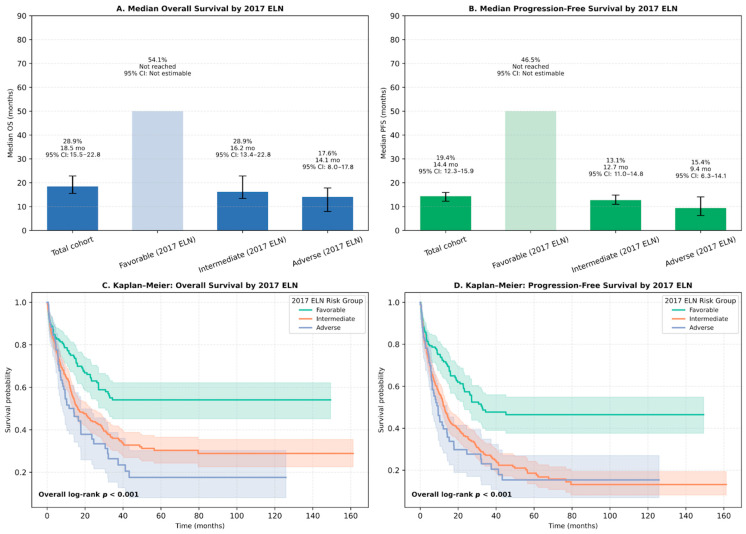 Figure 4
Figure 4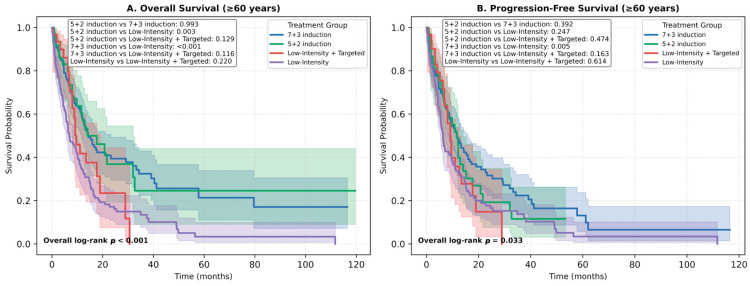 Figure 5
Figure 5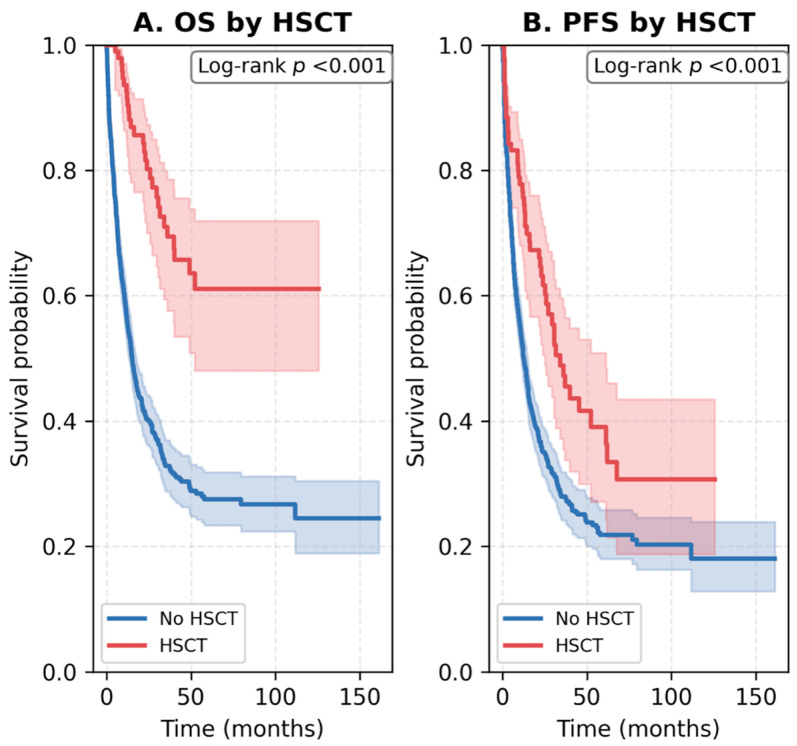 Figure 6
Figure 6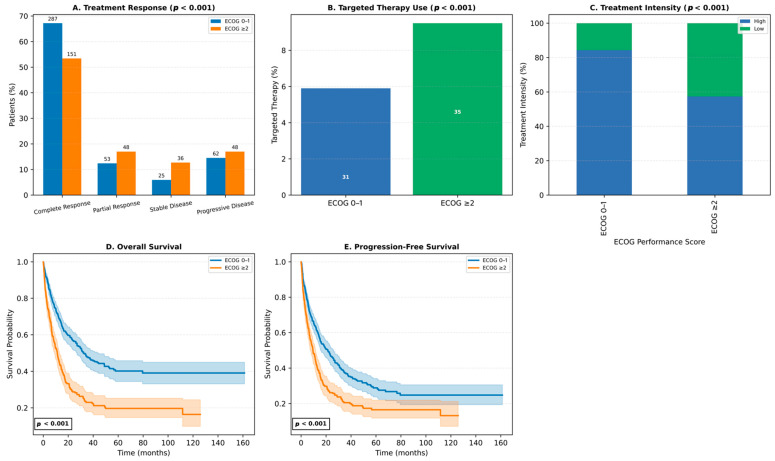 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Bone and Joint Diseases · Myeloproliferative Neoplasms: Diagnosis and Treatment
1. Introduction
Acute myeloid leukemia (AML) represents a biologically heterogeneous yet clinically aggressive myeloid neoplasm, driven by uncontrolled expansion of immature progenitor cells and most commonly encountered in older individuals [1,2]. Despite therapeutic advances, prognosis remains poor in elderly and high-risk populations, with 5-year survival rates declining steeply with age [3,4].
Over the past three decades, both the incidence and mortality of AML have increased globally, particularly among older adults [5,6]. In high-income regions such as North America and Western Europe, improved diagnostic capacity has revealed higher incidence but better outcomes, whereas survival rates remain markedly lower in low- and middle-income countries [5,7]. Among patients aged ≥60 years, 5-year survival is generally below 15%, compared with approximately 50% in younger adults [6].
Standard AML management involves induction chemotherapy—typically the intensive ‘7 + 3’ regimen—followed by consolidation with high-dose cytarabine or allogeneic hematopoietic stem cell transplantation (HSCT) in eligible cases [1,2,4,8]. For patients unfit for intensive treatment, non-intensive regimens with or without targeted therapies are used as disease-modifying approaches [1,2,8,9,10].
However, access to intensive chemotherapy, molecular diagnostics, and novel targeted agents remains heterogeneous worldwide, particularly in middle-income healthcare systems [11]. The integration of targeted therapies such as venetoclax or fms-like tyrosine kinase 3 (FLT3) inhibitors has improved remission and survival rates in unfit and older patients, yet these agents remain unavailable to many due to cost and reimbursement barriers [12,13,14].
Although complete remission (CR) is achieved in up to 70–80% of fit patients after induction, relapse or refractory disease remains common [10,15,16]. Outcomes are worse for patients receiving non-intensive treatments, with most unable to achieve durable remissions [15,16,17,18].
Moreover, disease biology—including cytogenetic and molecular risk—significantly influences prognosis and treatment response [1,3,4,8,19,20,21,22,23].
Fitness assessment remains subjective despite existing scoring systems [24], and global disparities persist in treatment accessibility due to variations in clinical practice, reimbursement, and regulatory frameworks [25].
While clinical trials have shaped current AML treatment standards, real-world outcomes often differ substantially due to broader patient heterogeneity and healthcare variability. Large-scale population-based registries from Europe and Asia have revealed lower remission and survival rates in unselected populations, driven by older age, comorbidities, and limited transplant access [7,26,27]. However, prospective real-world evidence from developing or middle-income healthcare systems remains scarce. National AML registries play a pivotal role in bridging this evidence gap by demonstrating how international guidelines are implemented in routine clinical practice under heterogeneous healthcare conditions [28].
In this context, establishing a national AML registry represents a crucial step toward generating real-world evidence in Turkey. Designed as a nationwide initiative, the Turkish AML Registry Project integrates data from multiple treatment environments to reflect real-world management practices. The present interim evaluation provides an overview of demographic and clinical profiles, therapeutic patterns, and one-year outcomes among adults diagnosed with AML in Turkey. In light of expanding targeted therapy options [1,29,30,31,32,33,34], this study highlights critical associations between treatment intensity, Eastern Cooperative Oncology Group (ECOG) performance status, European LeukemiaNet (ELN) risk classification, and survival outcomes, aiming to inform context-specific, personalized care strategies in AML.
2. Methods
2.1. Study Design and Population
This study is a nationwide, multicenter, non-interventional observational registry combining retrospective and prospective data collection (ClinicalTrials.gov Identifier: NCT05979675), conducted across 23 tertiary hematology centers in Turkey.
The retrospective phase included adult patients diagnosed with AML between January 2008 and June 2022, with anonymized data collected from institutional medical records, as approved by the Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee (Approval Date: 3 September 2021, Protocol No: E-108400098-772.02-4214).
The prospective phase was launched in June 2022 and is designed for a 5-year follow-up period (June 2022–June 2026). This phase received approval from the Istanbul Medipol University Clinical Research Ethics Committee (Approval Date: 21 February 2022, Protocol No: E-66291034-772.02-1237) and from the Republic of Turkey Ministry of Health Turkish Medicines and Medical Devices Agency (Approval Date: 14 April 2022, Protocol No: 202105019).
The present interim analysis includes baseline characteristics and 1-year outcomes of retrospectively and prospectively enrolled patients, with data collected up to July 2023. Survival analyses accounted for variable follow-up durations through right-censoring.
A total of 906 adult patients diagnosed with AML were initially identified. After excluding 15 patients due to incomplete clinical data, 891 patients were included in the final analysis. The median age at diagnosis was 58 years (range, 18–91), and 54.9% were male.
The study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all prospectively enrolled participants.
Genomic analyses were performed locally at participating institutions without central review, reflecting real-world diagnostic practice.
2.2. Data Collection and Definitions
Baseline demographic and clinical data included age, gender, AML subtype (according to the World Health Organization classification, WHO), ECOG performance status, ELN 2017 genetic risk classification [19], presence of extramedullary disease, and molecular status for FLT3-internal tandem duplication (FLT3-ITD) and nucleophosmin 1 (NPM1) mutations.
The treating physician determined the ECOG performance status at the time of AML diagnosis. Cytogenetic and molecular evaluations were carried out using bone marrow aspirates or, when applicable, peripheral blood samples obtained before initiation of induction therapy. Molecular analyses relied on institution-specific polymerase chain reaction (PCR) assays or next-generation sequencing (NGS) panels that had undergone local validation, whereas chromosomal abnormalities were identified through conventional karyotyping and fluorescence in situ hybridization (FISH) according to standard laboratory procedures.
Molecular analyses were conducted according to the diagnostic capacity of each participating center. FLT3 and NPM1 were the most frequently assessed markers, while additional genes—including IDH1/2, TP53, RUNX1, ASXL1, CEBPA, KIT, and KMT2A—were tested in centers equipped with PCR or NGS facilities. Cytogenetic abnormalities such as t(8;21), inv(16)/t(16;16), t(15;17), del(17p), and other recurrent aberrations were identified by conventional karyotyping, FISH, or narrative cytogenetic reports. Given the real-world nature of the registry, testing coverage varied across centers and over time; missing molecular data were not imputed.
Treatment-related variables included induction regimen intensity (high-intensity vs. low-intensity), use of targeted agents (e.g., venetoclax, midostaurin, gemtuzumab ozogamicin, sorafenib). The distribution of targeted agents across treatment intensities is presented in Supplementary Figure S1.
Treatment response was categorized as CR, partial response (PR), morphologic leukemia-free state, stable disease (SD), or progressive disease (PD), based on ELN 2017 response criteria. Overall survival (OS) represented the interval between initial diagnosis and either death from any cause or the date of last contact. Progression-free survival (PFS) was calculated from diagnosis until documented relapse, disease advancement, or death, whichever occurred first.
2.3. AML Subtypes and Risk Stratification
AML subtypes were classified according to the 2016 WHO criteria [8,35]. Risk stratification was performed in accordance with the 2017 ELN recommendations, categorizing patients into favorable, intermediate, and adverse genetic risk groups [19,36]. ELN categories were assigned using the available molecular and cytogenetic results for each patient, consistent with real-world registry practice. Missing molecular data were not imputed to preserve data integrity.
2.4. Statistical Analysis
Baseline characteristics were analyzed through descriptive statistical methods. Categorical variables were summarized as absolute frequencies and percentages, whereas continuous variables were described using medians with their corresponding ranges. Associations between categorical parameters were examined with the chi-square (χ^2^) test, and non-parametric group differences were evaluated using the Mann–Whitney U test.
Survival probabilities were estimated by the Kaplan–Meier approach, and intergroup differences were compared using the log-rank test. Where appropriate, pairwise and multivariate log-rank analyses were additionally conducted. Statistical significance was determined at a two-sided p value threshold of 0.05.
Analyses were conducted using Python (v3.13.2; Clang 16.0.0) in a virtual environment on macOS. Data preprocessing and transformation were performed with pandas, while survival modeling and statistical plotting utilized lifelines, matplotlib, and scipy.
3. Results
3.1. Patient Characteristics
The analysis encompassed 891 adults diagnosed with AML. Patients had a median age of 58 years (range 18–91), and slightly more than half of the cohort (54.9%) were men. According to WHO classification, AML not otherwise specified was the most prevalent subtype (55.8%), followed by AML with recurrent genetic abnormalities (17.6%) and AML with myelodysplasia-related changes (15.4%) (Table 1). Extramedullary involvement was documented in 4.4% of patients. Based on the 2017 ELN risk classification, 24.7% of patients were categorized as favorable-risk, 60.8% as intermediate-risk, and 14.5% as adverse-risk. At diagnosis, 63.1% of patients had an ECOG performance status of 0–1, while 36.9% were ECOG ≥ 2. In patients for whom molecular results were available, FLT3-ITD mutations were identified in 15.7% and NPM1 mutations in 20.1% of cases.
Beyond FLT3-ITD and NPM1, additional molecular and cytogenetic analyses were performed according to the diagnostic capacity of participating centers. IDH1/2, TP53, RUNX1, ASXL1, CEBPA, KIT, and KMT2A mutations were assessed in a subset of patients with available PCR or NGS testing, while recurrent cytogenetic abnormalities such as t(8;21), inv(16)/t(16;16), t(15;17), and del(17p) were detected by karyotyping, FISH, or narrative cytogenetic reports.
The frequency of tested patients and detected abnormalities for each marker is summarized in Supplementary Table S1, which reflects real-world heterogeneity in genomic testing coverage across the 23 centers.
3.2. Treatment Distribution and Targeted Therapy Use
Of the cohort, 74.1% received high-intensity induction therapy, while 25.9% were treated with low-intensity regimens (Figure 1A). Among high-intensity protocols, 7 + 3 single induction was dominant (80.8%), whereas azacitidine was the leading agent in low-intensity regimens (74.5%), followed by decitabine (19.1%) (Figure 1B). Targeted therapies were more frequently administered in patients receiving low-intensity regimens (19.1%) than those on high-intensity protocols (3.4%) (p < 0.001; Figure 1C), reflecting a clinical preference for integrating targeted agents in older or frail individuals. Subgroup distribution by regimen is shown in Supplementary Figure S1.
3.3. Response Rates
Treatment response differed significantly by intensity (p < 0.001). CR was achieved in 70.2% of patients on high-intensity regimens compared to 35.9% of those receiving low-intensity therapies. PD occurred in 30.1% of low-intensity patients versus 9.8% in the high-intensity group. PR and SD rates also favored high-intensity therapy (11.6% vs. 24.2% for PR; 8.3% vs. 9.8% for SD) (Figure 1E,F).
Stratifying by both intensity and targeted agent use, marked differences in response were observed (Figure 2). In the low-intensity group, adding targeted therapy improved CR rates from 35.9% to 51.4% and halved the PD rate from 30.1% to 14.3%. A similar but less pronounced benefit was seen in the high-intensity cohort. These differences were statistically significant (p < 0.001), emphasizing the additive impact of targeted therapy on disease control.
In participants aged ≥60 years, response distributions varied significantly across regimens (p < 0.001; Figure 3). The 7 + 3 induction group demonstrated the highest CR rate, while low-intensity plus targeted therapy yielded favorable response profiles with minimal progression. In contrast, low-intensity non-targeted regimens were associated with the highest rates of PD and SD. These findings highlight how treatment strategies are individualized according to patient age and fitness in real-world clinical practice.
3.4. Survival Outcomes
Outcomes stratified by ELN 2017 classification revealed substantial differences. Patients in the favorable-risk group had a 1-year OS rate of 54.1%, with median OS not reached (95% CI: 30.8–NA), whereas intermediate- and adverse-risk patients had 1-year OS rates of 28.9% and 17.6%, and median OS of 16.2 months (95% CI: 13.4–22.8) and 14.1 months (95% CI: 8.0–17.8), respectively (log-rank p < 0.001; Figure 4A–C). Similarly, 1-year PFS was 46.5% in favorable-risk patients (median PFS: 32.6 months), compared to 13.1% and 15.4% in intermediate- and adverse-risk groups (median PFS: 12.7 and 9.4 months, respectively) (log-rank p < 0.001; Figure 4B–D).
Among elderly patients (≥60 years), 1-year OS rates were 54.2% for 7 + 3 induction, 52.3% for 5 + 2 induction, and 48.5% for low-intensity targeted therapy, compared to only 31.4% for non-targeted low-intensity regimens. Median OS ranged from 17.6 months in the 7 + 3 group to 8.6 months in the low-intensity non-targeted group (Figure 5A,B).
The impact of allogeneic HSCT on survival outcomes was analyzed within the study cohort. Among all 891 patients, 99 (11.1%) underwent allogeneic HSCT, predominantly within the high-intensity group (18.9% in 7 + 3 induction), while no HSCT was performed among patients treated with low-intensity regimens. In patients aged ≥60 years, only 15 (3.8%) underwent HSCT, reflecting real-world limitations in transplant eligibility due to age and comorbidities. Transplanted patients achieved markedly improved survival compared with those who did not undergo HSCT. Median OS was not reached in the HSCT group versus 15.1 months in the non-HSCT group (log-rank p < 0.001), and median PFS was 34.1 versus 12.6 months, respectively (log-rank p < 0.001). These findings are illustrated in Figure 6.
3.5. Impact of ECOG Performance Status
Baseline ECOG status was a major determinant of treatment patterns and outcomes. Patients with ECOG 0–1 had higher CR rates (67.2%) and lower PD rates (14.5%) than those with ECOG ≥ 2 (CR: 53.4%, PD: 17.0%) (Figure 7A). Targeted therapies were used more frequently in ECOG ≥ 2 patients (8.7% vs. 5.2%), indicating a shift toward personalized treatment in frailer individuals (Figure 7B). High-intensity regimens were administered to 71.6% of ECOG 0–1 patients, but only 52.0% of those with ECOG ≥ 2, who were more often treated with low-intensity regimens (38.7%) (Figure 7C).
ECOG performance status also correlated with survival. Patients with ECOG 0–1 had superior outcomes, with a 1-year OS rate of 70.3% and median OS of 32.2 months, compared to 47.0% and 11.2 months in the ECOG ≥ 2 group. Similarly, 1-year PFS was 62.6% vs. 42.7%, with median PFS of 21.5 vs. 9.5 months (Figure 7D,E). These results underscore the prognostic significance of ECOG status in guiding treatment intensity and anticipating survival outcomes in AML.
4. Discussion
This interim prospective analysis of the Turkish AML Registry presents a comprehensive real-world overview of adult AML treatment strategies and clinical outcomes in a large, multicenter national cohort. The findings highlight how treatment intensity, risk classification, and targeted therapy use influence outcomes in routine practice. Notably, intensive regimens achieved higher remission rates, while the addition of targeted agents substantially improved responses in patients receiving low-intensity therapy.
Our results should be interpreted within the broader context of international real-world evidence. While clinical trials predominantly include younger and fitter patients, population-based registries have consistently shown lower remission and survival rates in unselected cohorts, largely driven by older age, comorbidities, and limited transplant access [26,37]. Such real-world datasets complement clinical trials by reflecting treatment heterogeneity and healthcare disparities encountered in daily practice. National AML registries, including those in Sweden, Denmark, Germany, Korea, and now Turkey, provide valuable insights into how evidence-based recommendations are implemented across diverse healthcare systems [7,27].
The CR rates observed in our cohort are comparable to those reported in clinical trials evaluating novel targeted therapies, suggesting that these treatments can achieve similar efficacy in a real-world setting [30,38,39,40,41,42]. However, several real-world studies have highlighted the limitations of low-intensity regimens in elderly AML patients. A multicenter cohort study involving patients aged 60–75 years reported that intensive chemotherapy was associated with significantly longer OS compared to venetoclax plus hypomethylating agent combinations [43]. Similarly, hypomethylating agents alone yielded modest overall response rates of 15–20%, with median OS ranging from 7.7 to 24.5 months [18,44,45]. In contrast, our cohort demonstrated a 1-year OS of 48.5% in patients aged ≥60 years treated with low-intensity regimens plus targeted therapy, significantly higher than the 31.4% in those without targeted agents. Additionally, retrospective analyses in relapsed/refractory AML have demonstrated that both intensive and non-intensive treatments offer a survival advantage over best supportive care [16].
Age remains one of the strongest prognostic indicators in AML, with population-based data showing a 5-year OS of approximately 58% for patients diagnosed before age 40, decreasing by nearly 10% with each subsequent decade [3,23,46]. In our cohort, age ≥ 60 years, ECOG performance status ≥ 2, and adverse or intermediate ELN risk were associated with reduced OS, consistent with prior population-based studies [3,22,23,47]. Although intensive chemotherapy is typically investigated in younger cohorts and reserved for older individuals deemed fit for aggressive treatment [31], our findings revealed that 74.1% of patients underwent intensive induction despite nearly half (45.5%) being aged 60 years or older. This suggests that clinicians’ assessments of patient fitness and initial treatment decisions for AML in community practices may differ from those in clinical trials among selected patients [24,31,48]. Supporting data from other registry-based subgroup analyses in Turkey have shown consistent CR rates with 7 + 3 induction in newly diagnosed patients, and improved outcomes with azacitidine–venetoclax combinations in unfit patients [49,50].
The diverse outcomes in AML patients highlight the critical role of cytogenetic and molecular markers in identifying high-risk patients for relapse and those who may benefit from personalized treatment approaches. Several mutations either respond to specific therapies or present opportunities for targeted interventions [30,32]. Recently, the United States Food and Drug Administration approved several oral targeted therapies for AML management, guided by specific genetic and molecular profiles [30,31]. These therapies are increasingly being utilized as frontline treatments for cases who are ineligible for intensive chemotherapy, as well as in salvage therapy for relapsed or refractory disease, demonstrating better outcomes compared to previous standards of care [1,29,30,31].
In our cohort, the median OS was 27.2 months, aligning with outcomes reported in recent clinical trials evaluating targeted therapies in AML [38,39,42,51,52]. Interestingly, a single-center, retrospective study of 127 AML patients aged 60–75 at diagnosis found no notable difference in OS between those receiving high-intensity chemotherapy and those treated with low-intensity targeted therapy [30].
It is also important to recognize the contextual relevance of our findings. In developing or middle-income countries, AML outcomes remain significantly inferior to those in high-income settings due to delayed diagnosis, limited access to molecular testing, and uneven availability of novel agents [28,53]. Real-world national registries, such as the Turkish AML Registry, are therefore essential for identifying practice gaps, informing healthcare policy, and guiding the equitable implementation of modern AML therapies.
This interim analysis, with a median follow-up of 12.0 months, highlights the potential impact of extended follow-up on survival outcomes. For instance, data from the Italian Compassionate Use Program reported a 1-year OS rate of 68.6% with an initial follow-up of 11 months. However, the median OS was just 13 months, and the estimated 2-year OS rate significantly declined to 29% after 22 months of follow-up [54,55,56]. While novel targeted agents have improved response rates and survival in AML, they are not considered curative on their own. Allogeneic HSCT remains a key potentially curative option, particularly for patients with ELN intermediate- or adverse-risk disease and those with relapsed or refractory AML [30]. In real-world settings, the proportion of patients undergoing HSCT varies but is generally comparable to or even higher than in clinical trials, especially with increased use of targeted agents such as CPX-351 (liposomal cytarabine-daunorubicin combination) [54,56,57,58].
In this real-world AML registry, 11.1% of patients underwent allogeneic HSCT, predominantly following intensive induction therapy. This rate parallels global real-world data, where HSCT utilization ranges from 18–40% in high-income and 3–6% in low- to middle-income countries [59,60]. Transplanted patients achieved markedly better outcomes, consistent with meta-analyses showing that HSCT in CR significantly improves OS and PFS compared with consolidation chemotherapy [61,62,63]. In older adults, reduced-intensity conditioning offers feasible survival benefits while minimizing toxicity [64,65]. Despite promising responses with venetoclax-based regimens, long-term survival remains superior with HSCT, particularly in high-risk or minimal residual disease (MRD)-positive AML [12,66]. Collectively, these findings affirm the central role of HSCT as a curative consolidation approach in appropriately selected AML patients.
Regional and center-specific variations in patient selection and transplant referral practices strongly influence allogeneic HSCT rates across real-world cohorts. In a subgroup analysis involving patients with newly diagnosed AML from the Turkish AML Registry Project database, allogeneic HSCT was performed in 10.9% of participants treated with idarubicin and 26.2% of those treated with daunorubicin, whereas no patients in the mitoxantrone group proceeded to allogeneic HSCT [49]. These findings highlight the need for more consistent and standardized approaches to transplant eligibility and referral in routine clinical practice.
Receipt of allogeneic HSCT, a well-established determinant of survival in AML, may be limited by limited early access to targeted therapies in certain settings, including our country. This is particularly relevant given the suggested link between these therapies and improved feasibility of undergoing allogeneic HSCT [54,58]. However, previous studies indicate that survival rates are similar for AML patients who undergo induction therapy followed by transplantation, regardless of whether remission is achieved through intensive chemotherapy or targeted treatments [30,67,68,69]. The essential role of transplantation in older adults remains paramount, irrespective of the treatment intensity employed to achieve a response [30,56,70]. According to a recent investigation by the Center for International Blood and Marrow Transplant Research, which evaluated prognostic factors influencing post-transplant outcomes in AML patients aged 60 years or older, chronological age alone does not hinder successful transplantation and should not exclude patients from allogeneic HSCT [71].
Several limitations should be acknowledged. As an interim analysis, the study is limited to 1-year outcomes and does not yet include post-relapse survival or long-term HSCT follow-up. Additionally, performance status and treatment intensity were not randomized, introducing potential selection bias. However, the large sample size, prospective design, and multicenter nature enhance the generalizability and relevance of our findings.
Future research should focus on integrating comprehensive genomic, clinical, and health-system data to refine personalized risk stratification in AML. Expanded national registries with standardized NGS and MRD assessment will be critical to validate the prognostic value of the 2022 ELN classification across age and fitness subgroups. Building on multicenter experience from the Turkish AML Registry, where molecular testing and access to FLT3-targeted therapy were heterogeneous, forthcoming phases should emphasize centralized genomic analysis, harmonized MRD monitoring, and systematic evaluation of real-world access barriers [72]. Such efforts will enable predictive modeling to guide treatment intensity and transplant selection, while supporting equitable implementation of novel AML therapies in middle-income healthcare systems.
5. Conclusions
In conclusion, this nationwide real-world study offers valuable insights into current AML treatment patterns and survival predictors in Turkey. High-intensity chemotherapy remains the most effective approach for eligible patients, but low-intensity regimens combined with targeted agents provide meaningful benefit in selected subgroups. ECOG performance status and ELN risk classification continue to play pivotal roles in guiding treatment intensity and anticipating prognosis. As the AML therapeutic landscape evolves, real-world evidence from prospective registries will be critical to optimizing personalized care and informing national treatment frameworks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Di Nardo C.D. Erba H.P. Freeman S.D. Wei A.H. Acute myeloid leukaemia Lancet 20234012073208610.1016/S 0140-6736(23)00108-337068505 · doi ↗ · pubmed ↗
- 2Shimony S. Stahl M. Stone R.M. Acute myeloid leukemia: 2023 update on diagnosis, risk-stratification, and management Am. J. Hematol.20239850252610.1002/ajh.2682236594187 · doi ↗ · pubmed ↗
- 3National Cancer Institute SEER Cancer Stat Facts: Acute Myeloid Leukemia Available online: https://seer.cancer.gov/statfacts/html/amyl.html(accessed on 4 August 2024)
- 4Talati C. Sweet K. Recently approved therapies in acute myeloid leukemia: A complex treatment landscape Leuk. Res.201873586610.1016/j.leukres.2018.09.00130223250 · doi ↗ · pubmed ↗
- 5Chen P. Liu X. Zhao Y. Hu Y. Guo J. Wang H. Global, national, and regional burden of acute myeloid leukemia among 60–89 years-old individuals: Insights from a study covering the period 1990 to 2019 Front. Public Health 202411132952910.3389/fpubh.2023.132952938274540 PMC 10808630 · doi ↗ · pubmed ↗
- 6Yi M. Li A. Zhou L. Chu Q. Song Y. Wu K. The global burden and attributable risk factor analysis of acute myeloid leukemia in 195 countries and territories from 1990 to 2017: Estimates based on the global burden of disease study 2017 J. Hematol. Oncol.2020137210.1186/s 13045-020-00908-z 32513227 PMC 7282046 · doi ↗ · pubmed ↗
- 7Han H.J. Choi K. Suh H.S. Impact of aging on acute myeloid leukemia epidemiology and survival outcomes: A real-world, population-based longitudinal cohort study P Lo S ONE 202419 e 030063710.1371/journal.pone.030063738771863 PMC 11108202 · doi ↗ · pubmed ↗
- 8Pollyea D.A. Altman J.K. Assi R. Bixby D. Fathi A.T. Foran J.M. Gojo I. Hall A.C. Jonas B.A. Kishtagari A. Acute myeloid leukemia, version 3.2023, NCCN clinical practice guidelines in oncology J. Natl. Compr. Cancer Netw.20232150351310.6004/jnccn.2023.002537156478 · doi ↗ · pubmed ↗