Early Use of Cryoprecipitate Versus Plasma and Clinical Outcomes in Major Spine Surgery
Aparna Depuru, Jong Ok La, Miriam M. Treggiari, Nicole R. Guinn

TL;DR
This study compares cryoprecipitate and plasma use in spine surgery patients and finds similar outcomes except for better home discharge rates with cryoprecipitate.
Contribution
The study provides new insights into the clinical outcomes of using cryoprecipitate versus plasma in managing coagulopathy after major spine surgery.
Findings
Cryoprecipitate was associated with higher odds of home discharge compared to plasma.
No significant differences were found in mortality or ICU length of stay after adjusting for confounders.
Univariable analysis suggested lower 1-year mortality with cryoprecipitate, but this was not significant in multivariable analysis.
Abstract
Background/Objectives: Major spine surgery often leads to significant blood loss and coagulopathy, necessitating blood product transfusion. Cryoprecipitate and plasma are two blood products commonly used to manage coagulopathy, but outcomes associated with their use in spine surgery remain unclear. Methods: This retrospective cohort study included adult patients undergoing major spine surgery from 2015 to 2022 within a single health system. Included patients received at least one unit of packed red blood cells (PRBCs) followed by either cryoprecipitate or plasma to investigate the treatment of coagulopathy after blood loss. Study endpoints included hospital length of stay (H-LOS), ICU length of stay (ICU-LOS), discharge disposition, one-year mortality, and total blood products transfused up to postoperative day (POD) 2. Multivariable linear and logistic regression was used to estimate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
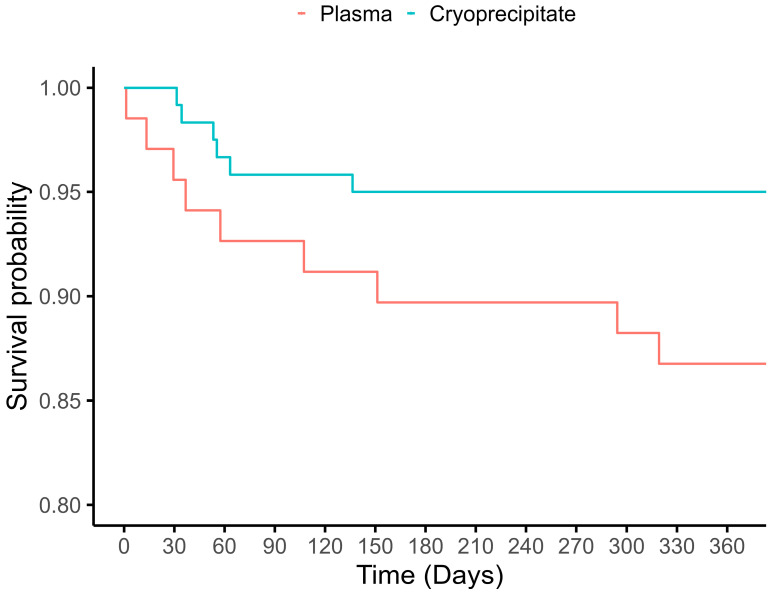 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Hematological disorders and diagnostics · Spinal Hematomas and Complications
1. Introduction
Major spine surgery is often associated with significant blood loss due to the extensive muscle and bone dissection and instrumentation needed for exposure, frequently necessitating transfusion to manage acute anemia [1]. Blood losses and subsequent transfusion of allogeneic red blood cells and/or cell-salvaged blood can cause significant dilution of coagulation factors, which may further contribute to blood losses and ongoing requirement for transfusion of other blood products [2].
While cryoprecipitate and plasma are both used to manage coagulopathy, they differ significantly in volume, composition, and mechanism of action. Plasma is sourced from human donors and contains albumin, coagulation factors, immunoglobulins, and acute-phase proteins. An alternative to plasma to treat coagulopathy related to low fibrinogen is cryoprecipitate, which is derived from plasma and is high in fibrinogen, factor VIII, factor XIII, and von Willebrand factor (VWF) [3]. Transfusion of plasma is associated with potential risk of infection, hemolysis, anaphylaxis, and transfusion-associated circulatory overload [4,5,6]. Cryoprecipitate, which has less volume than plasma, may reduce the risk of transfusion-associated circulatory overload and more promptly restore fibrinogen and has been associated with lower mortality in patients undergoing cardiac surgery [7], whereas transfusion of plasma has been associated with higher mortality in the same population [8]. In spine surgery, use of plasma has been associated with a higher risk of infection and longer hospital length of stay, as well as renal, ischemic, and thrombotic complications [9].
While the adoption of viscoelastic testing (VET) has been associated with a reduction in plasma usage and earlier, more frequent use of cryoprecipitate compared to management guided by conventional laboratory assessments, including in major spine surgery [10], limited research describes outcomes of early use of cryoprecipitate versus plasma in spine surgery. Due to scarce data, coagulopathy management varies widely, driven by provider preference and product availability.
Although plasma and cryoprecipitate have distinct indications, plasma for broad coagulation factor replacement and cryoprecipitate primarily for fibrinogen supplementation, there remains real-world variability in empiric transfusion practices during major spine surgeries. In settings where VET is unavailable, clinicians rely on clinical judgment, with preferences varying between plasma and cryoprecipitate. Additionally, with the potential for rapid blood loss during major spine surgery and the delay in obtaining laboratory results, blood products are often given empirically based on suspicion of clinical coagulopathy. This variation is common, especially in community hospitals or institutions without standardized protocols.
We conducted a cohort study of patients undergoing major spine surgery at a single health system who experienced blood loss requiring packed red blood cell (PRBC) transfusion, followed by at least one unit of either cryoprecipitate or plasma, to compare clinical outcomes based on the first used product for treatment of blood loss-associated coagulopathy.
2. Materials and Methods
2.1. Study Population
After Institutional Review Board approval (Protocol 00112563, approved 12/2023), we conducted a retrospective review of all adults (age ≥ 18 years) patients undergoing major spine surgery (CPT codes: 22800, 22802, 22804, 22808, 22810, 22812, 22206-8, and 22842-7) between 2015 and 2022 within a single health system (including one academic hospital and two community hospitals). Patients who received at least one unit of PRBCs followed by at least one unit of either cryoprecipitate (given as a pool of 5) or plasma in the operating room (between anesthesia start and anesthesia stop) were included to reflect a population of patients with suspected coagulation abnormalities in the setting of intraoperative bleeding.
2.2. Study Exposure and Endpoints
The study exposure was determined based on the first product that was received after at least one unit of the PRBCs. Patients were then assigned to either the cryoprecipitate group or the plasma group. The study endpoints were the length of hospital stay (H-LOS), length of ICU stay (ICU-LOS) among the patients admitted to the ICU, hospital discharge disposition, 1-year mortality, and total blood products transfused after meeting inclusion criteria (excluding any PRBCs before first cryoprecipitate or plasma and first unit of cryoprecipitate or plasma) up to postoperative day (POD) 2 as a short-term bleeding outcome.
2.3. Data Collection
Data were extracted from the electronic health record. Variables collected were patient demographics including age; sex; race; height; weight; smoking status; co-morbidities and American Society of Anesthesiologists (ASA) status; preoperative and intraoperative laboratory studies; and procedural information, including hospital location, surgical service line (neurosurgery or orthopedics), case length, use of tranexamic acid, use of cell salvage blood, estimated blood loss (EBL), and total units of PRBCs, platelets, plasma, and cryoprecipitate transfused intraoperatively and postoperatively. A chart review was performed among patients who died to determine the probable cause of death.
2.4. Anesthetic and Surgical Management
Restrictive transfusion practices are generally recommended across the health system, including giving single units of PRBCs at a time and using a hemoglobin trigger of 7–8 g/dL in stable, non-hemorrhaging patients. For non-PRBC transfusion, laboratory values generally guide transfusion decisions (fibrinogen < 150–200 mg/dL, platelets < 100 (×10^9^/L), INR > 1.5), although decisions to transfuse are multifactorial, depending on patient condition and left to the individual providers. Use of other blood management techniques, including cell salvage and antifibrinolytics, is requested by the surgeons, generally when anticipated EBL is greater than 1 L. When used, antifibrinolytics were started at the incision. Use of VET is available and encouraged at the university hospital, using ROTEM (Company: Werfen, Bedford, MA, USA) but not available at either of the two community hospitals.
2.5. Statistical Analyses
Median (IQR) was used to summarize continuous variables, and counts (percentages) were used for categorical variables. The study endpoints were compared between patients receiving cryoprecipitate as first-line with plasma as first-line. H-LOS and ICU-LOS were log-transformed and analyzed using a multivariable linear regression model. Discharge disposition (home independently vs. a disposition to other facility or needing assistance) and 1-year mortality were analyzed using multivariable logistic regression models. Total blood products transfused after meeting inclusion criteria up through POD2 were analyzed using Wilcoxon rank sum test, and results were reported as mean differences (MDs) with 95% confidence intervals. We first fitted univariable regression models, then we fitted multivariable models adjusting for age, sex, BMI, ASA status, use of tranexamic acid (yes/no), and hospital setting (academic versus community) for each of the study endpoints. Additionally, we conducted a subgroup analysis of patients who received cryoprecipitate versus those who received only plasma. Univariable and multivariable analyses were performed on the subgroup as described for the primary analysis. Results of the log-transformed outcome linear regression model are reported as ratios of geometric means (GMR) with 95% CI, and the results of the logistic regression model are reported as odds ratios (ORs) with 95% CIs. A two-sided alpha level of less than 0.05 was considered statistically significant. All statistical analysis was conducted by the study biostatistician (J.O.L.) using R version 4.4.0.
3. Results
3.1. Patient Demographic and Baseline Characteristics
Our initial query identified a cohort of 14,256 adult patients who underwent spine surgery. Of those, 585 received PRBCs intraoperatively, and 189 patients met the inclusion criteria, with 120 receiving cryoprecipitate and 69 receiving plasma as a first-line product following the transfusion of at least one unit of PRBCs in the operating room. Table 1 shows the baseline characteristics of the study population. The two groups were comparable for age, race, sex, BMI, co-morbidities, ASA status, and preoperative laboratory values. Hypertension was slightly more common in the cryoprecipitate group, and neurosurgery cases were more frequent, while orthopedic cases predominated in the plasma group.
3.2. Intraoperative Blood Product Transfusion Patterns
The total number of intraoperative PRBCs transfused was similar between the two groups, with a median of 3 units (IRQ: 2–5) for the cryoprecipitate group compared to 4 units (IRQ: 2–6) for the plasma group. Use of platelets was also similar (used in 33% of the cryoprecipitate group, median 1 (IQR: 1–2), and 35% of the plasma group, median 2 (IQR: 1–2). Some imbalances were noted in the following transfusion-related variables. Patients managed in the community hospitals were more likely to receive plasma, with only one patient receiving cryoprecipitate as the first-line product. In the cryoprecipitate group, only 17% received subsequent plasma, while a higher percentage of the patients in the plasma group received both plasma and cryoprecipitate (45%).
More patients in the cryoprecipitate group had spine neurosurgery as the primary surgical service (79%), while spine orthopedics was more common in the plasma group (58%). The median case length was slightly longer in the cryoprecipitate group (548 min) compared with the plasma group (498 min), and more patients had posterior versus anterior instrumentation. Compared with the plasma group, the use of cell salvage in the operating room was higher in the cryoprecipitate group (73% vs. 46%), as was the use of tranexamic acid (87% versus 42%) and viscoelastic testing (98% versus 61%).
3.3. Study Endpoints
Table 2 shows the comparison of clinical outcomes in patients receiving cryoprecipitate versus plasma first. Hospital LOS was similar in the univariable and multivariable analysis between patients in the cryoprecipitate group compared with the plasma group (GMR [95% CI]: 0.84 [0.68, 1.04], p = 0.109). The cryoprecipitate group had a shorter ICU LOS among patients admitted to the ICU (46 vs. 74 h; univariable analysis [95% CI]: 0.73 [0.53, 1.00], p = 0.048), although this failed to meet statistical significance in the multivariable model (GMR [95% CI]: 0.72 [0.50, 1.04], p = 0.078). Likewise, the cryoprecipitate group had lower 1-year mortality in the univariable model (5.0% vs. 14.5%; [95% CI]: 0.31 [0.10, 0.88], p = 0.0031, Figure 1), although this was also not significant in the multivariable model (adjusted OR [95% CI]: 0.49 [0.13, 1.88], p = 0.288). Discharge disposition was different between groups in the adjusted model, with the patients in the cryoprecipitate group more likely to be discharged home independently compared to being sent to another facility or needing assistance (adjusted OR 0.41 [95% CI]: 0.16, 0.97, p = 0.049).
As a surrogate of short-term bleeding, total blood products transfused (PRBCs, platelets, plasma, and cryoprecipitate) from the time of meeting the inclusion criteria through POD2 were evaluated. The median number of total units transfused was slightly higher in the plasma group [5 units; IQR: 3–9] compared to the cryoprecipitate group [4 units; IQR: 2–8], but this difference did not reach statistical significance (mean difference [95% CI]: −1 unit [−2, 1], p = 0.253).
The subgroup analysis of patients receiving only cryoprecipitate (N = 100) versus only plasma (N = 38) had similar results to the primary analysis (Table 3), with a trend favoring the cryoprecipitate group, which was only significant for discharge disposition (adjusted OR 0.16, 95% CI: 0.03, 0.69, p = 0.025).
Infection was the most common cause of death by one year, accounting for a higher proportion in the plasma group (Table 4).
4. Discussion
Our study found that in a cohort of patients undergoing major spine surgery, approximately one-third of patients who received PRBCs intraoperatively were subsequently administered either cryoprecipitate or plasma, with cryoprecipitate being more commonly administered. The two groups were similar in terms of demographics, although cryoprecipitate was less commonly used at the community hospitals than at the university hospital. Although all clinical outcomes favored the cryoprecipitate group, only ICU-LOS and mortality achieved significance in the univariable model, while only discharge disposition achieved significance in the multivariable model.
This is the first study to analyze early cryoprecipitate and plasma use in spine surgery and their perioperative outcomes. Our study findings of variation of cryoprecipitate and plasma use among providers are consistent with research in other surgical settings [11]. In our study, patients who received cryoprecipitate first were more likely to be in the neurosurgical service, whereas patients who received plasma transfusion were more likely to be in the orthopedic service. Although this may reflect differing practice patterns, it may also relate to hospital location, with more neurosurgical spine surgeons at the main academic center versus more orthopedic procedures in the community hospitals. The higher use of cryoprecipitate at the university hospital may reflect the provider’s preference or product availability. Given these local differences, our findings may not have fully accounted for patient clustering within hospitals, despite adjusting for location, and this may have affected the difference seen in postoperative disposition.
We also evaluated a short-term bleeding outcome of total blood products transfused from meeting study inclusion to POD2 as a proxy for perioperative bleeding severity. This metric did not differ significantly between groups, suggesting that early cryoprecipitate use may not decrease total transfusion burden. To address bleeding in the surgical setting, there is little evidence to support distinct clinical or laboratory-based triggers for plasma and cryoprecipitate transfusion [12]. Hypofibrinogenemia has been associated with increased blood loss and transfusion in spine surgery [13], and guidelines suggest transfusing at a plasma fibrinogen level of less than 1.5–2 g/L in bleeding patients [14], although there is no precise threshold point for clinically significant hypofibrinogenemia [14]. Use of VET has favored the use of cryoprecipitate [10], and in our study, more patients in the cryoprecipitate group (97.5%) had VET performed in comparison to the plasma group (60.9%). Although traditional laboratory studies, including INR, are an alternative to VET for assessing the degree of coagulopathy, the time required for results in patients with acute intraoperative blood loss can deter many clinicians from conducting these studies, favoring empiric treatment of suspected clinical coagulopathy. In our study, only a minority of patients (26.5%) had INR checked prior to transfusion of plasma or cryoprecipitate.
Despite the need to manage bleeding and coagulopathy, blood component transfusion is associated with complications such as anaphylaxis, transfusion-related acute lung injury, transfusion-associated circulatory overload, and transfusion-related immunomodulation [14]. Interestingly, in our study, of those who died within one year, infection was the most common cause of death, with the survival curves separating between the two groups early after the surgery (Figure 1). Given the limited sample size, we cannot draw definitive conclusions; however, the higher proportion of infection-related deaths in the plasma group may reflect the relatively increased immunosuppression risk associated with plasma transfusion, among other contributing factors.
This study has several limitations. In addition to being a retrospective, single-health-system study, we were unable to examine how abnormal laboratory studies influenced decisions of which product to transfuse. Cryoprecipitate and plasma differ in both their components and their indications for transfusion, and the decision to choose one product over the other is multifactorial, including product availability, use of conventional laboratory testing and/or VET, and personal preference. It is also worth noting that in terms of the dose of plasma, many of the patients can be considered to be underdosed. The standard dose of plasma is 15–20 mL/kg, yet in this study, 42% of the patients in the plasma group received only a single unit of plasma. An additional limitation of our study is the potential for time-to-transfusion bias. While most hospitals maintain thawed or liquid plasma for immediate availability, cryoprecipitate typically requires on-demand thawing, which can delay administration by 30 to 45 min even under optimal conditions. This delay may have influenced the timing of transfusion decisions and introduced unmeasured confounding related to patient stability or clinical urgency. Therefore, we cannot ensure that indication bias and practice variability were fully accounted for in our analyses and note that these findings may not generalize to other settings. During the study period, there were several brief periods of cryoprecipitate shortage, during which the providers were instructed to use plasma preferentially. Although time-limited, these shortages introduced some real-world variability in blood product assignment independent of provider choice and potentially mitigated the residual confounding. However, given the higher likelihood of receiving cryoprecipitate at the university hospital, it is possible that our adjustments in the multivariable models did not allow us to completely account for bias or residual confounding, despite adjusting for hospital location. Therefore, our results should be interpreted as hypothesis-generating, and future prospective design studies should be performed to test these hypotheses.
In this study, we did not examine the use of fibrinogen factor concentrates or prothrombin complex concentrates. Although these have been studied for bleeding-related coagulopathy in major surgery, they are rarely used in our operative setting due to limited availability and the need for hematology approval. The cost and limited availability, along with limited clinical evidence supporting the effectiveness of clotting factor preparations in surgery, have resulted in a lack of standardization of coagulation factor concentrates relative to the blood product transfusion [9].
5. Conclusions
There is limited research on blood product administration to manage coagulopathy during major spine surgery, a procedure often requiring transfusions due to significant blood loss. In our study, patients receiving cryoprecipitate versus plasma as a first-line product were more likely to be discharged home and had a lower 1-year mortality and shorter ICU-LOS, although the differences in mortality and ICU-LOS did not retain significance after accounting for measured confounders. Given the lower cost of plasma to cryoprecipitate, if clinical outcomes are similar, plasma may be preferable. If early cryoprecipitate truly improves outcomes and this study was underpowered or missed confounders, its higher cost may be justified as a first-line treatment for coagulopathy in spine surgery. Further prospective research is needed to guide transfusion practices for managing coagulopathy in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rocos B. Kato S. Oitment C. Smith J. Jentszch T. Martin A. Rienmuller A. Nielsen C. Shaffrey C.I. Lenke L.G. Blood Management and Conservation During Adult Spine Deformity Surgery Glob. Spine J.202515(Suppl. S 3)95s 107s 10.1177/2192568223118881040632291 PMC 12254652 · doi ↗ · pubmed ↗
- 2Bible J.E. Mirza M. Knaub M.A. Blood-loss Management in Spine Surgery J. Am. Acad. Orthop. Surg.201826354410.5435/JAAOS-D-16-0018429303921 · doi ↗ · pubmed ↗
- 3Nair P.M. Rendo M.J. Reddoch-Cardenas K.M. Burris J.K. Meledeo M.A. Cap A.P. Recent advances in use of fresh frozen plasma, cryoprecipitate, immunoglobulins, and clotting factors for transfusion support in patients with hematologic disease Semin. Hematol.202057738210.1053/j.seminhematol.2020.07.00632892846 PMC 7384412 · doi ↗ · pubmed ↗
- 4Vlaar A.P. Toy P. Fung M. Looney M.R. Juffermans N.P. Bux J. Bolton-Maggs P. Peters A.L. Silliman C.C. Kor D.J. A consensus redefinition of transfusion-related acute lung injury Transfusion 2019592465247610.1111/trf.1531130993745 PMC 6850655 · doi ↗ · pubmed ↗
- 5Bharadwaj M.S. Bora V. Managing Fresh-Frozen Plasma Transfusion Adverse Effects: Allergic Reactions, TACO, and TRALI Stat Pearls Publishing LLC.Petersburg, FL, USA 202537983337 · pubmed ↗
- 6Green L. Bolton-Maggs P. Beattie C. Cardigan R. Kallis Y. Stanworth S.J. Thachil J. Zahra S. British Society of Haematology Guidelines on the spectrum of fresh frozen plasma and cryoprecipitate products: Their handling and use in various patient groups in the absence of major bleeding Br. J. Haematol.2018181546710.1111/bjh.1516729527654 · doi ↗ · pubmed ↗
- 7Hinton J.V. Xing Z. Fletcher C.M. Perry L.A. Karamesinis A. Shi J. Ramson D.M. Penny-Dimri J.C. Liu Z. Williams-Spence J. Association of Perioperative Cryoprecipitate Transfusion and Mortality After Cardiac Surgery Ann. Thorac. Surg.202311640141110.1016/j.athoracsur.2023.02.05436914040 · doi ↗ · pubmed ↗
- 8Hinton J.V. Xing Z. Fletcher C. Perry L.A. Karamesinis A. Shi J. Penny-Dimri J.C. Ramson D. Coulson T.G. Segal R. Association of perioperative transfusion of fresh frozen plasma and outcomes after cardiac surgery Acta Anaesthesiol. Scand.20246875376310.1111/aas.1440638467589 · doi ↗ · pubmed ↗