Circulating Tumor DNA as a Prognostic and Predictive Biomarker in Lung Cancer
Puneet Dhillon, Simo Du, Haiying Cheng

TL;DR
This paper reviews how blood-based tumor DNA testing can help diagnose, treat, and monitor lung cancer, especially non-small cell lung cancer.
Contribution
The paper summarizes the current state and potential of ctDNA as a biomarker in lung cancer precision medicine.
Findings
ctDNA can detect actionable genomic changes in lung cancer patients.
ctDNA helps predict treatment response and cancer evolution.
ctDNA is useful for minimal residual disease detection and risk stratification.
Abstract
Liquid biopsy is a type of blood test which detects circulating tumor DNA (ctDNA). This is a key advance in precision medicine which can help in diagnosing, treating, and monitoring lung cancer. This article reviews the current applications of ctDNA in the context of lung cancer, particularly non-small cell lung cancer (NSCLC). Research to date reveal ctDNA is useful in detecting actionable genomic alterations, helps guide treatment, and may predict how the cancer may respond to treatment and evolve. Minimal residual disease detection is another key area of interest. ctDNA detection and tracking have powerful potential uses, and many studies are currently underway. Background/Objectives: Lung cancer remains a leading cause of cancer-related mortality worldwide. In recent years, the development of liquid biopsy, or ctDNA detection in body fluids, particularly blood, has been shown to be…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
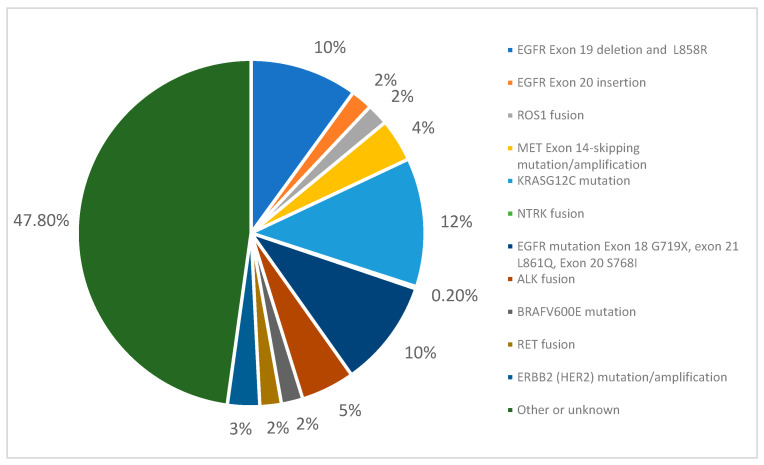 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Genomics and Diagnostics · Lung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment
1. Introduction
Lung cancer is one of the most diagnosed cancers worldwide at 12.4% of total cancer diagnoses [1] and the second most diagnosed cancer in the United States in both men and women. It remains one of the leading causes of cancer-related deaths, causing approximately 131,584 deaths in the United States alone in 2023 [2].
Around 85% of lung cancer is non-small cell lung cancer (NSCLC) [3]. In recent years, the discovery of driver mutations in NSCLC and the utilization of mutation-targeted therapies have significantly improved therapeutic options for patients. Due to this, tumor genotyping is of the utmost importance and is traditionally performed on specimens that are obtained through invasive means, like tissue biopsies. Liquid biopsy is a non-invasive method which analyzes circulating tumor DNA (ctDNA) and can assist in genotyping the tumor [4,5,6].
Cell-free DNA (cfDNA) comprises partially degraded DNA fragments that are not encased in cells. Circulating tumor DNA (ctDNA) in particular comprises short, double-stranded DNA fragments that are released by tumor cells into blood and, depending on the tumor, other biologic fluids like cerebrospinal fluid or urine. ctDNA shed from cancer cells holds unique genetic alterations from where the tumor originated [7,8].
Various international oncology societies currently recommend the use of liquid biopsy for tumor molecular genotyping in lung cancer.
Liquid biopsy is a term used to describe sampling of body fluid, typically blood, to detect tumor cells and cancer cell DNA [6,8]. There are multiple advantages, including being minimally invasive. ctDNA is also thought to better reflect intra-tumoral heterogeneity, given the ability to capture information from different tumor sub-clones. The turnaround time of ctDNA detection is relatively quick, and it can be performed in the office without needing to plan for a biopsy [9,10].
There are various methods to detect ctDNA. Currently, ctDNA testing is typically performed using polymerase chain reaction (PCR)-based or next-generation sequencing (NGS), though NGS is more commercially utilized [11,12,13]. Digital PCR-based methods detect specific DNA sequences and have been preferred in this context over prior PCR methods, but they interrogate only specific numbers of mutations at a time and cannot easily detect copy number alterations and rearrangements [14,15,16]. TAM-seq and CAPP-seq are NGS-based assays. They retain high sensitivity and specificity and can detect multiple mutations of interest, as well as copy number alterations [17,18]. However, for NGS assays, turnaround times can be longer, the cost is higher than for PCR, and they require bioinformatics result interpretation [16,17,18,19].
Fragmentomics analyzes the size patterns of cfDNA and is another area of ongoing research [20,21,22]. Methylation patterns of ctDNA can mirror those in cancerous tissue, and studies have been investigating applications in detection and monitoring [23].
Most commonly, ctDNA testing is performed on blood samples, but it can also be performed in cerebrospinal fluid (CSF) or body fluid; for example, pleural fluid ctDNA analysis of patients with brain metastasis has revealed either the absence or very low levels of ctDNA, possibly because of the blood–brain barrier [24]. However, one study found that ctDNA in CSF had a higher sensitivity than plasma for CNS genomic alterations [25], and another study found that the EGFR mutation detected was the same in the CSF and blood [26,27]. Other body fluids have also been studied, such as urine, saliva, and bronchoalveolar lavage fluid, but they do not have clinically relevant applications yet [28,29,30,31].
In NSCLC, ctDNA has been evidenced to be effective in detection, genotyping, and evaluating therapy response, though further work is required in establishing standardized practices.
2. Applications
2.1. Detection/Screening
In patients who qualify for lung cancer screening, low-dose CT is recommended for early detection, but there are suboptimal compliance rates due to cost and difficulty [20]. Detection of cancers with ctDNA is being studied as a tool to aid in screening to augment low-dose CT chest screening [32,33]. Limitations include early-stage cancers being harder to detect as ctDNA level has been shown to be proportional to tumor burden [31,32,34,35]. There has been work on testing machine learning models to diagnose lung cancer, combining ctDNA, imaging, patient risk factors, and fragmentation features [20,36].
ctDNA levels can fluctuate in response to treatment and thus can aid in monitoring disease progression and/or recurrence. Overall, there is a positive correlation with tumor burden, and higher ctDNA levels in the blood have been linked to poorer prognosis in NSCLC [37,38,39]. There are various clinical trials that aim to study the role of ctDNA in lung cancer screening and stratification such as the Lung Cancer Mutation Consortium (NCT04712877) and DNA Evaluation of Fragments for Early Interception—Lung Cancer Training Study (DELFI-L101 Study) (NCT04825834) [24].
2.2. Genotyping and Detecting Actionable Genomic Alterations (AGAs)
ctDNA can be used to identify specific mutations in lung cancer and guide selection of targeted therapy, which has significantly improved outcomes, especially in recent years [32]. It is current practice to test for EGFR, KRAS, ALK, ROS1, BRAF, NTRK 1/2/3, MET, RET, ERBB2 (HER2), and NRG1 via liquid or tissue biopsy at diagnosis, recurrence, and/or progression. Figure 1 shows the prevalence of different mutations in lung adenocarcinoma, which makes up about 45% of NSCLC. Around 65% of these patients may harbor a clinically actionable genomic alteration [1,2,3,4,5,6,40].
Molecular genotyping from liquid biopsy can be as effective as from a tissue specimen, depending on the specimen characteristics. Specific genomic alterations can also be monitored longitudinally, like in copy number mutations over time, like EGFR after surgery. Liquid biopsy can be performed at any stage of disease including at the time of progression to evaluate for any new potential actional genomic alterations to guide treatment decisions [15,41,42].
There has been some evidence of increased adherence to standard of care and overall more prompt care, though this relationship is likely not causal. For instance, Thompson et al. demonstrated that the inclusion of plasma-based NGS testing led to higher rates of guideline-recommended treatment (74% vs. 46%, p = 0.0005), but it was noted that physicians had test results available before the first patient visit much more frequently when a plasma-based strategy was used, which is likely a contributing factor [43].
2.3. Utilizing ctDNA in Resectable Disease
Approximately 25% to 30% of patients with NSCLC present at stages I to IIIA [11,12,13]. Surgery remains the definitive treatment for early-stage NSCLC. Unfortunately, 30–50% of NSCLC patients will relapse after surgery. Adjuvant treatment has improved overall survival (OS) by around 5%, but a significant proportion of patients develop recurrence, resulting in a median OS rate ranging from 84% at stage IA to 36% at stage IIIA. Minimal residual disease (MRD) refers to the small number of remaining cancer cells, or micrometastasis, during the course or after the completion of treatment. An effective strategy to eradicate MRD and therefore minimize the chance of post-operative recurrence consists of adjuvant therapy. Currently disease is followed using imaging and monitored using the Response Evaluation Criteria in Solid Tumors (RECIST) criteria. CT imaging is most commonly used, and small lesions may be missed given the limit of detection is 2–3 mm. Using ctDNA to track MRD and perform appropriate risk stratification and treatment decisions is an area of research which is becoming more studied.
ctDNA MRD analyses can be tumor-informed or tumor-agnostic [44] and depend on prior knowledge of tissue sequencing. Tumor-informed analysis requires sequencing of tumor tissue to identify mutations to track and is more sensitive. One of the main approaches used has been to employ NGS to track mutations since this facilitates the tracking of multiple mutations in parallel, minimizes the number of tests needed, and increases sensitivity [34], but it requires longer assay development times and may not capture newly evolved mutations [33,45]. Tumor-agnostic methods utilize epigenetic features such as DNA methylation and DNA fragmentation patterns to detect ctDNA. Currently, the sensitivity of these methods is worse compared to tumor-informed approaches and thus, at this time, they are less applicable in MRD tracking [45].
Studies using a variety of tumor-informed NGS-based ctDNA MRD assays have demonstrated that the detection of residual ctDNA after completion of treatment means a higher risk of recurrence [11,12,13,39,45]. There has been variation among them in terms of when ctDNA is drawn after definitive treatment. Lower ctDNA shedding has also been associated with the adenocarcinoma histological subtype as opposed to squamous cell carcinoma [13].
There are two main methodologies for the MRD testing timeline—longitudinal or serial measurements over time and landmark or singular designated time points [19]. Though there is no clear recommendation for one methodology, studies will typically utilize one of the other. In a systematic review of 13 studies that performed ctDNA analysis for post-operative MRD detection in stage I-III NSCLC patients, higher overall sensitivity was achieved in studies that performed longitudinal MRD analysis compared to landmark analysis [18,19].
Chauduri et al. showed that longitudinal tracking of multiple mutations can significantly increase the sensitivity of post-treatment MRD detection (94% vs. 58% for a single mutation p = 0.001) [11,12]. In a prospective study by Zhang et al., landmark analysis was utilized at one month post-operatively and at one month post-adjuvant therapy. For those who received adjuvant chemotherapy, 86.6% of patients with negative MRD status remained disease-free [39]. Different studies utilize different time points in both methodologies, but obtaining measurements at baseline, post-operatively, and before and after systemic therapy seems pertinent, as these landmark timepoints are clinically relevant, though more trials are needed [39].
One of the key applications of interest in MRD testing is guiding treatment decisions on when to de-escalate treatment, such as in decisions around adjuvant therapy.
2.3.1. Chemoimmunotherapy in Resectable Disease
Neoadjuvant chemotherapy and/or immunotherapy is an important treatment strategy in resectable NSCLC [46]. The phase II NADIM study that included patients with resectable stage IIIA disease showed that clearance of ctDNA after three cycles of neoadjuvant nivolumab plus chemotherapy was significantly correlated with longer progression-free survival (PFS) (HR: 0.16, 95% CI: 0.03–0.73) and overall survival (OS) (HR: 0.05, 95% CI: 0–0.62). It is of note that analyses excluded patients with undetectable ctDNA at baseline [47].
The phase III AEGEAN trial used peri-operative durvalumab plus neoadjuvant chemotherapy in patients with resectable stage II-IIIB NSCLC and showed that patients achieving ctDNA clearance after three cycles of neoadjuvant therapy had significantly better event-free survival (EFS) outcomes compared with those with residual ctDNA, especially in the durvalumab-plus-chemotherapy arm (HR: 0.26; 95% CI: 0.13–0.54) [48]. Patients with no detectable ctDNA before surgery had better survival outcomes even in the absence of pathologic complete response [48,49].
It is important to note that the negative prognostic value of ctDNA clearance is suboptimal at this time. Analyses from CheckMate 816 (neoadjuvant nivolumab plus chemotherapy) and CheckMate 77T (peri-operative nivolumab plus chemotherapy trials in resectable NSCLC) both showed that although clearance of ctDNA was correlated with a higher pCR rate, as many as 50% of patients with ctDNA clearance did not achieve pCR, implying that ctDNA negativity may not necessarily translate into eradication of residual tumor cells [50].
2.3.2. Targeted Therapies in Resectable Disease
Targeted therapies have significantly changed the landscape of treatment for EGFR-mutated NSCLC in general, though it is not yet clear how MRD can guide therapy duration and personalize treatment to patients. Herbst et al. in post hoc ADAURA trial analysis looked at patients that would benefit beyond three years using MRD to guide therapy. In this study, MRD preceded DFS events in most patients [51]. DFS and MRD event-free status was maintained for most patients during adjuvant osimertinib treatment and posttreatment follow-up, with most MRD or DFS events occurring after osimertinib treatment discontinuation or completion [52].
The TRACERx study used ctDNA to track a median of 200 mutations in resected NSCLC tissue. It utilized a tumor-informed approach (anchored multiplex PCR) to detect MRD in early-stage NSCLC after surgery. It found that 25% of patients were positive for MRD within 120 days of surgery, and 3- to 6-monthly ctDNA surveillance identified relapse in a further ~20% of landmark-ctDNA-negative patients. A bioinformatic tool, ECLIPSE, was used to track sub-clonal architecture at low ctDNA levels, which identified patients with polyclonal metastatic dissemination and was associated with poor clinical outcomes [51,53].
Jung et al. studied stage I–IIIA EGFR-mutated NSCLC patients who underwent curative resection. ctDNA was measured prior to surgery, after curative surgery, and then at different time points with increasing interval lengths up to 5 years or until clinically definite recurrence [54]. Patients were then classified into three groups: baseline ctDNA-negative, baseline ctDNA-positive but post-operative MRD-negative, and baseline ctDNA-positive and post-operative MRD-positive. The study found that the 3-year DFS rate was significantly different among the three groups (84% versus 78% versus 50%, p = 0.02), suggesting the possible future development of ctDNA MRD status-based risk stratification [54]. Table 1 shows a concise summary of key studies highlighting resectable NSCLC and ctDNA applications and outcomes.
2.4. Locally Advanced, Metastatic, and Recurrent NSCLC
Like in resectable disease, tracking changes using RECIST criteria represents the primary quantification of response and progression [55,59,62,63,64]. In advanced disease, the utility of ctDNA lies in the ability to track it over time to measure progression prior to radiographic progression, and, in theory, change treatment if needed, to improve patient outcomes. Additionally, ctDNA tracking after chemoradiation or consolidation therapy to guide therapy is another area of interest [56,65,66,67,68]. This is not yet a guideline-directed application.
Studies have shown that detecting ctDNA after chemoradiation is associated with worse prognosis, prompting further investigation [69]. Moding et al. studied samples from patients treated with chemoradiation for locally advanced NSCLC, including patients receiving consolidation immunotherapy. Patients ctDNA-negative after chemoradiation had better outcomes, and outcomes of those with MRD after chemoradiation were significantly improved by consolidation immunotherapy [69]. In a prospective observational study, Gale et al. found that patients with ctDNA negativity in all plasma samples and those with ctDNA clearance (previously positive) had longer PFS and OS than patients with persistent ctDNA detection [57]. In certain therapeutic scenarios, the relationship of ctDNA may help guide one towards a specific therapeutic [70,71,72]. For patients being treated for advanced disease with amivantamab plus lazertinib, there have been improved outcomes in high-risk patients with baseline positive ctDNA, as well as without ctDNA clearance, compared to osimertinib [73].
Some studies demonstrate the importance of a molecular response in the relevant biomarker or molecular target irrespective of the target. In metastatic HER2 NSCLC, plasma ctDNA was tested before first-line therapy, and it was found that patients with detectable baseline ctDNA had significantly shorter OS (hazard ratio (HR), 5.25; 95% CI, 1.2–23.9; p = 0.019) [74]. The phase II VISION study evaluated tepotinib in patients with advanced or metastatic NSCLC with a confirmed MET exon 14 skipping mutation and found a high concordance between the molecular cfDNA response and clinical response based on RECIST tumor measurement. Four patients who had decreased levels of cfDNA during treatment did have clinical progression [75]. In patients with KRASG12C-mutated NSCLC treated with sotorasib, those with detectable KRASG12C had inferior progression-free survival (hazard ratio [HR] 2.13 [95% confidence interval [CI]: 1.06–4.30], p ¼ 0.031) and overall survival (HR 2.61 [95% CI: 1.16–5.91], p ¼ 0.017). The disease control rate was significantly higher in those with a molecular response. KRAS amplifications were identified as recurrent treatment-emergent alterations which represent a proposed mechanism of resistance [76].
Table 2 shows a concise summary of key studies highlighting advanced NSCLC and ctDNA and a summary of relevant outcomes. In short, ctDNA detection after an intervention may be a prognostic indicator.
2.5. Resistance
Detecting resistance early to guide treatments and evaluate if there is an impact on outcomes is also a purpose for which ctDNA is being studied [84,87,88,89]. Liquid biopsy is particularly effective in detecting genotypic variations in the background of clonal drift and molecular heterogeneity.
Most patients treated with first- and second-generation TKIs develop resistance early [16,17]; osimertinib is a preferred TKI for this reason [79,81,90,91,92]. However, resistance to osimertinib does occur, and knowing resistance patterns may help predict the course of treatment. The most common mechanism of resistance to osimertinib (which inhibits the T790M isoform) is the development of the C797S isoform, as well as L792X, G796S, L718Q, S768I, G796R, G796D, and G724S [40,93,94]. EGFR gene amplifications and copy number alterations are also mechanisms of resistance [95]. Other mechanisms of resistance include novel fusion events, ERBB2 amplification, and activation of the RAS-MAPK or RAS–PI3K pathway [96,97]. Kato et al. in 2021 performed deep sequencing (CAPP-seq) to analyze ctDNA and were able to identify potentially targetable genetic alterations in patients with osimertinib resistance [43].
Yamaguchi et al. evaluated ctDNA during osimertinib administration as a second-line or further treatment to identify the relationship between EGFR mutation levels and outcomes in patients with advanced NSCLC. In patients with EGFR T790M-positive NSCLC who were receiving osimertinib after prior EGFR-TKI treatment, ctDNA was collected at pretreatment, after 1 month, and at the time of POD. The detection rate of copy numbers of exon 19 deletion, L858R, and T790M in plasma samples was significantly lower 1 month after osimertinib than at pretreatment and significantly higher at PD than at 1 month, whereas that of C797S was significantly higher at PD than at 1 month. No statistically significant difference was observed in the copy numbers of exon 19 deletion, L858R, T790M, and C797S between complete response or partial response and stable disease or PD. Testing based on ctDNA may be helpful in predicting outcomes of osimertinib treatment in T790M-positive NSCLC after previous EGFR-TKI treatment [84].
3. Future Directions
Though there are promising data, further studies are paramount in evaluating the role of using ctDNA to guide care and therapeutic decisions in NSCLC in a way that effects patient outcomes. Both resectable and advanced NSCLC are areas that have seen several promising studies showing prognostic and predictive value, and there are myriad clinical trials that will hopefully help guide clinicians on when and how to change therapeutic course and impacts on survival. Particularly, the ability to risk-stratify patients and escalate or de-escalate based on ctDNA detection would be paramount in limiting toxicities and improving clinical outcomes. Using ctDNA in screening is still immature but could augment low-dose CT and, in the future, could aid in risk stratification. We hope that further studies in these directions lead to consistent incorporation and recommendations for clinicians.
4. Conclusions
The development of liquid biopsy has been a significant development, especially to detect actionable genomic alterations and to choose the appropriate therapy. Though ctDNA has clear indications in guidelines for detecting key biomarkers and has promising applications, it is not uniformly integrated into care and has not reached its full potential yet. The sensitivity and negative predictive value of current ctDNA testing are still low, especially for early-stage cancers. Further research is needed to standardize ctDNA analysis and validate its clinical utility for lung cancer screening, diagnosis, and prognostication.
Additionally, variants can be detected that are not related to the tumor [clonal hematopoiesis of indeterminate potential (CHIP)]. It is also important to note that there are no standard approved practices for MRD testing at this time. There are numerous ongoing clinical trials to evaluate the value of ctDNA in various stages and clinical applications, and ctDNA is effective in the clinical setting so far. Table 3 shows a list, including primary outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Centers for Disease Control and Prevention U.S. Cancer Statistics Lung Cancer Stat Bite U.S. Department of Health and Human Services Washington, DC, USA 2025 Available online: https://www.cdc.gov/lung-cancer/statistics/index.html(accessed on 25 July 2025)
- 3Zhang Y.-L. Yuan J.-Q. Wang K.-F. Fu X.-H. Han X.-R. Threapleton D. Yang Z.-Y. Mao C. Tang J.-L. The prevalence of EGFR mutation in patients with non-small cell lung cancer: A systematic review and meta-analysis Oncotarget 20167789857899310.18632/oncotarget.1258727738317 PMC 5346692 · doi ↗ · pubmed ↗
- 4Merker J.D. Oxnard G.R. Compton C. Diehn M. Hurley P. Lazar A.J. Lindeman N. Lockwood C.M. Rai A.J. Schilsky R.L. Circulating Tumor DNA Analysis in Patients with Cancer: American Society of Clinical Oncology and College of American Pathologists Joint Review J. Clin. Oncol.2018361631164110.1200/JCO.2017.76.867129504847 · doi ↗ · pubmed ↗
- 5Hiatt J.B. Doebley A.-L. Arnold H.U. Adil M. Sandborg H. Persse T.W. Ko M. Wu F. Villalonga A.Q. Santana-Davila R. Molecular phenotyping of small cell lung cancer using targeted cf DNA profiling of transcriptional regulatory regions Sci. Adv.202410 eadk 208210.1126/sciadv.adk 208238598634 PMC 11006233 · doi ↗ · pubmed ↗
- 6Duffy M.J. Circulating tumor DNA (ct DNA) as a biomarker for lung cancer: Early detection, monitoring and therapy prediction Tumor Biol.202346 S 283S 29510.3233/TUB-22004437270828 · doi ↗ · pubmed ↗
- 7Stroun M. Anker P. Maurice P. Lyautey J. Lederrey C. Beljanski M. Neoplastic Characteristics of the DNA Found in the Plasma of Cancer Patients Oncology 19894631832210.1159/0002267402779946 · doi ↗ · pubmed ↗
- 8Wan J.C.M. Massie C. Garcia-Corbacho J. Mouliere F. Brenton J.D. Caldas C. Pacey S. Baird R. Rosenfeld N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA Nat. Rev. Cancer 20171722323810.1038/nrc.2017.728233803 · doi ↗ · pubmed ↗