Maternal Overweight and Obesity Alter Neurodevelopmental Trajectories During the First Year of Life: Findings from the OBESO Cohort
Arturo Alejandro Canul-Euan, Jonatan Alejandro Mendoza-Ortega, Juan Mario Solis-Paredes, Héctor Borboa-Olivares, Sandra Martínez-Medina, Carmen Hernández-Chávez, Gabriela Gil-Martínez, Erika Osorio-Valencia, Mariana Torres-Calapiz, Blanca Vianey Suárez-Rico

TL;DR
Mothers who are overweight or obese before pregnancy may negatively affect their infants' brain development, especially in language and motor skills during the first year of life.
Contribution
This study identifies specific neurodevelopmental impacts of maternal pregestational overweight/obesity in infants during the first year of life.
Findings
Infants of overweight/obese mothers had lower language and socio-emotional scores at 12 months.
Higher maternal BMI was linked to lower motor and language scores at 6 and 12 months.
Overweight/obesity was associated with a decline in language development from 6 to 12 months.
Abstract
Background/Objectives: Overweight and obesity during pregnancy are metabolic risk factors that may compromise offspring brain development. The first 1000 days of life represent a critical window in which neurodevelopmental trajectories are shaped by intrauterine and early-life exposures. The 6- and 12-month milestones are key checkpoints where deviations may emerge, and interventions are most effective. This study evaluated the association between maternal pregestational weight status and infant neurodevelopment at 6 and 12 months of age. Methods: Mother and infant pairs from the OBESO perinatal cohort in Mexico City were included. Women in the first trimester of pregnancy were classified as normal weight and overweight/obesity according to their pregestational body mass index (pBMI), calculated from self-reported pre-pregnancy weight. Infant neurodevelopment was assessed at 6 and 12…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
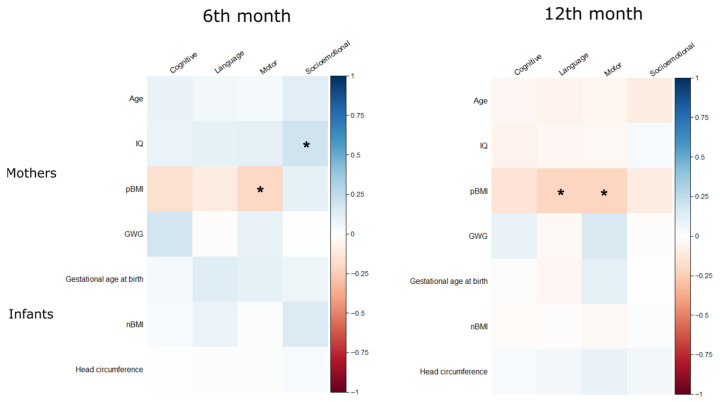 Figure 1
Figure 1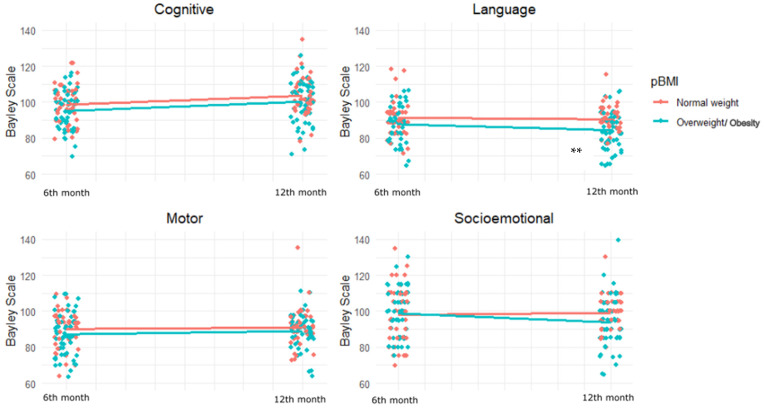 Figure 2
Figure 2- —National Institute of Perinatology
- —CONAHCyT
- —Fund for Research and Innovation in Global Health and Social Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · Infant Development and Preterm Care · Obesity, Physical Activity, Diet
1. Introduction
The global prevalence of overweight and obesity has dramatically risen, particularly among women of reproductive age [1]. In Mexico, 68% of women of childbearing age are affected by overweight or obesity, according to the 2022 National Health and Nutrition Survey [2]. These metabolic conditions during pregnancy can have detrimental effects of fetal development, including neurodevelopmental outcomes [3,4]. Emerging evidence suggests that maternal pregestational body mass index (pBMI) plays a crucial role in shaping early-life brain development, potentially altering trajectories that extend into childhood and adolescence [5,6,7,8,9,10,11].
Pregestational overweight and obesity are associated with a range of adverse outcomes, including altered micronutrient transfer, inflammatory processes, oxidative stress, and lipotoxicity, which may disrupt fetal brain development [12,13]. These conditions may also influence infant outcomes through postnatal factors such as altered breastmilk composition and maternal–infant interaction [14]. Epigenetic modifications and changes in the infant gut microbiome linked to maternal metabolic status further support the concept of developmental programming [3].
Neurodevelopmental disorders affect approximately 10–20% of the global population [15] and share common pathophysiological mechanisms, many of them may originate even before conception [16,17]. In this context, the first 1000 days of life—from conception to two years of life—constitute a biologically sensitive window in which developmental trajectories are established. [18]. During this time, the brain undergoes rapid structural and functional changes and is particularly vulnerable to nutritional and environmental insults [15,19]. Each month contributes to a dynamic path shaped by genetic, epigenetic, and environmental influences. Within this continuum, the 6- and 12-month marks represent critical checkpoints: at 6 months, the introduction of complementary feeding and the emergence of early motor and social milestones provide opportunities for monitoring divergence; at 12 months, language, mobility, and autonomy accelerate, making atypical trajectories more visible [16,20,21]. These moments are not only clinically relevant but also strategic for parental education, policy engagement, and early intervention. In this sense, the first 1000 days are foundational, and the 6- and 12-month nodes are pivotal points where trajectories can be reinforced, redirected, or repaired [21,22]. While numerous studies have examined associations between maternal obesity and offspring neurodevelopment, most rely on cross-sectional assessments and lack data on early developmental trajectories.
Longitudinal assessments provide deeper insight into developmental patterns and the timing of risk. Previous studies, such as those in the PREOBE and PREDO cohorts, have linked maternal obesity with lower cognitive and motor outcomes in early childhood [23,24]. Recently, maternal overweight has been identified as a risk factor that predicts neurodevelopmental transition patterns toward lower scores from the infant to early childhood stage [25]. However, limited evidence exists regarding how maternal pBMI may influence neurodevelopment as early as 6 and 12 months. This study aimed to fill this gap by evaluating the association between maternal weight status and neurodevelopmental trajectories during the first year of life using data from the OBESO perinatal cohort.
2. Materials and Methods
2.1. Study Population
This study is part of the OBESO (Epigenetic and Biochemical Origin of Overweight and Obesity), prospective perinatal cohort conducted at the National Institute of Perinatology (INPer) in Mexico City. The OBESO study investigates how maternal nutrition, lifestyle, and metabolic and inflammatory profiles influence offspring neurodevelopment and body composition. The study protocol was approved by the INPer IRB (Register No. 3300-11402-01-575-17; 14 January 2024, 11 January 2021), and all participants provided written informed consent.
The study enrolled 238 mother-infant pairs as part of the ongoing OBESO perinatal cohort. Pregnant women were recruited during their first prenatal visit (11–14 weeks of gestation) at the Department of Maternal-Fetal Medicine (January 2017–January 2020). The inclusion criteria required mothers to be at least 18 years old at enrollment, carrying a singleton pregnancy, and free from preexisting chronic diseases (type 2 diabetes, hypertension, thyroid dysfunction, autoimmune, cardiac, hepatic, or renal disorders) or medication use affecting metabolism (e.g., insulin, corticosteroids, metformin). Mothers were excluded if they used tobacco or recreational drugs, had a clinical diagnosis of fetal abnormalities, or reported any medications that could affect their physical or mental health. Newborn without complete neurodevelopment assessments at 6 and 12 months were eliminated from this study.
2.2. Maternal and Infant Variables
Maternal pregestational weight was self-reported, and height was measured using the Lohman’s technique [26] with a digital stadiometer (SECA 246; SECA GmbH & Co. KG, Hamburg, Germany). pBMI was calculated and classified using WHO criteria [27]: normal weight (18.5−24.99 kg/m^2^) and overweight/obesity (≥25 kg/m^2^). Maternal intelligence quotient (IQ) was assessed using the Wechsler Abbreviated Scale of Intelligence (WASI) [28]. Additional variables included maternal age, parity, educational attainment, and gestational weight gain (GWG) were categorized as insufficient, adequate, or excessive according to the Institute of Medicine guidelines [29].
Obstetric complications such as gestational diabetes (GDM), gestational hypertension, preeclampsia, and fetal growth restriction were recorded using standard clinical definitions [30,31]. Gestational age at birth was estimated based on the ultrasound in the first trimester of pregnancy and corrected gestational age was used for preterm infants. Mode of delivery, preterm birth (<37 weeks) [32], Apgar scores, and neonatal anthropometric outcomes (birth weight, length, head circumference) [26] were also documented. Newborn BMI (nBMI) was calculated. Trained dietitians performed all neonatal measurements within 48–72 h of delivery using calibrated equipment (Tanita WB-3000; Tanita Corporation, Tokyo, Japan);infantometer (SECA model 207; SECA GmbH & Co. KG, Hamburg, Germany); and measuring tape (SECA model 212; SECA GmbH & Co. KG, Hamburg, Germany).
2.3. Neurodevelopment Assessment
Infant neurodevelopment was evaluated at 6 and 12 months of age using the Bayley Scales of Infant Development, Third Edition (BSID-III). This standardized tool assesses four domains: cognitive, language, motor, and socio-emotional development [33]. Tests were administered by trained child psychologists at the research facility. Each assessment session lasted 30–40 min at 6 months and 40–50 min at 12 months. Socio-emotional development was assessed via a maternal questionnaire.
2.4. Statistical Analysis
Descriptive statistics and bivariate analyses (Student’s t-test, Mann–Whitney U, one-way ANOVA, Kruskal–Wallis, and Pearson correlations) were conducted to explore associations between maternal and infant characteristics and BSID-III scores.
To evaluate developmental trajectories from 6 to 12 months, linear mixed-effects models were applied for each domain. Models included maternal weight status (overweight/obesity) as the main exposure were adjusted for covariates identified in bivariate analyses (maternal IQ, education, parity; infant sex, gestational age, and nBMI. Marginal and conditional R^2^ values were reported to reflect variance explained by fixed and random effects, respectively. Statistical significance was defined as p < 0.05.
All statistical analyses were conducted using R version 4.4.1 in RStudio (version 2024.09.1+394, “Cranberry Hibiscus”).
3. Results
3.1. Maternal and Neonatal Characteristics
Of the 238 mother–infant pairs initially included as part of the OBESO cohort with complete pregnancy follow-up, 127 children did not complete the neurodevelopmental assessments at 6 or 12 months due to the COVID-19 pandemic, and 28 more did not meet other inclusion criteria. Ninety-seven dyads with full neurodevelopmental data at both 6 and 12 months were included in the final analysis.
No significant differences were observed between normal-weight and overweight/obesity groups regarding maternal age, education, or IQ. While not statistically significant, a higher proportion of multiparous women and cesarean deliveries was observed in the overweight/obesity group. Women with overweight/obesity gained significantly less weight during pregnancy (mean ± SD: 6.16 ± 5.32 kg) than those with normal weight (8.36 ± 3.88 kg, p = 0.02), and a greater proportion experienced excessive gestational weight gain (27.8% vs. 12.4%, p = 0.02). Prevalence of gestational diabetes and preeclampsia was higher in the overweight/obesity group, though not statistically significant. Regarding neonatal outcomes, there were no significant differences between groups in birth weight, gestational age, sex, Apgar scores, or nBMI (Table 1).
3.2. Neurodevelopmental Outcomes
In the bivariate analysis, at 6 months of age, neurodevelopmental domain scores did not differ significantly by maternal weight status. However, at 12 months, infants born to mothers with overweight/obesity showed significantly lower language (p = 0.002) and socioemotional (p = 0.031) scores. Male infants scored lower in cognitive development than females at 6 months, while children of multiparous mothers had reduced socio-emotional scores at both time periods (Table 2).
Neurodevelopmental scores at 6 and 12 months, stratified by infant sex and maternal pre-pregnancy BMI, are presented in Table 3. At 6 months of age, no significant differences were observed across pBMI groups in any neurodevelopmental domain for either sex, although a non-significant trend toward lower cognitive, language, and motor scores was noted among infants born to mothers with overweight/obesity. By 12 months, significant differences emerged. Among females, language scores were lower in the overweight/obesity group (p = 0.046). Among males, maternal overweight/obesity was associated with significantly lower scores in cognitive (p = 0.039), language (p = 0.010), and socioemotional (p = 0.029) domains. Motor scores did not differ significantly between groups at either age.
Negative correlations were observed between pBMI and motor scores at 6 months (r = −0.2, p = 0.03), and between pBMI and both motor (r = −0.21, p = 0.04) and language (r = −0.21, p = 0.04) scores at 12 months. Maternal IQ was positively associated with socio-emotional development at 6 months (r = 0.21, p = 0.04) (Figure 1).
3.3. Developmental Trajectories
In mixed-effects models (Figure 2 and Table 4) adjusted for maternal and infant covariates, maternal overweight/obesity was significantly associated with a reduction in language scores from 6 to 12 months (β = −5.44, 95% CI: −8.92 to −1.97, p = 0.003). A non-significant trend toward lower cognitive scores was also observed (β = −3.21348, 95% CI: −6.79072 to 0.363772, p = 0.07). Additional predictors included female sex (β = 4.05, p = 0.027) positively associated with cognitive development, and maternal IQ and nBMI positively associated with socio-emotional scores. Multiparity was negatively associated with socioemotional development (β = −7.06, p = 0.003).
These findings indicate that maternal overweight/obesity influences early neurodevelopment, particularly in the language domain, and that both biological and sociodemographic factors contribute to developmental trajectories during the first year of life.
4. Discussion
This study explored the association between maternal overweight and obesity before pregnancy with infant neurodevelopmental trajectories during the first year of life. Our findings indicate that infants born to mothers with overweight and obesity exhibited significantly lower language scores, with a downward trend in cognitive development. These effects persisted after adjusting for relevant maternal and neonatal covariates. These results contribute to a growing body of evidence linking maternal metabolic health to early-life brain development.
Several cohort studies have demonstrated long-term cognitive impacts of maternal obesity [34,35,36,37]. The U.S. Collaborative Perinatal Project reported that maternal pregestational obesity was associated with lower full-scale and verbal IQ scores in children at school age [6]. In the PREDO study, children born to mothers with obesity showed lower scores across multiple domains, including communication, motor, problem-solving, and personal-social skills at 3.5 years [38]. The Millennium Cohort Study in the UK also found that maternal pre-pregnancy BMI was negatively associated with children’s cognitive performance at 5 and 7 years of age, even after adjusting for sociodemographic variables [39].
Our findings regarding decreased language scores at 6 and 12 months are consistent with those of the PREOBE study, which reported lower composite and expressive language scores in infants of mothers with obesity. Follow-up analyses showed an initial acceleration in cognitive and language development followed by a decline at 18 months, particularly in the language domain [23]. A recent meta-analysis also highlighted maternal obesity as a significant moderator of poor language outcomes in early childhood [40].
In terms of motor development, negative correlations between maternal pBMI and motor scores at 6 and 12 months in our study echo findings from the Columbia Center for Children’s Environmental Health, which reported that pregestational obesity was associated with lower psychomotor development scores in boys at 3 years of age [41]. The PREOBE study also documented a trend toward lower gross motor scores among infants of mothers with obesity [42].
Emerging evidence also links maternal overweight/obesity to early socio-emotional difficulties. In our cohort, we observed lower socio-emotional scores at 12 months among infants of multiparous and overweight mothers. Similar patterns were noted in the Shanghai Maternal-Child Pairs Cohort (MCPC) and in the PREDO study, which reported impaired emotional and social development in toddlers exposed to maternal obesity [43,44]. These early impairments may reflect precursors of more severe behavioral or neuropsychiatric outcomes later in childhood [45,46].
The biological mechanisms underlying these associations remain under investigation. Maternal obesity has been linked to systemic inflammation, oxidative stress, altered placental signaling, and disruptions in fetal neurogenesis and synaptic maturation [13,47]. Neuroimaging studies reveal cortical thinning in language-related brain regions between neonates born to obese mothers, indicating that increased maternal pBMI has a programming influence on the developing neonate brain functional networks [12,48]. Additionally, differences in infant gut microbiota and breastmilk composition may influence neurodevelopmental trajectories after birth [49].
Given the significant preventive promise of the Developmental Origins of Health and Disease (DOHaD) hypothesis, follow-up studies have been conducted in older children, suggesting that risks of neurodevelopmental impairments (cognitive, language, emotional and IQ) persist throughout early and middle childhood [50,51]. We must highlight the richness of early follow-ups of child development, as we see differences in the scores of the developmental domains that have a significant inverse association with pBMI at the end of the first year of life. Since it is not entirely clear how neurodevelopmental trajectories occur from the infant to early childhood stage, and little is known about the risk factors affecting the downward transition patterns of neurodevelopment [52], our study contributes to the understanding of this gap of knowledge.
Our study also highlighted the role of maternal and neonatal characteristics. Multiparity was negatively associated with socioemotional development, consistent with literature suggesting reduced one-on-one interaction and increased caregiving burden, underscoring the crucial role of maternal factors in early development [53,54,55,56]. Conversely, higher maternal IQ and nBMI were linked to better socioemotional scores, supporting the protective effects of maternal cognitive resources and adequate postnatal growth [57,58,59,60]. However, an unexpected negative correlation was found between maternal education and language scores at 12 months. Educational level and IQ are closely related and recognized as key predictors of child development; nonetheless, the influence is multifactorial and strongly shaped by contextual circumstances [61]. One possible explanation is that mothers with higher education may have less time to dedicate to direct stimulation and interaction with their infants. In line with this, some studies report improvements in certain developmental domains with higher maternal education, while others describe negative effects in behavioral aspects, or even no significant associations at all [59,60]. Although IQ and education are critical predictors, multiple environmental and family factors modulate the development of children’s skills and learning, making this process highly multifactorial and dynamic [61].
Female sex was associated with higher cognitive scores, consistent with previous evidence showing early sex differences in neurodevelopment [62,63,64,65]. A well-documented gender gap in favor of girls during early childhood indicates that sex influences neurodevelopment and mental health in diverse ways. Differences in brain structure and function between males and females are evident throughout development, even prenatally, and are thought to contribute to variations in behavior, cognition, and the risk of neurodevelopmental disorders [64,65].
The strengths of this study include its prospective design, the use of standardized and repeated neurodevelopmental assessments using BSID-III, and adjustment for key maternal and infant covariates. However, several limitations should be acknowledged. First, the relatively small sample size (n = 97) may have limited statistical power and increased the risk of type I or II errors. While our findings provide preliminary insights, they should be interpreted with caution and validated in larger cohorts. Second, the study was conducted within a single national context, which may restrict the generalizability of the results. Socioeconomic status, cultural factors, healthcare system characteristics, early nutrition, and early childhood service models could all influence the applicability of these findings in other settings. It is important to note that the women recruited for this study were primarily from middle- and lower-income groups, and this low socioeconomic status may have influenced the outcomes observed. To enhance external validity, future research should include cross-cultural comparisons and recruit larger, more diverse populations.
Another limitation is that pregestational weight was self-reported, which may have introduced misclassification. Moreover, we did not include relevant postnatal exposures —such as parenting style, caregiver mental health, detailed infant feeding practices, or diet and supplement consumption during pregnancy—that are known to influence neurodevelopment. In addition, we relied exclusively on BSID-III scores, whereas previous studies have also documented associations with affective and behavioral outcomes using alternative assessment tools [8,9,17]. Other early-life factors, such as adverse childhood experiences, parenting practices, and caregiver mental health [66,67], must also be considered given their strong influence on developmental trajectories.
Beyond biological mechanisms, maternal obesity may indirectly affect child development through caregiving behaviors. Reduced engagement in physically active interactions—such as outdoor play or movement-based stimulation—could restrict opportunities for motor and cognitive development in infancy. These indirect pathways may contribute to the observed differences in Bayley scores, particularly in motor and language domains. Further research is warranted to investigate caregiving behaviors as potential mediators of the association between maternal obesity and infant neurodevelopment.
Taken together, our findings support the hypothesis of early programming of neurodevelopment through maternal metabolic health. The effects observed in the first year of life, particularly in language and socioemotional domains, warrant close follow-up and early screening that consider other important maternal determinants and environmental factors in child development. Interventions promoting maternal health before and during pregnancy may mitigate risks of early neurodevelopmental delays, with potential long-term benefits for child development and well-being.
5. Conclusions
Infants born to mothers with pregestational overweight or obesity showed a decline in certain neurodevelopmental domain scores from 6 to 12 months of age, particularly in language and cognitive trajectories. These findings enhance our understanding of the impact of maternal weight status on early neurodevelopment and highlight the need for closer monitoring and timely interventions during pregnancy and infancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Obesity and Overweight [Internet]Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight(accessed on 25 October 2023)
- 2Campos-Nonato I. Galván-ValenciaÓ. Hernández-Barrera L. Oviedo-Solís C. Barquera S. Prevalence of obesity and associated risk factors in Mexican adults: Results of the Ensanut 2022 Salud Publica Mex.202365 s 238s 24710.21149/1480938060949 · doi ↗ · pubmed ↗
- 3Bolton J.L. Bilbo S.D. Developmental programming of brain and behavior by perinatal diet: Focus on inflammatory mechanisms Dialogues Clin. Neurosci.20141630732010.31887/DCNS.2014.16.3/jbolton 25364282 PMC 4214174 · doi ↗ · pubmed ↗
- 4Godfrey K.M. Reynolds R.M. Prescott S.L. Nyirenda M. Jaddoe V.W.V. Eriksson J.G. Broekman B.F.P. Influence of maternal obesity on the long-term health of offspring Lancet Diabetes Endocrinol.20175536410.1016/S 2213-8587(16)30107-327743978 PMC 5245733 · doi ↗ · pubmed ↗
- 5Hao X. Lu J. Yan S. Tao F. Huang K. Maternal Pre-Pregnancy Body Mass Index, Gestational Weight Gain and Children’s Cognitive Development: A Birth Cohort Study Nutrients 202214461310.3390/nu 1421461336364875 PMC 9654549 · doi ↗ · pubmed ↗
- 6Huang L. Yu X. Keim S. Li L. Zhang L. Zhang J. Maternal prepregnancy obesity and child neurodevelopment in the Collaborative Perinatal Project Int. J. Epidemiol.20144378379210.1093/ije/dyu 03024569381 · doi ↗ · pubmed ↗
- 7Tong L. Kalish B.T. The impact of maternal obesity on childhood neurodevelopment J. Perinatol.20214192893910.1038/s 41372-020-00871-033249428 · doi ↗ · pubmed ↗
- 8Edlow A.G. Maternal obesity and neurodevelopmental and psychiatric disorders in offspring Prenat. Diagn.2017379511010.1002/pd.493227684946 PMC 5572633 · doi ↗ · pubmed ↗