Supportive Care Needs of Patients with Breast Cancer Who Self-Identify as Black: An Integrative Review
Etienne Oshinowo, Emily Peterson, Michelle Audoin, Jennifer Ryan, June Buckle, Clare Cruickshank, Jennifer Jones, Lisa Malinowski Kamran, Aisha Lofters, Patricia Russell, Leila Springer, Danielle VandeZande, Ashanté Lakey, Laura Burnett, Melanie Powis

TL;DR
This paper explores the specific supportive care needs of Black women with breast cancer in Canada, highlighting gaps and priorities for equitable care.
Contribution
The study identifies and prioritizes high-priority supportive care needs specific to Black-identifying breast cancer patients in the Canadian healthcare context.
Findings
Patient navigation was identified as the top priority need for Black breast cancer patients.
Financial support and access to culturally tailored information were highlighted as high-priority needs.
Emotional support and culturally relevant care were also identified as critical for this population.
Abstract
Black women are more likely to be diagnosed with breast cancer at a younger age and with more aggressive cancers. Once diagnosed, they are less likely to receive appropriate treatments for their cancer and are more likely to experience dose reductions, dose holds, and early treatment termination, which can negatively impact survival. However, little is currently known about the specific supportive care and informational needs of this population, particularly in the Canadian healthcare system context. To address this gap, we performed an integrative review to synthesize the findings of prior needs assessments of patients with breast cancer who were reported to be Black from the published literature and integrated them with the findings of a pan-Canadian needs assessment and prioritization exercise conducted by our team. This work identified patient navigation, financial support, access…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
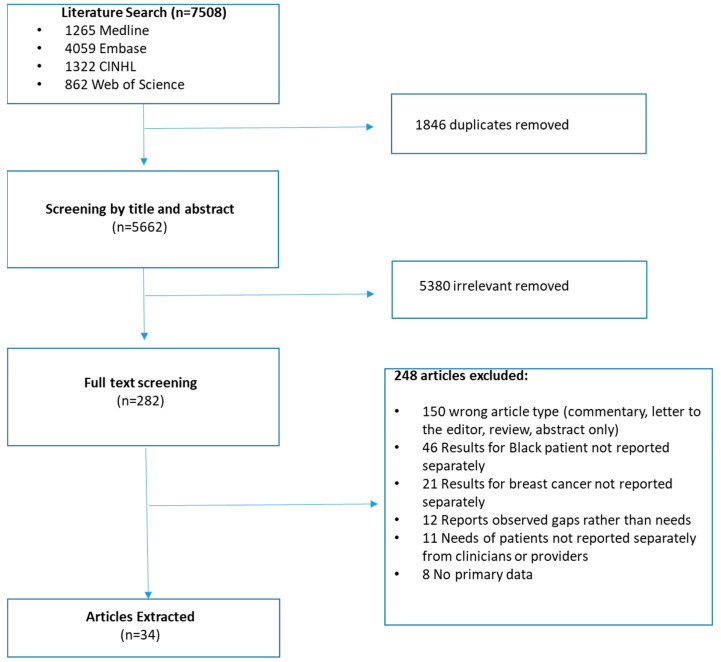 Figure 1
Figure 1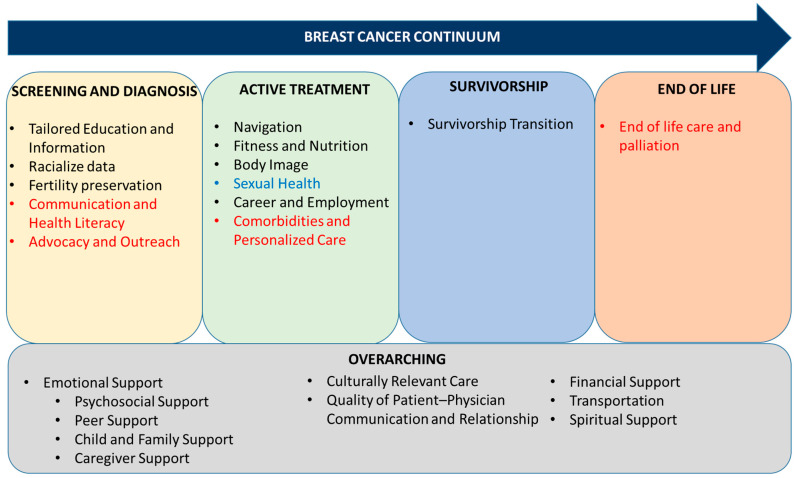 Figure 2
Figure 2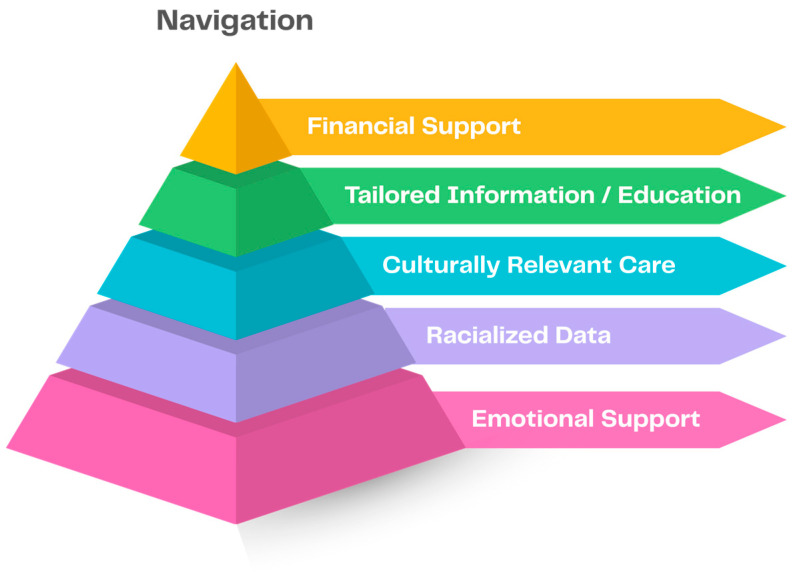 Figure 3
Figure 3- —Canadian Cancer Society
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Cancer Risks and Factors · Economic and Financial Impacts of Cancer
1. Introduction
Breast cancer remains one of the most prevalent malignancies amongst women [1], constituting approximately 25% of incident cancer cases [2] and 14% of cancer-related deaths [3]. Black women are disproportionately affected by aggressive sub-types and are more likely to be diagnosed at a younger age [4] and a higher stage [5]. Once diagnosed, many structural barriers prevent Black-identifying patients from receiving equitable breast cancer care [6]. Fewer Black women receive appropriate genetic testing [7], timely systemic therapy [8], treatment with targeted drugs [9], or access to interventional trials [10]. Additionally, there is growing evidence that Black women experience a higher incidence of serious treatment-related toxicity, such as anthracycline-induced cardiotoxicity [11,12,13], which, with sub-optimal management, can lead to higher rates of dose reductions, dose holds, and early termination, negatively impacting both treatment efficacy and survival [14,15]; however, a lack of representation in prospective trials [16], a lack of race and ethnicity data in routinely collected administrative health data [17], and a lack of targeted research [18] limit current knowledge. In addition to clinical differences and structural barriers to care, social determinants of health, including anti-Black racism, economic insecurity, and medical mistrust, further exacerbate disparities in the health outcomes of Black women and necessitate additional supportive resources [19].
Addressing these multi-layered barriers requires advancements in current clinical research that are inclusive of underrepresented populations [20], as well as systemic interventions that prioritize representation, equity, and culturally tailored models of cancer and supportive care [21]. However, much of the literature to date has focused on describing care disparities rather than addressing underlying causes or centering research on tailored solutions to reduce inequities. As such, little remains known about the unique supportive care and informational needs of this patient population, as there has been no published evidence synthesis to date, particularly in the Canadian single-payer, publicly funded healthcare system context [22].
To address this gap, we undertook an integrative review [23]. We conducted a scoping review to identify and synthesize what is known about the needs of Black patients with breast cancer in the published literature. Findings were then grouped thematically across the stages of the cancer continuum from screening and diagnosis to survivorship care. Since all of the retained studies were completed in the United States, we conducted a virtual nominal consensus group to identify the supportive care and informational needs of patients with breast cancer who self-identify as Black from across Canada and compared these findings to constructs identified in the literature [24]. The final set of needs was validated and prioritized through a series of workshops with a panel of patients with lived experience and community partner organizations to direct future research, advocacy, and policy efforts.
2. Materials and Methods
This study leveraged integrative review research methods [23,25] and included a scoping review of the literature, coupled with nominal consensus groups, and a validation and prioritization exercise through a series of workshops with patient partners with lived experience and relevant community advocacy organizations. The literature review did not require ethics approval; however, the nominal consensus group was approved by the University Health Network Research Ethics Board (UHN REB#: 24-5472), and the validation and prioritization workshops were approved through a separate application to the University of Toronto Research Ethics Board (Protocol#: 48281).
To identify existing studies reporting on the needs of Black-identifying patients with breast cancer, we undertook a scoping literature review. Relevant citations published from database inception to January 2025 were retrieved from MEDLINE, Embase, and CINAHL using search terms grouped by key concept (breast cancer, support needs, and Black), with syntax and headings translated as appropriate across databases (Table S1). Resultant citations were imported into Covidence (Veritas Health Innovation; Melbourne, Australia) for review, and duplicates were removed. The review was carried out in accordance with the PRISMA extension guidelines for scoping reviews [26]. Studies were included if they reported on primary research examining the needs of Black-identifying patients with breast cancer of any gender or sex. The search was restricted to articles published in English and reporting on adult populations. Articles were excluded if they were literature reviews, protocols for needs assessments without accompanying findings, commentaries, letters to the editor, or abstracts only. Additionally, articles reporting on population-level cohort studies that derived patient needs based on observed gaps in care, rather than soliciting needs directly from patients, were excluded.
Titles, abstracts, and full texts were screened for inclusion by two reviewers (EP and MP); no conflicts in inclusions between reviewers were identified. Details of retained articles were abstracted using a standardized abstraction form into Excel (Microsoft, Redmond, DC, USA) by one reviewer (EO). A second abstractor (MP) extracted data from a random sub-set of 10 articles to evaluate the reliability of the abstraction process; there were no discrepancies identified between reviewers. Findings were inductively coded, then thematically grouped into constructs and concepts and mapped to the stages of the breast cancer continuum: (1) screening and diagnosis; (2) active treatment; (3) survivorship; (4) end-of-life; or (5) overarching.
In parallel, we undertook a nominal consensus group [24] to identify the needs of patients with breast cancer who self-identified as Black from across Canada. Potential participants were recruited through an email invitation disseminated to members of the Patient and Caregiver Partners listserv of the Canadian Cancer Society. To be eligible to participate, participants had to be ≥18 years of age, have a prior diagnosis of breast cancer for which they had received treatment in the previous 12 months, self-identify as Black, reside in Canada, and be proficient in spoken English. The nominal group was carried out virtually on Zoom for Healthcare (Zoom Communications, San Jose, CA, USA). The group was facilitated by members of the study team trained in nominal group technique (MA, JR, and MP). At the start of the session, participants were provided with a prompt: “If you received any supportive resources or services during your treatment with chemotherapy what services did you find helpful? If you did not receive any supports, what support resources or services do you think would be/have been helpful to you during and after chemotherapy?” Following silent ideation, participants underwent iterative round-robin-style rounds of ideation until all ideas were recorded, then serially discussed each idea [27,28,29]. Ideas were reorganized and combined or parsed by the participants as they reached consensus on the final set of needs. The session was recorded and transcribed verbatim; supportive quotes for each of the needs identified in the session were extracted from the transcript. The final set of needs identified by the nominal consensus group was then compared against the findings of the literature review to identify areas of concordance and discordance [23,25].
The final set of needs identified by the nominal consensus group was then presented to a panel consisting of patients with lived experience and relevant community partner organizations, assembled to leverage a community-based participatory research approach [30] to co-design a supportive care program for patients with breast cancer who self-identify as Black. Through a series of workshops, panel members validated the list of supportive care and informational needs and undertook consensus discussions to arrive at a final ranking of the needs in order of priority from highest to lowest.
3. Results
3.1. Details of Retained Articles
The scoping literature search identified 7508 articles; after duplicate removal and review, 34 met inclusion criteria and were retained for analysis (Figure 1). All retained studies were conducted in the United States and focused on Black patient populations residing in specific regions, either the American South (42.9%; 15/34) or on the East Coast (29.4%; 10/34; Table 1). Sample sizes were generally small, with 47% (16/34) of articles reporting on samples of ≤25 patients (range: 9–1056). None of the articles identified needs across all stages of the cancer continuum or included all of the identified constructs. Details of all the retained articles are included in Table S2. The majority of articles identified supportive care and interventional needs relevant to all stages of the cancer continuum (overarching; 94.1%; 32/34), screening and diagnosis (76.5%; 26/34), or active treatment (70.6%; 24/34). Few articles included needs from the survivorship phase (23.5%; 8/34), while none of the articles specifically discussed end-of-life care or palliation.
3.2. Supportive Care and Informational Needs Common to the Literature and Nominal Consensus Group (NG)
The literature review identified 15 unique informational and supportive care needs, many of which spanned the breast cancer continuum. Findings of the literature review are summarized in Figure 2 and below.
3.2.1. Overarching Needs
The literature review findings highlighted the need for emotional support (79.4%; 27/34) across the breast cancer continuum, which included access to formal psychosocial supports (38.2%; 13/34) who can be confided in and who will actively listen, to address changing relationships, social needs, and mental health across the cancer journey (Table 2). In line with the literature, NG participants stressed the need for psychosocial supports to be provided by clinicians who are knowledgeable of and reflect the Black community. NG participants also identified the need to provide upfront information for patients on the types of supports that are available, how long the wait for psychosocial support is likely to be, and the frequency and duration of support that will be provided. The literature review identified the need for more targeted emotional support resources specifically for children and families (35.3%; 12/34) and caregivers (2.9%; 1/34). NG participants highlighted the impact that cancer care can have on existing family dynamics and stressed the need for tailored family support groups, as well as the availability of childcare to reduce barriers to accessing cancer treatment and supportive resources. The literature underscored the need for access to peer support (61.8%; 21/34) for practical support and advice from others with lived experience with cancer who had faced similar challenges. NG participants reflected that it was helpful to connect with community support groups and peers who had lived similar experiences to themselves and understood what they were going through. However, they highlighted the need for better engagement with, and integration within, the Black communities and Black-focused community health organizations to ensure patients have a safe and welcoming space.
The findings emphasized a desire for spiritual support (47.1%; 16/34) to help describe a sense of meaning in the cancer experience in line with the patients’ belief system; however, this need was much less pronounced in the NG than in the literature, which may reflect both the representativeness of the NG sample and the greater diversity of religious beliefs amongst patients from Canada. To reduce barriers to accessing care, reliable transportation was needed to get to and from treatments and supports (8.8%; 3/34), and financial resource information and supports (26.5%; 9/34) for out-of-pocket cancer and treatment-related costs. NG participants identified information and resources to support financial planning and critical injury insurance, and financial assistance as needed financial supports. In the literature, patients emphasized the need for culturally relevant and trauma-informed approaches to care (14.7%; 5/34), as well as improved quality of patient–physician communication and relationships (35.3%; 12/34) through shared decision-making and culturally sensitive communication approaches. NG participants stressed that seeing any gains in breast cancer care equity would require healthcare system adoption of anti-racist and anti-oppressive reflexivity and approaches as a precursor.
3.2.2. Screening and Diagnosis
Specific to the screening and diagnosis phases, patients identified the need for culturally and ethnically tailored information and education on breast screening and cancer risk, treatment efficacy, and treatment options (67.6%; 23/34). Participants in the NG noted that most easily identifiable sources of information are from the United States and that access to information can help drive self-advocacy efforts. The NG highlighted similar informational needs as in the literature but also specifically called out the need for information on what to expect during treatment, how to interpret test results, information on types and rates of treatment-related toxicities amongst Black patients, scarring and skin toxicities on darker skin tones, prosthetics, genetic testing, end-of-life care and hospice, and resources for Black hair, including racially tailored information on the effectiveness of cold capping.
Patients in the literature and NG were interested in access to racialized data on treatment-related toxicities, risks, and clinical outcomes to inform treatment decision-making (11.8%; 4/34). Additionally, both the literature review (8.8%; 3/34) and NG highlighted the need for information and resources to support fertility preservation. In the NG, patients highlighted the need for sufficient time to think about and make informed decisions, and the pivotal roles that emotional and financial support play in fertility preservation discussions and choices. Participants in the NG highlighted the cultural significance of family and children and the potential for loss of identity and community alongside loss of fertility post-treatment. The NGs identified two additional constructs that were not included in the literature review: communication and health literacy, and advocacy and outreach, which are likely reflective of sociodemographic and contextual differences between our NG sample and samples from previously published articles from the United States, which were primarily carried out in the South and/or in jurisdictions with lower median incomes and literacy rates, and in which proportions of Black-identifying healthcare providers are higher. Participants highlighted the need for better patient–clinician communication and the role that health literacy plays in patients’ abilities to self-advocate or find relevant and trustworthy information. They highlighted the pivotal role that advocacy and community outreach play in improving rates of screening and diagnosis in the Black community and stressed the need for the cancer system to make more intentional efforts to engage with the Black community.
3.2.3. Active Treatment
Patient navigators were identified by both the literature (38.2%; 13/34) and the NG as needs, particularly during treatment decision-making and active treatment. NG participants conceptualized the role of the navigator as someone to walk through treatments, tests, and results with patients; connect them to tailored resources; help them to navigate the healthcare system, particularly between providers and institutions; use lay terms and answers questions; and act as a bridge between the cancer system and the community. Participants stressed how exhausting self-advocacy can be and identified that navigators could alleviate some of that burden by attending appointments with patients and advocating on their behalf. Fitness and nutrition were identified as needs in both the literature (26.5%; 9/34) and in the NG. NG participants identified the need for information on best practices for fitness before, during, and after treatment, how to build stamina to stay on treatment, access to physiotherapy, and the need for culturally tailored information about what to eat when experiencing treatment-related toxicities.
Body image was identified by the literature (20.6%; 7/34); NG participants discussed the relationship between body image, hair texture, and identity. Participants discussed the cultural significance of hair and beauty and the need for emotional support to work through the grief of loss of body parts and body image. Career and employment needs (literature: 2.9%; 1/34) identified in the NG included resources and advice on patients’ rights when navigating critical illness with employers and on how to manage working while experiencing treatment-related toxicities. Sexual health information and education on intimacy and post-treatment reproductive health were identified as needs in the literature (17.6%; 6/34) but were not identified in the NG, which may be reflective of the NG sample size. On the other hand, NG participants identified the need for whole-person, personalized care that considers their comorbid conditions.
3.2.4. Survivorship
Both the literature (23.5%; 8/34) and NG identified the need for improved supports during the transition from active treatment to survivorship. NG participants discussed the fear of cancer recurrence, the sense of uncertainty about what happens or should happen once treatment ends, the evaporation of formal, hospital-based supports at the end of treatment, and the positive role that warm hand-offs to peer support and community-partner organizations could play in improving care.
3.2.5. End of Life
The literature did not identify any constructs specific to end-of-life care. NG participants discussed the need for information on accessing palliative care, hospice care, and medically assisted dying. Participants discussed the lack of information on what supports are available and the associated costs, as well as the need for culturally competent approaches to discussing end-of-life care.
3.3. Prioritization of Supportive Care and Informational Needs
Findings of the literature review and NG were validated through a series of workshops with a panel consisting of patients with lived experience and relevant community partner organizations (n = 9). Through discussions, the identified needs were ranked and re-ranked in order from highest to lowest priority needs until consensus on priority was reached. The panel identified patient navigation as the foundational need, followed, in order from highest priority, by (1) financial support; (2) culturally tailored education and information; (3) culturally relevant care; (4) access to racialized data; and (5) psychosocial support (Figure 3).
4. Discussion
Numerous, persistent disparities in the receipt of equitable breast cancer care for Black patients [4,5,6,7,8,9,10] highlight the ongoing need for tailored interventions aimed at overcoming the structural and sociodemographic barriers to care. However, there has been little published to date on the unique needs of this patient population, and all of the studies so far have been undertaken in the United States. As such, needs may not translate well to the Canadian healthcare system, given the differences inherent in the universal healthcare system context [43], the differing role of private insurance in cancer and supportive care coverage [44], the comprehensiveness of available social supports, breast cancer clinical outcomes [45], and population diversity [46]. In addition to the 15 needs in common between the literature review and NG, we identified four additional needs in the NG that were not identified in the literature: advocacy and outreach, communication and health literacy, comorbidities and personalized care, and end-of-life care. These needs reflect broader structural and cultural barriers that affect Black patients. Through a prioritization exercise, patient navigation was seen as a foundational need, with financial support, tailored education and information, culturally relevant care, access to racialized data, and emotional support as the highest-ranking needs. To our knowledge, our study is the first to synthesize the literature around supportive care needs of Black-identifying patients with breast cancer, and the first published needs assessment of this population in the Canadian context. The results of our study demonstrate a critical gap between the documented needs of predominantly United States-based literature and the lived experiences of Canadian women. Understanding the priorities of Black-identifying patients with breast cancer is an instrumental step in developing community-centered interventions to address these needs [47], alongside policy changes and funding opportunities that support their implementation and evaluation and help to break down structural barriers to care.
The needs for navigation, culturally tailored information and education, and culturally relevant care were explicitly called out as community priorities through our consensus discussions. Navigation fatigue has been described as a growing issue prevalent in marginalized patients. Repeated interactions with fragmented healthcare support create exhaustion and disengagement [48]. For Black-identifying patients, these prolonged negative interactions with the system are compounded by experiences of racism with care providers and the burden of having to educate providers on their cultural needs [48]. Our findings align with both the Canadian Cancer Society’s Breast Cancer Survey and Focus Group Data [49] and the Uncovered: A Breast Recognition Project [50], which specifically identifies the need for patient navigation to support patients who self-identify as Black, to improve access to and connect them with culturally relevant information and treatments and culturally appropriate supportive care services. There is substantial evidence of the positive impacts of Patient Navigators on improving access to and receipt of quality care for Black patients undergoing breast cancer treatment in other jurisdictions [51,52]. Navigation programs have been shown to shorten the time to treatment initiation, improve adherence, enhance patient satisfaction and quality of life, and decrease unscheduled acute-care utilization, particularly among racialized groups [52,53]. Findings from our NG stressed that proper navigation would require culturally embedded approaches that take into account the structural inequities Black women face. This would require training navigators in anti-racist and trauma-informed practices as well as connecting women to community and other referral networks [54]. A study by Pal et al. [55] demonstrated that scalable, culturally relevant educational interventions, such as web-based tools, can empower Black breast cancer patients with the resources and knowledge required to make informed decisions about their care. Another project, which supports women across the United States and is known as the Susan G. Komen Foundation’s Black Women’s Health Equity, which echoes the need for navigators to be culturally informed. The foundation notes that without addressing financial toxicity, systemic mistrust, lack of support networks, and cultural disconnection, navigation programs will ultimately be ineffective for Black patients [56].
Financial impacts of cancer on patients are substantial, with the Canadian Cancer Society estimating the lifetime out-of-pocket costs for a patient at approximately 33,000 CAD [57]. The need for improved financial supports for patients with breast cancer was reflected in both the literature and NG findings. Financial toxicity disproportionately affects Black patients, and ultimately, financial strain can influence treatment choices, adherence, and outcomes. This disparity is linked to loss of income post-diagnosis and even persists after controlling for clinical and socioeconomic factors [58]. Financial navigation interventions that provide support for insurance, financial counselling, and accommodations for employment can mitigate financial burden and substantially reduce financial toxicity [59].
The need for improved emotional supports for patients with breast cancer was identified in both the literature review and NG, prioritized by the patient and community partner panel, and included access to psychosocial supports and peer support, inclusive of children, families, and caregivers. Black patients’ emotional distress following a breast cancer diagnosis can be further compounded by experiences of medical racism, cultural isolation, and difficulty in accessing psychosocial resources specific to them [60]. Interventions designed specifically for Black women in America have shown significant promise. A recent randomized trial demonstrated that culturally tailored virtual psychoeducational programs improved both physical and emotional quality of life amongst African-American women with breast cancer [61]. Similarly, a recent study highlighted that psycho-oncology interventions, which are culturally grounded, can alleviate distress and improve the ability to cope with the physical and emotional toll of cancer [62]. Psycho-oncological interventions have also been noted to strengthen the trust between patients and providers, which is essential for communities that have been historically marginalized in healthcare [62].
Our findings highlight the desire for greater access to disaggregated data on treatment effectiveness, clinical outcomes, and treatment-related toxicities to facilitate treatment decision-making. While few articles in the literature reported on this need (11.8%; 4/34), despite Canada’s universal, single-payer healthcare system, financial support was identified in the NG and ranked as high priority by our patient and community partner panel. Many of the existing studies examining race-based differences in treatment and outcomes are from the United States using administrative data, as race data are routinely collected in Medicare and Medicaid data holdings [63]; similar variables are not currently systematically collected within Canadian healthcare billing data [64,65,66]. As differences in historical contexts, patterns of breast cancer care, and diversity of the patient population can impact the generalizability of the findings, improved capture of self-reported race and ethnicity variables to facilitate Canadian analyses is warranted. On the policy side, without the availability of data on race or ethnicity, it is difficult to quantify current disparities in access to or receipt of care by patients who are Black, so it is difficult to advocate for improved equity [67]. Current reports by the Public Health Agency of Canada and the Canadian Public Health Association call attention to the matter of Black Canadians experiencing disproportionate burdens of chronic disease, poor access to healthcare, and higher levels of distress due to systemic racism [66,68,69]. In the absence of robust race-disaggregated data, these concerns remain invisible in both policy and practice, reinforcing the urgency of equity-focused research based in Canada. Efforts to address this gap should remain mindful of historic exploitations by research and build in anti-oppressive data sovereignty and governance structures as foundational components.
Our findings must be interpreted within the limitations of our study. A major limitation of our study is generalizability outside of the North American historical and cultural context. Observed differences between the published literature from the United States and our needs assessment of Canadian patients in this study highlight the need for context-specific understanding of patients’ unmet supportive care and informational needs. There have been few articles published to date examining the needs of breast cancer patients who self-identify as Black, and high heterogeneity between the published studies, necessitates the use of a scoping review methodology to narratively synthesize the findings rather than the use of more rigorous meta-analytic methods. Our search excluded articles written in languages other than English due to logistical constraints in screening and abstracting the articles, which may have biased findings through systematic exclusion of articles from outside of North America, Europe, and Australia. Our study samples for both the NG (n = 3) and patient and community partner panel (n = 9) were small. Despite larger populations of Black-identifying patients in many regions of the United States, sample sizes were comparable to previously published works in this space. This reflects the poor engagement of racialized communities in health research [70], resulting from exploitation by researchers and subsequent distrust [71,72]. While our sample included patients of a spectrum of ages from across Canada, participants were largely from Ontario, and the sample did not include participants from either Quebec or Nova Scotia, which have large Black-identifying patient populations. Additionally, our sample was skewed towards those with a middle or higher income, those self-identifying as originally from the Caribbean, and was not inclusive of men, trans, or intersex people who may have unique supportive care and informational needs. While taking an integrative review methodological approach allowed us to compare and validate our findings from the NG and patient and community partner panel against the broader literature [23], further validation of our findings is needed more broadly in the community, inclusive of patients from across the African diaspora and those representative of additional intersecting identities.
5. Conclusions
Understanding the needs of Black-identifying patients with breast cancer is imperative in informing culturally tailored interventions to address these needs, and policy and funding structures that support improvement in the delivery of equitable care. Patient navigation was identified as a foundational need, with financial support, access to culturally tailored information and resources, culturally relevant care, racialized data for treatment decision-making, and emotional support identified as high priority. Future work should focus on improving representation and diversity in prospective studies, and on leveraging community-based participatory approaches [73], which centre research activities around patient and community voices to co-create community-driven and culturally tailored supportive care interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yedjou C.G. Sims J.N. Miele L. Noubissi F. Lowe L. Fonseca D.D. Alo R.A. Payton M. Tchounwou P.B. Health and racial disparity in breast cancer Adv. Exp. Med. Biol.20191152314910.1007/978-3-030-20301-6_331456178 PMC 6941147 · doi ↗ · pubmed ↗
- 2Government of Canada Breast Cancer Available online: https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/breast-cancer.html(accessed on 1 September 2025)
- 3Canadian Cancer Society Breast Cancer Statistics Available online: https://cancer.ca/en/cancer-information/cancer-types/breast/statistics(accessed on 1 September 2025)
- 4Howlader N. Noone A.M. Krapcho M. Miller D. Brest A. Yu M. Ruhl J. Tatalovich Z. Mariotto A. Lewis D.R. SEER Cancer Statistics Review, 1975–2016 Available online: https://seer.cancer.gov/csr/1975_2016(accessed on 1 September 2025)
- 5American Cancer Society Cancer Facts & Figures for African Americans 2013–2014 Available online: https://www.cancer.org/research/cancer-facts-statistics/cancer-facts-figures-for-african-americans.html(accessed on 1 September 2025)
- 6Hirko K.A. Rocque G. Reasor E. Taye A. Daly A. Cutress R.I. Copson E.R. Lee D.-W. Lee K.-H. Im S.-A. The impact of race and ethnicity in breast cancer—Disparities and implications for precision oncology BMC Med.2022207210.1186/s 12916-022-02260-035151316 PMC 8841090 · doi ↗ · pubmed ↗
- 7Reid S. Cadiz S. Pal T. Disparities in Genetic Testing and Care among Black women with Hereditary Breast Cancer Curr. Breast Cancer Rep.20201212513110.1007/s 12609-020-00364-133603954 PMC 7885902 · doi ↗ · pubmed ↗
- 8Stabellini N. Cullen J. Cao L. Shanahan J. Hamerschlak N. Waite K. Barnholtz-Sloan J.S. Montero A.J. Racial disparities in breast cancer treatment patterns and treatment related adverse events Sci. Rep.202313123310.1038/s 41598-023-27578-436683066 PMC 9868122 · doi ↗ · pubmed ↗