Cost-Effectiveness of Sacituzumab Govitecan Versus Chemotherapy in Metastatic Triple—Negative Breast Cancer in Taiwan
Shyh-Yau Wang, Yun-Sheng Tai, Henry W. C. Leung, Shin Hang Leung, Agnes L. F. Chan

TL;DR
This study finds that the cancer drug sacituzumab govitecan is not cost-effective for treating advanced breast cancer in Taiwan at its current price.
Contribution
The study evaluates the cost-effectiveness of sacituzumab govitecan in Taiwan, a new context not previously analyzed.
Findings
Sacituzumab govitecan costs USD 121,836 per QALY gained, exceeding Taiwan’s WTP threshold of USD 102,120.
A 50% price reduction would improve the likelihood of cost-effectiveness.
Drug cost is the main factor affecting cost-effectiveness results.
Abstract
Sacituzumab govitecan (SG) is a novel antibody–drug conjugate (ADC) targeting trophoblast cell surface antigen 2 (TROP2) expressing cancer cells. It delivers the topoisomerase I inhibitor SN-38 to induce DNA damage-mediated apoptosis. Sacituzumab is approved for patients with unresectable, locally advanced or metastatic triple-negative breast cancer who has received two or more prior systemic therapies, at least one of which was for metastatic disease. Based on the positive results from the Phase III ASCENT clinical trial, sacituzumab offers an alternative new mechanism treatment option for patients with metastatic triple-negative breast cancer who have failed initial chemotherapy and have a poor prognosis. However, previous cost-effectiveness analyses conducted in the United States and China concluded that sacituzumab is not cost-effective for mTNBC at its current price, within…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
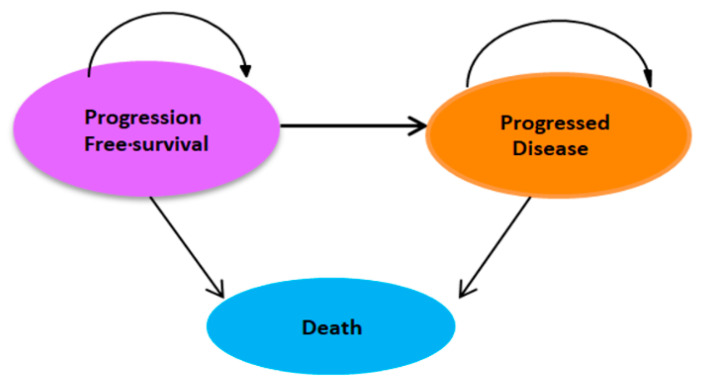 Figure 1
Figure 1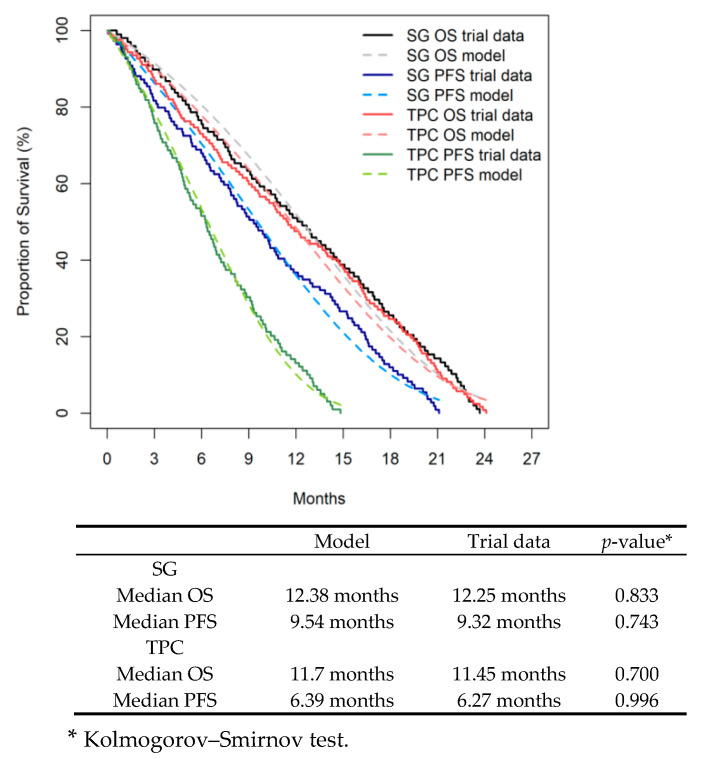 Figure 2
Figure 2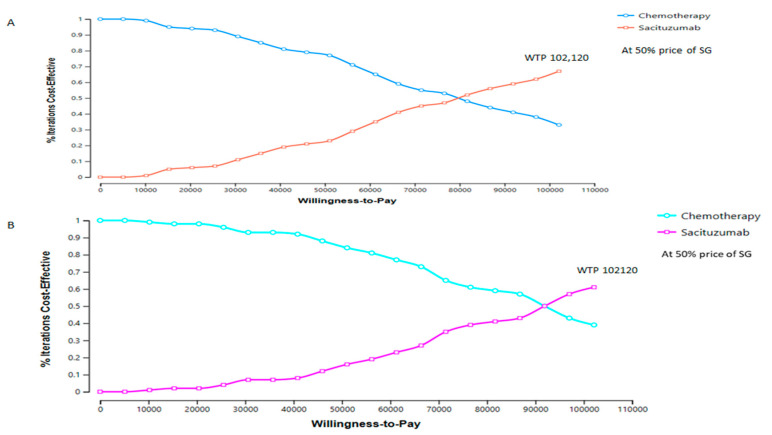 Figure 3
Figure 3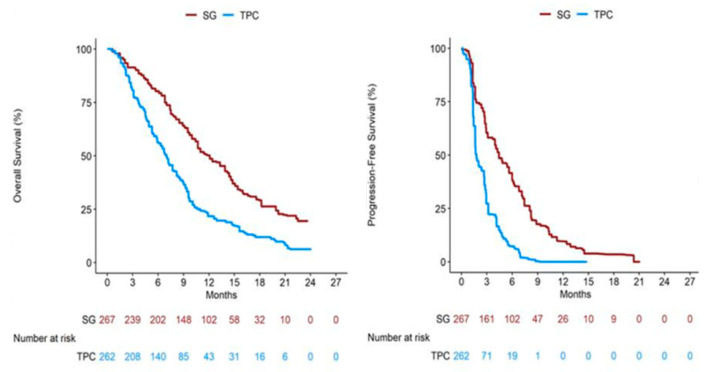 Figure 4
Figure 4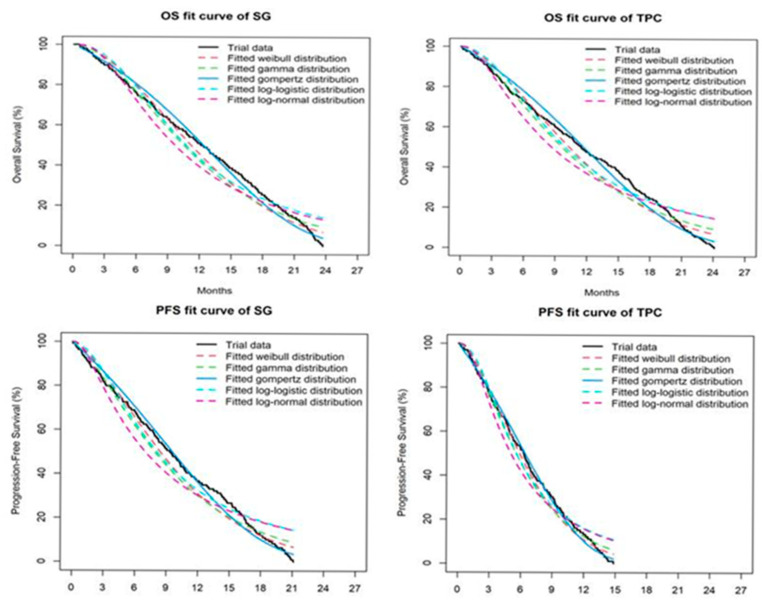 Figure 5
Figure 5- —An Nan Hospital, China Medical University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Breast Cancer Therapies · HER2/EGFR in Cancer Research · Colorectal Cancer Treatments and Studies
1. Introduction
Triple-negative breast cancer (TNBC) is an aggressive subtype of breast cancer characterized by high mortality, early recurrence, and poor prognosis. Globally, it accounts for approximately 15–20% of all breast cancer cases [1]. Recent epidemiological studies have shown that the incidence of TNBC is rising among adolescents and young adults [2]. Women born after 1980 have a higher risk of developing breast cancer—particularly TNBC—compared with those born before 1950 [3]. In Taiwan, the incidence of TNBC increased from 15% in 2012 to 19% in 2022 [4].
Hormone receptor-positive, human epidermal growth factor receptor 2-negative (HR+/HER2−) breast cancer remains the predominant molecular subtype, representing about 70% of all breast cancer cases [5]. For these patients, endocrine therapy combined with cyclin-dependent kinase 4/6 (CDK4/6) inhibitors is the current standard first-line treatment [6]. Although CDK4/6 inhibitors are highly effective in treating HR+/HER2− breast cancer, their high cost often makes them less cost-effective in this setting. Previous cost-effectiveness studies have suggested lowering drug prices, potentially benefiting patients, and exploring their potential use in combination with other therapies or as monotherapy for triple-negative breast cancer (TNBC) to improve cost-effectiveness. However, CDK4/6 inhibitors are currently not considered cost-effective for treating TNBC because they are not approved for this specific subtype and are expensive [7,8]. TNBC management contributes disproportionately to healthcare expenditures: in the United States, it accounts for 5–10% of cancer costs and approximately 0.5% of the total healthcare budget [9]. In Taiwan, TNBC represented about 0.033% of total cancer treatment costs in 2022 [10]. These figures highlight both the clinical and economic burden of TNBC and the urgent need for effective and affordable therapies.
Sacituzumab govitecan (SG) is a novel antibody–drug conjugate (ADC) targeting trophoblast cell surface antigen 2 (TROP2) expressing cancer cells. It delivers SN-38, the topoisomerase I inhibitor, to induce DNA damage-mediated tumor cells apoptosis [11]. On 15 January 2024, Taiwan’s NHIA approved SG for reimbursement under restricted conditions: adult patients with unresectable locally advanced or metastatic TNBC who received at least two prior systemic therapies, including one for advanced disease. SG gained approval based on the phase 3 ASCENT trial, which demonstrated superior outcomes compared with standard chemotherapy, including significant improvements in progression-free survival (PFS), overall survival (OS), and objective response rate [12].
There is no doubt that SG offers a new treatment option for patients with metastatic triple-negative breast cancer (mTNBC). However, the cost of SG treatment is significantly higher, which may limit its popularity in many countries [13]. Currently, only a few economic evaluations of SG for the treatment of mTNBC have been conducted. Healthcare policymakers must assess cost-effectiveness to ensure efficient use of limited healthcare resources. Previous cost-effectiveness analyses conducted in the United States and China concluded that SG was not cost-effective for mTNBC at current prices [14,15,16,17,18]. Since SG has now been reimbursed in Taiwan, it is essential to evaluate whether its clinical benefits justify the economic burden. This study is the first to assess the cost-effectiveness of SG compared with chemotherapy for advanced or metastatic TNBC in Taiwan.
2. Methods
2.1. Model Structure
A partitioned survival model (PSM) with three health states was developed to evaluate the costs and long-term outcomes of SG compared with TPC in patients with metastatic TNBC from the perspective of Taiwan’s NHIA. The three mutually exclusive health states were progression-free survival (PFS), progressed disease (PD), and death (Figure 1).
The proportion of patients in each health state at each cycle was estimated from OS and PFS curves reported in the ASCENT trial [12]. The area under the PFS curve represented the proportion of patients alive without progression, while the area under the OS curve represented total survival. A cycle length of one month was used, and the model adopted a 10-year time horizon to capture lifetime outcomes. Costs and health outcomes were discounted at an annual rate of 3% [19].
Primary outcomes included total costs, QALYs, ICERs, and net monetary benefit (NMB). NMB represents the total monetary value of an intervention by subtracting its costs from its benefits, all expressed in monetary terms, given a specific willingness-to-pay (WTP) threshold. A positive NMB suggests that the intervention is worthwhile compared to the alternatives at that threshold, offering a single, absolute measure of value rather than a ratio like the incremental cost-effectiveness ratio (ICER) [20]. The model was developed using TreeAge Pro version 2022 (TreeAge Software, Williamstown, MA, USA).
2.2. Clinical Data
As individual patient data from the ASCENT trial were unavailable, survival data were reconstructed from Kaplan–Meier curves using WebPlotDigitizer v4.6 and the Guyot algorithm [21]. Reconstructed curves are shown in Appendix A. The reconstructed curves were validated by comparing the model clinical outcomes with selected trial data (median OS and PFS). Based on the local oncologist’s assessment of clinical plausibility and goodness of fit, the goodness of fit of the reconstructed IPD with the standard parametric distributions of Weibull, Gamma, lognormal, and log-logistic was compared using the analytic Akaike distribution and the Bayesian information criterion [22,23]. Extrapolated curves informed long-term outcomes (Appendix B: Figure A2; Appendix C: Table A1).
2.3. Direct Medical Costs and Utility
The analysis adopted the NHIA perspective. Only Direct medical costs were included in this analysis (Appendix D Table A2). In the PFS state, drug costs included SG or TPC acquisition costs, administration costs, assessment costs (MRI costs), and the cost of treatment of grade 3/4 adverse events. In the PD state, costs included costs of MRI, palliative care or basic supportive care, and hospice per event (SAEs).
We investigated that the total drug costs of patients who received either SG at a dose of 10 mg per kilogram of body weight intravenously on days 1 and 8 of each 21-day cycle or single-agent chemotherapy or TPC (eribulin (1.4 mg/m^2^ IV, days 1 and 8 of a 21-day cycle), vinorelbine (25 mg/m^2^ IV, day 1 of a 7-day cycle), capecitabine (1000–1250 mg/m^2^ orally twice daily, days 1–14 of a 21-day cycle), or gemcitabine (800–1200 mg/m^2^ IV, days 1, 8, 15 of a 28-day cycle)) according to the ASCENT trial, To calculate the dosage of the above drugs, we adopted a mean body surface area (BSA) of 1.72 m^2^ and body weight of 57.3 kg, reflecting the Taiwanese female population [24]. Drug costs and other direct medical costs were collected based on the 2024 NHIA reimbursement list [25] and converted to US dollars (USD 1 = TWD 29) in June 2025. Only treatment costs of grade ≥ 3 SAEs were included, as lower-grade events incur minimal additional costs.
Appendix E Table A3 summarizes cost inputs. The willingness-to-pay (WTP) threshold was set at USD 102,120/QALY, which is 3 times the Taiwanese average monthly GDP per capita in 2024, to assess cost-effectiveness [26].
Utility scores for PFS and PD states ranged from 0 (death) to 1 (perfect health) and were derived from a previously published cost-effectiveness study [27,28]. We assumed 0.85 for SG in PFS, 0.58 for TPC in PFS, and 0.52 for PD. A disutility of 0.28 was applied for grade ≥ 3 adverse events, assumed to occur in the first cycle [27].
2.4. Base-Case Analysis
According to the recommendation of Guidelines for Pharmacoeconomic Evaluations in Taiwan [29], the incremental cost-effectiveness ratio (ICER) was calculated as the incremental cost per incremental quality adjusted life year (QALY) gained between the sacituzumab govitecan group and chemotherapy group. When the ICER was below the defined willingness-to-pay (WTP) threshold, the intervention was considered to be cost-effective. Costs and QALYs were discounted at an annual rate of 3% [19].
2.5. Sensitivity Analyses
One-way sensitivity analyses varied parameters by ±30% of baseline values (Appendix E: Table A3), with results presented in tornado diagrams [23,30]. Probabilistic sensitivity analysis (PSA) used 1000 Monte Carlo simulations, with gamma distributions for cost inputs and beta distributions for utilities. Cost-effectiveness acceptability curves compared SG and TPC against Taiwan’s WTP threshold.
2.6. Scenario Analyses
Three scenario analyses were conducted. The first was price reduction: reducing SG costs by 30% and 50%, while other direct medical costs remain unchanged in the progression-free survival state; the second is threshold analysis: raising the WTP threshold to a certain ratio in Taiwan, Netherlands, and England to compare the likelihood that SG treatment is cost-effective because these two countries adopt a universal public health insurance system similar to Taiwan, but with different policy support. The third was the BMN subgroup: The model for the brain metastasis negative (BMN) subgroup in the ASCENT trial was rerun to examine the cost-effectiveness of SG treatment.
3. Results
3.1. Internal Validity
The internal validation results of the reconstructed survival curves showed that the clinical outcomes predicted by the model were consistent with the empirical trial data in terms of median OS and PFS, confirming the internal validity of the parametric regression model (Figure 2).
3.2. Base-Case Analysis
SG provided 9.40 QALYs compared with 4.94 QALYs for TPC, yielding an incremental gain of 4.47 QALYs. The ICER was USD 113,277 per QALY gained. NMB was −111,074 for SG and USD 171,498 for TPC, indicating that SG was not cost-effective under Taiwan’s WTP threshold of USD 102,120/QALY, and a negative NMB represented that SG was not cost-effective compared with chemotherapy (Table 1).
3.3. One-Way Sensitivity Analyses
Tornado analyses showed that ICER estimates were most sensitive to SG cost in progression-free health state (PFS), and utility values for both SG and TPC in PFS and PD state also had substantial influence.
3.4. Probabilistic Sensitivity Analyses
PSA results showed that at the WTP threshold of USD 102,120/QALY, SG had a 29% probability of being cost-effective, compared with 71% for TPC.
3.5. Scenario Analyses
The first scenario results: Reducing SG’s price (cost) by 30% did not achieve cost-effectiveness. If the price of SG is reduced by 50%, SG has a 75% probability of being cost-effective, while TPC has only a 25% probability of being cost-effective (Table 2; Figure 3A). In both scenarios, the overall population ICER is within Taiwan’s WTP threshold (USD 102,120 per QALY gained).
Table 3 summarizes the results of the threshold analysis. In Taiwan, when the cost of sacituzumab was maintained at the baseline level and the willingness-to-pay (WTP) threshold was increased by 10% and 30%, sacituzumab demonstrated a 56% and 71% probability of being cost-effective, respectively, whereas treatment of the physician’s choice (TPC) showed corresponding probabilities of 44% and 29%. In the Netherlands and the United Kingdom, assuming the same sacituzumab cost as in Taiwan and adjusting the Netherlands’ WTP threshold to 10% of its maximum range (EUR 20,000–EUR 80,000 per quality-adjusted life year [QALY] gained), sacituzumab and TPC exhibited probabilities of cost-effectiveness of 87% and 13%, respectively. In contrast, in the United Kingdom, when the WTP threshold was raised to 2.9 times the current upper limit (GBP 20,000–GBP 30,000 per QALY gained), sacituzumab and TPC achieved probabilities of 57% and 43%, respectively. These differences may be attributed to the greater flexibility of WTP thresholds in the Netherlands and the United Kingdom, which vary according to disease severity and the potential to extend survival among terminally ill patients (often by several months) [31]. Similarly, WTP in Taiwan is a dynamic value that fluctuates with individual preferences, contextual factors, economic conditions, and demographic characteristics. Previous research in Taiwan has indicated that WTP for QALYs varies considerably depending on individual perspectives and uncertainties regarding future health states [32].
In the third scenario, i.e., the BMN subgroup, SG provided 2.6 incremental QALYs at an additional cost of USD 303,107. With a 50% price reduction, SG achieved a 70% probability of cost-effectiveness compared with 30% for TPC, which is consistent with the overall results (Figure 3B).
4. Discussion
SG has been reimbursed in Taiwan for nearly one year for patients with unresectable locally advanced or metastatic TNBC. While clinical outcomes are promising, our analysis indicates that SG is not cost-effective at current prices.
The cost of SG was the key driver of ICER outcomes, consistent with findings from U.S. and Chinese analyses [28,29]. Scenario analyses confirmed that only a 50% price reduction allowed SG to reach cost-effectiveness in both overall and BMN populations. These results highlight the significant economic challenges posed by innovative oncology drugs in Taiwan.
Our findings also align with recent analyses using data from other trials (TROPiCS-02, EVER-132-002), which similarly concluded that SG was not cost-effective across diverse populations [33,34,35,36]. Together, this suggests that SG’s market price may not reflect its clinical value.
In addition to the market price of sacituzumab, a major challenge in economic evaluation lies in defining an appropriate willingness-to-pay (WTP) threshold for each country. To date, there is no international consensus on how such thresholds should be determined. The World Health Organization (WHO) has recommended using one to three times the gross domestic product (GDP) per capita as a cost-effectiveness benchmark, particularly for low- and middle-income countries. However, few nations currently apply this guideline in practice. To illustrate cross-country variation, this study examined the United Kingdom and the Netherlands to explore the price levels at which sacituzumab would become cost-effective within their respective WTP thresholds. Both countries operate universal public health insurance systems similar to Taiwan’s, but their policy frameworks differ substantially. The Netherlands employs flexible thresholds ranging from EUR 20,000 to EUR 80,000 per quality-adjusted life year (QALY) gained, depending on disease severity. In contrast, the United Kingdom applies a narrower threshold of GBP 20,000–GBP 30,000 per QALY gained, typically for interventions that extend survival among terminally ill patients by approximately three months [31].
Our analysis suggests that, at Taiwan’s current sacituzumab price (USD 55,274 per course), cost-effectiveness could be achieved if the WTP thresholds were increased to 10% of the maximum range in the Netherlands and 30% in Taiwan. Conversely, the WTP threshold in the United Kingdom would need to be raised to 2.9 times its current upper limit for sacituzumab to be considered cost-effective. These results highlight the pivotal role of threshold selection in shaping economic conclusions—higher WTP thresholds substantially increase the probability of sacituzumab being cost-effective.
Comparable patterns can be observed across other high-income Asian economies with healthcare systems similar to Taiwan, including Japan, Singapore, and South Korea, as well as China, which is classified as an upper-middle-income economy [37]. All these countries implement universal public health insurance and assess cost-effectiveness using the incremental cost-effectiveness ratio (ICER) relative to a defined WTP threshold. When ICERs exceed the threshold, new technologies are typically considered less cost-effective, and price negotiations or adjustments are often pursued. For instance, South Korea’s WTP threshold is approximately KRW 30 million (around USD 22,000) per QALY for general cases and can increase to KRW 50 million for oncology drugs [38]. In Japan, several studies cite JPY 5 million (approximately USD 37,000) per QALY as a benchmark, with reported ranges extending up to JPY 15 million per QALY [39]. Singapore generally applies a WTP threshold equal to half its GDP per capita—around SGD 48,899 per QALY in 2021 [40]. Similarly, China adopts an ICER-based framework, with thresholds typically set at three times the GDP per capita, closely resembling Taiwan’s approach. Recent studies have reported China’s WTP ranging from USD 38,256 per QALY in 2022 to USD 38,201 per QALY in 2024 [14,28].
Reaching a consensus on the definition and application of WTP thresholds remains a longstanding yet critical issue in health economics. Standardized, transparent, and empirically grounded thresholds are essential to ensure that WTP estimates reflect collective social preferences and provide a robust foundation for policy decisions. Without such clarity, WTP estimates may be inconsistent or misleading, leading to inequitable or inefficient resource allocation. This underscores the importance of context-sensitive, evidence-based approaches to value measurement [41]. Despite decades of debate, achieving fairness and transparency in how healthcare resources are distributed among patients and across countries continues to be a key area for further research [42].
Another noteworthy finding of this study is the influence of health utility values as a sensitivity parameter. Because the ASCENT trial did not report utility data, prior cost-effectiveness analyses have relied on external estimates, which inevitably introduce uncertainty. Future research should therefore prioritize the inclusion of health utility assessments in phase III clinical trials or real-world quality-of-life studies to provide robust, locally relevant data and enhance the precision of cost-effectiveness analyses.
This study has several limitations. First, survival data were reconstructed from Kaplan–Meier curves using parametric extrapolation, which may introduce bias. Second, utility estimates were drawn from published studies rather than direct trial data. Third, assumptions regarding subsequent treatment strategies and best supportive care costs may also affect results. Nonetheless, the analysis provides important evidence for decision-making in Taiwan. Finally, this study may underscore the tension between clinical effectiveness and economic value in oncology. SG improves survival outcomes, but its high cost prevents it from being cost-effective under Taiwan’s WTP threshold.
5. Conclusions
At Taiwan’s current WTP threshold, SG is not a cost-effective treatment for advanced or metastatic TNBC. Substantial price reductions would be required for SG to achieve cost-effectiveness. Alternative reimbursement strategies, such as value-based pricing or pay-for-performance agreements [43,44], or adjusting the WTP threshold value depending on disease severity or patients’ age, may help balance innovation, affordability, and equitable patient access in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Almansour N.M. Triple-Negative Breast Cancer: A Brief Review About Epidemiology, Risk Factors, Signaling Pathways, Treatment and Role of Artificial Intelligence Front. Mol. Biosci.2022983641710.3389/fmolb.2022.83641735145999 PMC 8824427 · doi ↗ · pubmed ↗
- 2American Cancer Society. Cancer Facts & Figures 2025. Atlanta: American Cancer Society. 2025 Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2025-cancer-facts-figures.html(accessed on 5 September 2025)
- 3Sung H. Jiang C. Bandi P. Minihan A. Fidler-Benaoudia M. Islami F. Siegel R.L. Jemal A. Differences in cancer rates among adults born between 1920 and 1990 in the USA: An analysis of population-based cancer registry data Lancet Public Health 20249 e 583e 59310.1016/S 2468-2667(24)00156-739095135 · doi ↗ · pubmed ↗
- 4Hsu J.-Y. Chang C.-J. Cheng J.-S. Survival, treatment regimens and medical costs of women newly diagnosed with metastatic triple-negative breast cancer Sci. Rep.20221272910.1038/s 41598-021-04316-235031634 PMC 8760241 · doi ↗ · pubmed ↗
- 5Gao H.-F. Lin Y.-Y. Zhu T. Ji F. Zhang L.-L. Yang C.-Q. Yang M. Li J.-Q. Cheng M.-Y. Wang K. Adjuvant CDK 4/6 inhibitors combined with endocrine therapy in HR-positive, HER 2-negative early breast cancer: A meta-analysis of randomized clinical trials Breast 20215916517510.1016/j.breast.2021.07.00234271289 PMC 8287214 · doi ↗ · pubmed ↗
- 6Shao H. Zhao M. Guan A.-J. Shao T. Zhou D. Yu G. Tang W. A network meta-analysis of efficacy and safety for first-line and second/further-line therapies in postmenopausal women with hormone receptor-positive, HER 2-negative, advanced breast cancer BMC Med.2024221310.1186/s 12916-023-03238-238212842 PMC 10785354 · doi ↗ · pubmed ↗
- 7Elazzazy S. Al-Ziftawi N.H. Mohamed Ibrahim M.I. Bujassoum S. Hamad A. Comparative cost-effectiveness analysis of CDK 4/6 inhibitors in the first-line treatment of HR-positive and HER 2-negative advanced breast cancer: A Markov’s model-based evaluation Front. Oncol.202414141367610.3389/fonc.2024.141367639114308 PMC 11303311 · doi ↗ · pubmed ↗
- 8Masurkar P.P. Damgacioglu H. Deshmukh A.A. Trivedi M.V. Cost Effectiveness of CDK 4/6 Inhibitors in the First-Line Treatment of HR+/HER 2- Metastatic Breast Cancer in Postmenopausal Women in the USA Pharmaco Economics 20234170971810.1007/s 40273-023-01245-y 36920662 · doi ↗ · pubmed ↗