Phenotypes of Food Allergies in Patients with Atopic Dermatitis Aged Under 24 Months: A Multicenter Study
Mujde Tuba Cogurlu, Metin Aydogan, Ozlem Cavkaytar, Pinar Uysal, Hazal Cansu Culpan, Nalan Yakici, Zeynep Hizli Demirkale, Erdem Topal, Hasan Yuksel, Sezin Aydemir, Nursen Cigerci Gunaydin, Cigdem Aydogmus, Sukru Cekic, Emre Akkelle, Tuba Tuncel, Isil Eser Simsek, Mustafa Arga

TL;DR
This study examines food allergy types in young children with eczema and finds that severe eczema and blood in stool are strong indicators of food allergies.
Contribution
The study identifies three distinct food allergy phenotypes in children with atopic dermatitis and their clinical predictors.
Findings
IgE-mediated food allergy was found in 28.1% of children with atopic dermatitis.
Non-IgE-mediated food allergy was observed in 22.4% of participants.
Severe atopic dermatitis and blood in stool were the strongest predictors of food allergy.
Abstract
Background: Atopic dermatitis (AD) and food allergy (FA) are common allergic diseases in early childhood. AD may be concomitant with FA, particularly in young children. Although studies report the prevalence of FA in children with AD, there is insufficient data regarding different phenotypes of FA. Objective: The aim of our research was to determine the prevalence and clinical predictors of different phenotypes of concomitant FA in children with AD. Methods: This cross-sectional multicenter study included patients younger than 24 months old diagnosed with AD, recruited from 14 pediatric allergy centers. Patients were categorized into two groups using skin testing, allergen-specific IgE, and ultimately food challenge testing (FCT): those with FA and those without. Individuals with FA were classified into three distinct phenotypes: IgE-mediated, non-IgE-mediated, and concurrent IgE- and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
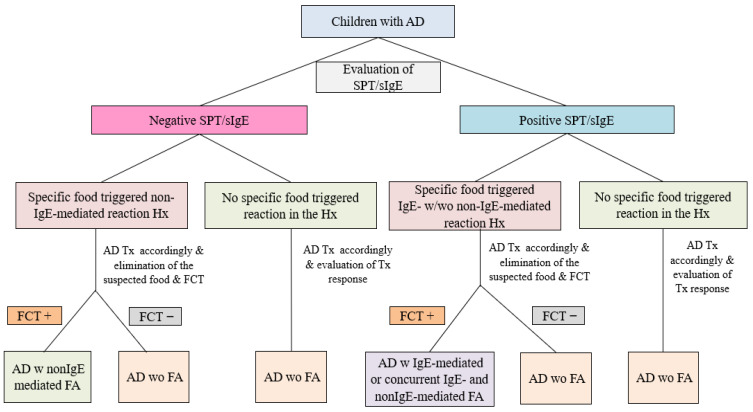 Figure 1
Figure 1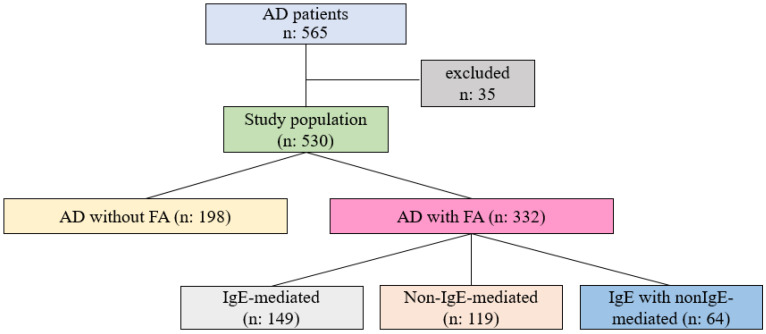 Figure 2
Figure 2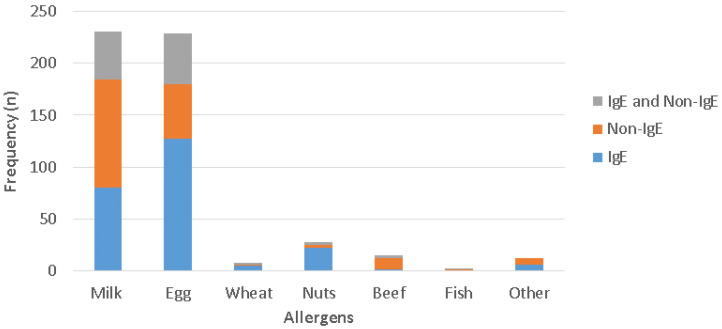 Figure 3
Figure 3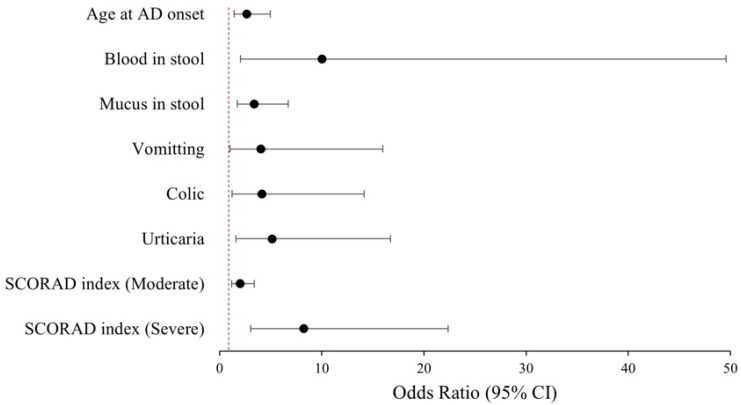 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Allergy and Anaphylaxis Research · Dermatology and Skin Diseases · Allergic Rhinitis and Sensitization
1. Introduction
Atopic dermatitis (AD) and food allergy (FA) are common allergic diseases in early childhood, and the prevalences of both have increased in the last decade [1]. There is an increased risk of FA in children with AD, particularly in those less than 24 months [2,3]. FA can develop through various mechanisms in this population, such as IgE- or non-IgE-mediated ones, and manifest different clinical symptoms from each other [4]. The timely and precise identification of FA phenotypes is essential for managing disease progression. Conversely, the exclusion of FA is crucial to prevent unnecessary elimination diets and adverse clinical outcomes [5]. Data regarding the prevalence of concomitant IgE-mediated FA in AD patients are available due to the objective nature of symptoms and the utility of molecular allergology in the diagnostic process [6]. There remains an insufficient amount of knowledge regarding various phenotypes, especially non-IgE-mediated and concurrent IgE- and non-IgE-mediated FA [7].
The main objective of our study was to determine the prevalence of different phenotypes of concomitant FA in AD patients under 24 months. We also aimed to identify clinical predictors of FA.
2. Methods
This cross-sectional multicenter study included patients younger than 24 months old diagnosed with AD, recruited from 14 pediatric allergy centers in tertiary hospitals in Turkey between March 2019 and February 2020. Ethical approval was obtained from Kocaeli University Medical Faculty Clinical Trials Ethics Committee (project no: 2019/11, decision no: KU GOKAEK 2019/01.17, date of approval: 1 September 2019). The study was conducted in compliance with the Declaration of Helsinki of 1975 (revised in 2013), and parents provided written informed consent before recruitment to the study.
2.1. Data Acquisition and Patient Follow-Up
Individuals under 24 months of age diagnosed with AD by clinicians based on the Hanifin-Rajka criteria were included in the study [8]. Exclusion criteria included the presence of a physician-diagnosed primary immune deficiency or a significant systemic disease affecting other organ systems. The initial data comprised baseline demographic characteristics and a comprehensive clinical history of AD. Furthermore, parents were inquired about the presence of particular dietary proteins that might be responsible for the symptoms related to FA in the mother’s diet (for breast-fed children) or in the patient’s diet [9].
The severity of AD was assessed using the Scoring Atopic Dermatitis (SCORAD) index and was classified as mild (0–25 points), moderate (>25–50 points), or severe (>50 points) [10]. Skin prick tests (SPT)/serum specific immunoglobulin E (sIgE) were conducted on all patients for cow’s milk (CM), egg-white, peanut, tree nuts (hazelnut and walnut), wheat, beef, sesame, lentil, soy, and fish [11]. All patients underwent consistent treatment for AD with moisturizers and topical corticosteroids, followed by a re-evaluation of treatment responses after a two-week period [12]. Open oral food challenge tests (FCT) were performed a minimum of 15 days following the resolution of AD lesions and other FA-related symptoms [13]. FCTs were conducted on all patients with a history of specific food-triggered IgE-mediated reactions under physician supervision in a hospital environment. Patients with histories of non-IgE-mediated food-induced symptoms, lacking food sensitization, were instructed to consume the index food at home following the elimination period. They were then re-evaluated for the occurrence of non-IgE-mediated gastrointestinal symptoms during the 2–4 weeks following OFC [14]. The food identified as responsible, in accordance with OFC, was removed from the patients’ diet (Figure 1).
2.2. Classification of FA Phenotypes
AD concomitant IgE-mediated FA
Patients demonstrating a positive SPT/sIgE, in conjunction with a positive FCT indicated by the emergence of at least one IgE-mediated symptom (urticaria, angioedema, vomiting within 2 h, respiratory symptoms, or anaphylaxis) or an exacerbation of AD indicated by a minimum 10-point increase in the SCORAD index, were categorized as “AD concomitant IgE-mediated FA.”
AD concomitant non-IgE-mediated FA
Patients exhibiting symptoms of non-IgE-mediated FA (food protein-induced allergic proctocolitis), such as blood in stool, recurrent vomiting, loose stools, mucus in stool, painful flatulence, and colic, while being SPT/sIgE negative, were subjected to a diet including the suspected food for a duration of two weeks. Patients experiencing the same reactions following FCT with the suspected food after a two- to four-week elimination period were categorized as “AD concomitant non-IgE-mediated FA.”
AD concomitant IgE- and non-IgE-mediated FA
Individuals who responded with both an IgE- and a non-IgE-mediated FA to a particular food protein or to various food proteins are classified as “AD concomitant IgE and non-IgE-mediated FA.”
AD without FA
Patients who exhibit negative SPT/sIgE, or those with positive SPT/sIgE without experiencing any symptoms or exacerbation of AD during OFC after elimination for 7 days, or who do not indicate non-IgE-mediated symptoms and respond positively to standard AD treatment during follow-up for 4 weeks, are classified as “AD without FA.”
3. Statistical Analysis
SPSS v21.0 (SPSS Inc., Chicago, IL, USA) and Microsoft Office Excel (Microsoft Corporation, Redmond, WA, USA) software were used for statistical analysis. Continuous variables were presented as median and interquartile range (IQR), and categorical variables as frequency and percentage. The Chi-square test or Fisher Exact test, as appropriate, was used to analyze categorical variables. Comparison of continuous variables between two groups was performed using the Mann–Whitney U test and with the Kruskal–Wallis test for more than two groups. Post hoc tests were used for pairwise comparisons. A p-value < 0.05 was regarded as statistically significant. Multivariate logistic regression analysis was performed to explain the co-existence of FA with AD. Results were presented as Odds Ratio (OR) and 95% Confidence Interval (95% CI). The Receiver Operating Characteristic (ROC) curve method was used, and area under the curve (AUC) values were given.
4. Results
4.1. Demographic and Clinical Characteristics of AD Patients, with or Without FA
Of the 565 participants, 35 were excluded from the study based on factors such as insufficient follow-up (n = 11) and failure to undergo (declined consent) FCT (n = 24) (Figure 2). The study was completed with 530 individuals diagnosed with AD with a median age of 7 months (IQR: 5–11), of whom 59.4% (n = 315) were male. The subjects classified as “AD concomitant FA” (62.6%, n = 332) had a median age upon diagnosis of 7 months (IQR: 5–10.8), with 59% being male. In a comparison of patients’ median ages (2 months, IQR: 1–3.5) at the onset of AD symptoms, individuals with AD concomitant FA were significantly younger than those without FA (3 months, IQR: 2–6) (p < 0.001). Patients with FA exhibited more severe AD, with a SCORAD median of 21.9 (IQR: 15.5–31.1), compared to individuals without FA, who also had a SCORAD median of 31.3 (IQR: 20.6–45) (p < 0.001) (Table 1).
4.2. Clinical Characteristics of FA Phenotypes
Three hundred eighty-six patients underwent 529 FCTs, and FA was confirmed in 332 (62.6%) patients. The analysis determined that 4 months is the most discriminative age for distinctive variables related to various types of FA in the study population. AD concomitant IgE-mediated FA was identified in 28.1% (n = 149/530) of participants. FCT results indicated that isolated urticaria occurred in 59 patients, vomiting in 6 patients, respiratory symptoms in 4 patients, and anaphylaxis in 5 patients. Of the participants, 22.4% (n = 119/530) were identified as exhibiting non-IgE-mediated FA. During the late period, blood in stool was noted in 50 patients, intermittent vomiting in 30 patients, and loose stool in 24 patients. Concurrent IgE- and non-IgE-mediated FA was observed in 12.1% (n = 64/530) of the patients with AD (Table 2).
4.3. The Distribution of Triggering Foods for Different Phenotypes of FA
Despite a negative FCT, positive sIgE/SPT results were observed in 27.2% (n = 54/198) of AD patients without FA. Approximately 34.6% (n = 80/231) of patients with CM allergy (CMA) exhibited IgE-mediated responses, while 45.0% (n = 104/231) had only non-IgE-mediated reactions, and 20.3% (n = 47/231) presented with concurrent IgE- and non-IgE-mediated FA. Among patients with egg-white allergy, 55.5% (n = 127/229) exhibited IgE-mediated, 23.1% (n = 53/229) demonstrated non-IgE-mediated, and 21.4% (n = 49/229) presented with both IgE- and non-IgE-mediated reactions. The majority of patients with peanut and tree nut allergy (78.6%, n = 22/28) had IgE-mediated FA (Figure 3).
4.4. Clinic Predictors of FA Phenotypes
The analysis revealed that the probability of concomitant FA with AD was significantly increased by factors including moderate-to-severe AD, the presence of blood in stool, mucus in stool, symptoms of urticaria, vomiting, colic, and the emergence of AD at or before 4 months of age. Multivariate logistic regression analysis indicated that the most significant predictors of the coexistence of FA in AD patients were the presence of blood in stool and severe AD with OR of 10.04 (95% CI: 2.03–49.59) and 8.25 (95% CI 3.04–22.39), respectively (Table 3, Figure 4).
5. Discussion
Our research conducted on a population under 24 months of age found that the prevalence of FA is 62.7% among children with AD. Multiple studies demonstrate that children diagnosed with moderate-to-severe AD at a younger age are more likely to have concomitant FA [15,16,17].
Our study revealed that 87.9% of patients identified with FA exhibited the onset of AD before 4 months of age. Mild AD was observed in 58% of patients without FA, whereas 65.7% of patients with FA exhibited moderate-to-severe AD. This figure may primarily result from the study’s setting in tertiary allergy centers and the observation that over half of the children with FA exhibited moderate-to-severe AD. The majority of patients with mild AD can be treated in primary care and are not referred to tertiary allergy centers.
The primary objective of this research is to highlight the different FA phenotypes in children with AD. The prevalence of IgE-mediated FA varies across studies, ranging from 17.8% to 40% when diagnoses were confirmed by FCTs. This rate increases from 33% to 81% in patients with moderate-to-severe AD [18,19,20]. The present study found that the frequency of solely IgE-mediated FA was 28.1%. Recognition of IgE-mediated FA is more straightforward due to the presence of objective symptoms and the availability of standardized diagnostic tests (SPT, sIgE, OFC, etc.) [21]. Conversely, diagnostic tests for non-IgE-mediated FA are infrequent and lack standardization [22]. Therefore, the data concerning the frequency of non-IgE-mediated FA in patients with AD remains inadequate [23,24]. One of the most important results of our study is that the rate of non-IgE-mediated FA was found to be 22.4%, closely approximating the ratio of IgE-mediated FA. These results indicate that in young children with AD, the existence of non-IgE-mediated FA symptoms should be disclosed with a detailed investigation.
The literature lacks definitive data regarding the concurrent IgE- and non-IgE-mediated FA in children with AD [7]. This coexistence was observed in 12.0% of individuals. We would like to emphasize that, in addition to immediate reactions, symptoms such as blood and/or mucus in the stool, vomiting, and colic should be considered for the risk of non-IgE-mediated FA in AD patients.
Although the prevalence of food sensitization among children with AD has been reported to range from 47% to 66% in the literature, it is known that the frequency of allergy is lower [25,26,27]. Our study found that 27% of patients without FA exhibited sIgE/SPT positivity, despite negative FCT results. The FCT test, which is the gold standard in the diagnosis of FA, is strongly recommended to diagnose true FA and to prevent unnecessary food elimination and adverse clinical outcomes, especially in AD patients with food sensitivity [22]. FCT decisions may not always be straightforward for individuals and healthcare professionals. Therefore, it is essential to identify who is at high risk for FA [28]. The risk of FA is known to rise in the presence of early-onset and moderate-to-severe AD [29,30]. We established that the presence of blood in stool was the most significant risk factor for FA, alongside early-onset and moderate-to-severe AD.
The main strengths of the study are its multicenter prospective design, extensive sample size, and the confirmation of FA by pediatric allergy specialists with FCT. The simultaneous evaluation of immediate and late-onset symptoms is another strength. Open FCTs may be regarded as a drawback; however, the patients in our study sample were under 2 years of age, allowing for objective assessment of FCTs in this demographic. The fact that our study population consisted of AD patients under 24 months of age could be considered a limitation. But we aimed to contribute to the literature in this area due to the higher prevalence of the association between AD and FA in this age group.
6. Conclusions
Our research offers important insights about the concomitant FA phenotypes in children with AD in early childhood. Children with early-onset and mild-to-moderate AD should be thoroughly investigated for FA symptoms. Diagnosing true FA is crucial in order to avoid unnecessary food elimination and negative clinical consequences, particularly in AD patients who have food sensitivity. The findings of the study suggest that the primary indicators of concomitant FA in AD patients were the presence of blood in stool and severe AD. We underline that it is important to consider that children with AD who exhibit IgE-mediated FA may also have concurrent non-IgE-mediated FA. Addressing these symptoms may assist healthcare practitioners in clinical practice to improve the quality of care for AD patients having FA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Domínguez O. Plaza A.M. Alvaro M. Relationship Between Atopic Dermatitis and Food Allergy Curr. Pediatr. Rev.20201611512210.2174/157339631566619111112243631713486 · doi ↗ · pubmed ↗
- 2Samady W. Warren C. Kohli S. Jain R. Bilaver L. Mancini A.J. Gupta R. The prevalence of atopic dermatitis in children with food allergy Ann. Allergy Asthma Immunol.201912264766510.1016/j.anai.2019.03.01930922954 PMC 7898751 · doi ↗ · pubmed ↗
- 3Sitarik A.R. Eapen A.A. Biagini J.M. Jackson D.J. Joseph C.L.M. Kim H. Martin L.J. Rivera-Spoljaric K. Schauberger E.M. Wegienka G. Phenotypes of Atopic Dermatitis and Development of Allergic Diseases JAMA Netw. Open 20258 e 251509410.1001/jamanetworkopen.2025.1509440504529 PMC 12163678 · doi ↗ · pubmed ↗
- 4Tedner S.G. Asarnoj A. Thulin H. Westman M. Konradsen J.R. Nilsson C. Food allergy and hypersensitivity reactions in children and adults—A review J. Intern. Med.202229128330210.1111/joim.1342234875122 · doi ↗ · pubmed ↗
- 5AAAAI/ACAAI JTF Atopic Dermatitis Guideline Panel Chu D.K. Schneider L. Asiniwasis R.N. Boguniewicz M. De Benedetto A. Ellison K. Frazier W.T. Greenhawt M. Huynh J. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on practice parameters GRADE– and Institute of Medicine–based recommendations Ann. Allergy Asthma Immunol.202413227431210.1016/j.anai.2023.11.00938108679 · doi ↗ · pubmed ↗
- 6Venter C. Halken S. Toniolo A. Nowak-Wegrzyn A. Vlieg-Boerstra B. Nilsson C.A. Fleischer D.M. de Silva D. Barber D. Khaleva E. Global Network of Centres of Excellence for Anaphylaxis & Food Allergy—AN Acare. Diagnosing Ig E-mediated food allergy: How to apply the latest guidelines in clinical practice J. Allergy Clin. Immunol. Glob.2025410055610.1016/j.jacig.2025.10055640989752 PMC 12452672 · doi ↗ · pubmed ↗
- 7Meyer R. Chebar Lozinsky A. Fleischer D.M. Vieira M.C. Du Toit G. Vandenplas Y. Dupont C. Knibb R. Uysal P. Cavkaytar O. Diagnosis and management of Non-Ig E gastrointestinal allergies in breastfed infants—An EAACI Position Paper Allergy 202075143210.1111/all.1394731199517 · doi ↗ · pubmed ↗
- 8Langan S.M. Irvine A.D. Weidinger S. Atopic dermatitis Lancet 202039634536010.1016/S 0140-6736(20)31286-132738956 · doi ↗ · pubmed ↗