SUMF1 Common Variant rs793391 Is Associated with Response to Inhaled Corticosteroids in Patients with COPD
Charikleia Ntenti, Eleni Papakonstantinou, Leticia Grize, Maria Pascarella, Björn C. Frye, Sebastian Fähndrich, Despoina Ioannidou, Spasenija Savic Prince, Antonis Goulas, Daiana Stolz

TL;DR
A genetic variant in SUMF1 is linked to better lung function improvement in COPD patients using inhaled corticosteroids.
Contribution
Identifies a SUMF1 SNP (rs793391) associated with ICS response and COPD progression, suggesting potential for personalized treatment.
Findings
rs793391 heterozygotes showed significant FEV1 improvement with ICS treatment.
Improved patient-reported outcomes were observed in rs793391 heterozygotes.
The variant may influence COPD progression and treatment response.
Abstract
This study investigated whether specific sulfatase modifying factor-1 (SUMF1) SNPs—previously linked to lung function—are associated with COPD progression and response to inhaled corticosteroid (ICS) treatment, specifically budesonide, given that SUMF1 expression is altered in COPD and its variants linked to increased disease risk. A subgroup of 165 COPD patients from the HISTORIC study were genotyped for two common SUMF1 SNPs, rs11915920 and rs793391. Patients first underwent a six-week run-in phase with open-label triple inhaled therapy (LAMA/LABA/ICS), then were randomized to receive either LAMA/LABA/placebo or LAMA/LABA/ICS for 12 months. Associations between SNPs, baseline characteristics, and response to ICS—based on FEV1 change over 12 months—were evaluated. Heterozygotes (TG) for the rs793391 polymorphism treated with LAMA/LABA/ICS showed a significant and clinically meaningful…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
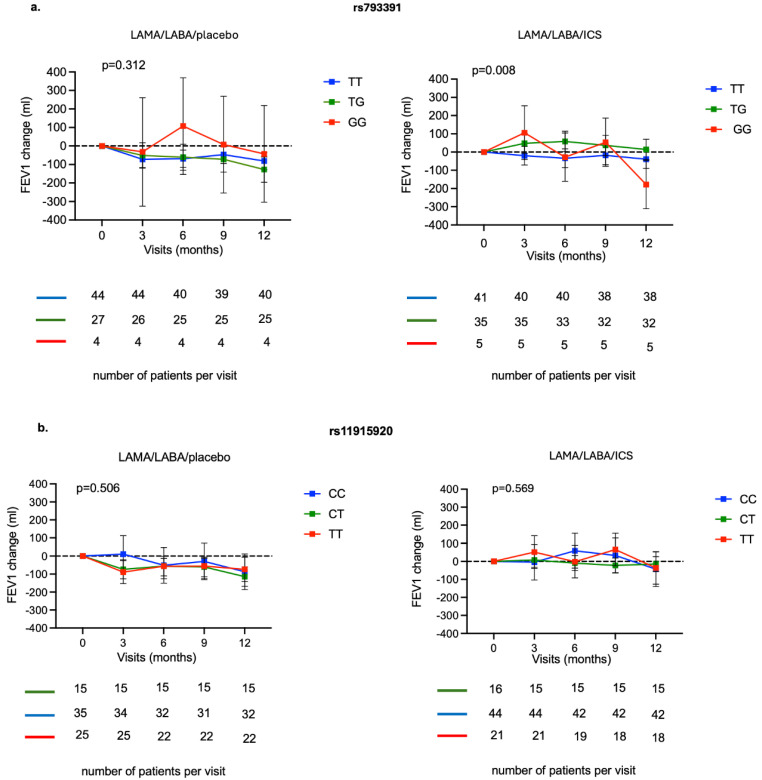 Figure 1
Figure 1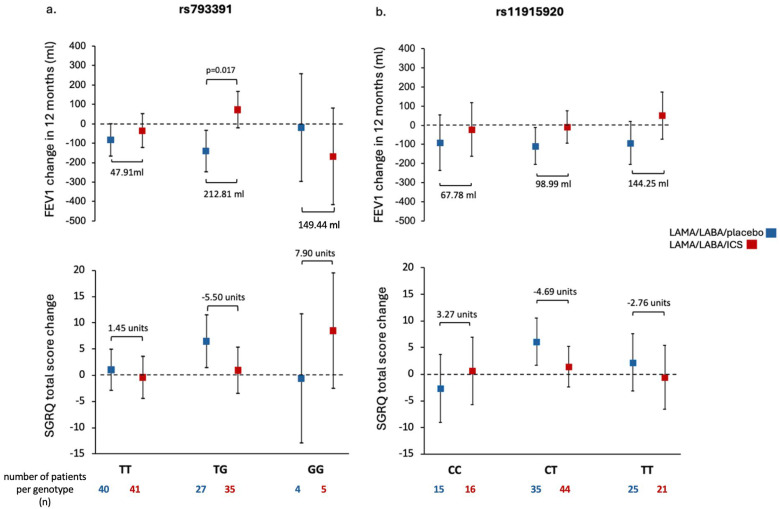 Figure 2
Figure 2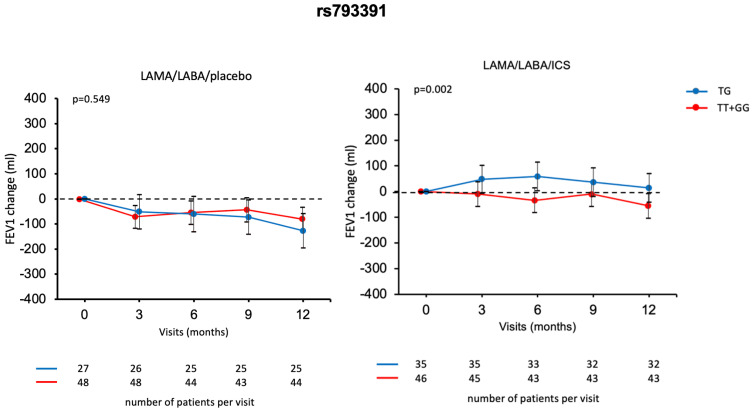 Figure 3
Figure 3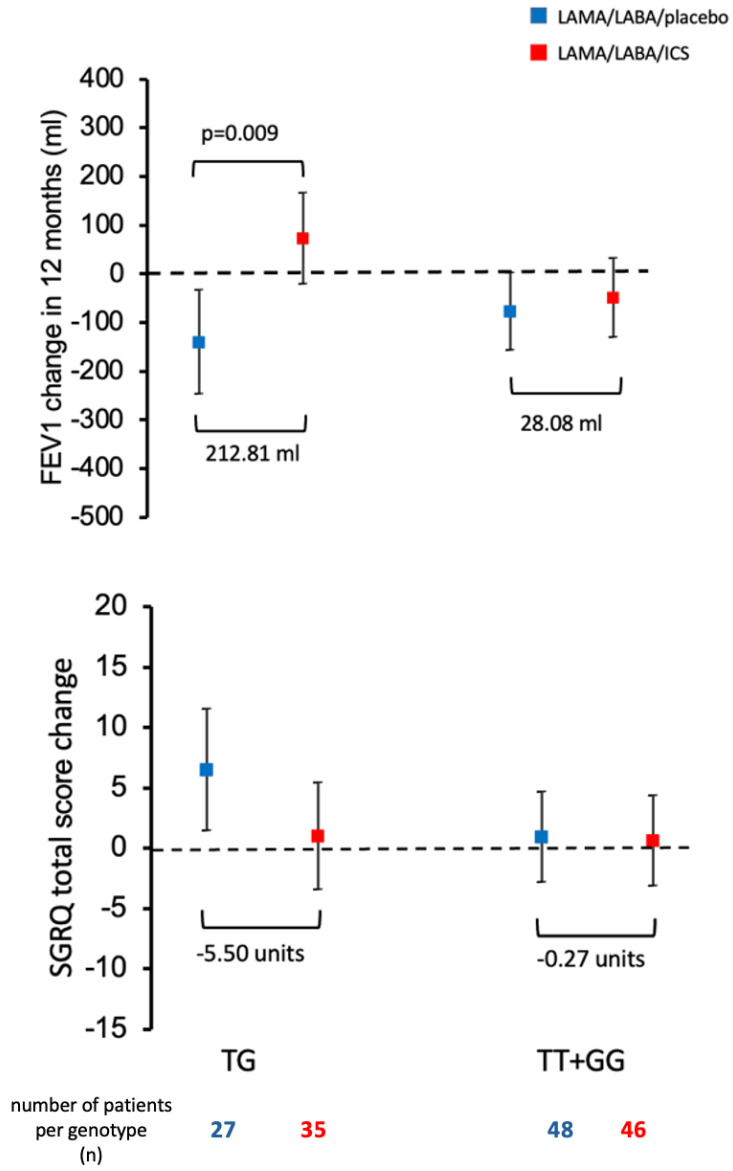 Figure 4
Figure 4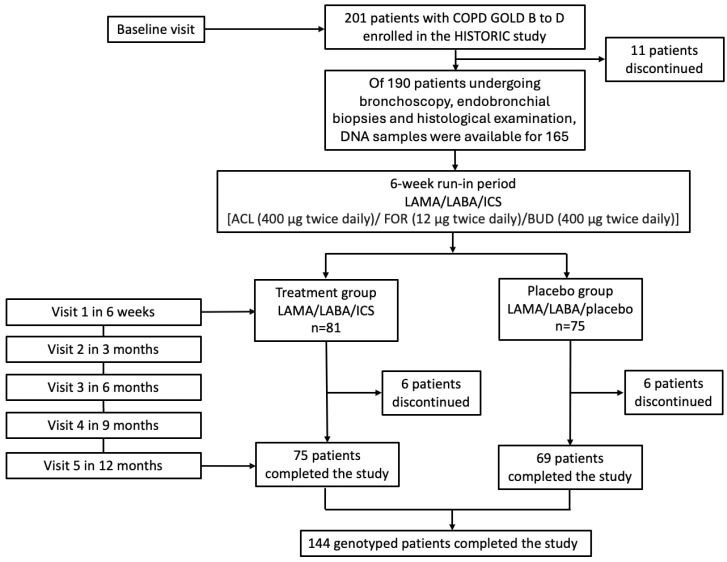 Figure 5
Figure 5- —Astra Zeneca
- —Clinic of Pneumology, University Hospital Basel, Switzerland
- —Swiss National Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Pulmonary Hypertension Research and Treatments · Neonatal Respiratory Health Research
1. Introduction
Recent investigations have focused on identifying the genetic underpinnings of Chronic Obstructive Pulmonary Disease (COPD) to improve our understanding of the disease and its progression. Using genome-wide association studies (GWAS) and whole-genome sequencing, researchers have identified various genes and single nucleotide polymorphisms (SNPs) associated with COPD [1,2,3]. Inhaled corticosteroids (ICS) are the most used and effective treatment for asthma [4]. However, COPD patients often do not respond as well to ICS, likely due to genetic factors. Furthermore, glucocorticoid unresponsiveness in COPD hampers effective treatment [5]. ICS in COPD patients unresponsive to treatment may lead to increased risks of pneumonia, oral thrush, increased exacerbations, and systemic side effects without improving outcomes [6,7,8,9]. Long-term ICS use also increases the risk of pneumonia, oral candidiasis, and dysphonia [10]. Therefore, understanding the genetic factors influencing the ICS response in COPD patients could enable physicians to personalize treatment decisions and action plans for individual patients.
Sulfatases are enzymes that modify proteoglycan chains through the removal of sulfate groups and are, thus, critical for extracellular matrix (ECM) remodeling. All sulfatases are regulated by the sulfatase modifying factor 1 gene (SUMF1), several polymorphisms of which have been associated in the past with predisposition to COPD [11]. SUMF1, the protein product of SUMF1, displays a formylglycine-generating enzymatic activity catalyzing a post-translational modification of sulfatases required for full activity (11). Mutations in SUMF1 are a leading cause of a variety of human diseases, many of them causing detrimental effects in the lungs [12]. It is well-established that the impaired expression of SUMF1 can cause lung function decline by affecting alveoli, related to an overabundance of sulfated glycosaminoglycans (GAGs) deposited in the ECM [13]. Thus, SUMF1 polymorphisms could conceivably be associated with lung function and clinical characteristics of COPD patients [14]. In the present study, we explore the association of two SUMF1 common single nucleotide polymorphisms (SNPs) with lung function characteristics, histological and biochemical parameters, and response to therapy based on annual FEV1 change and health-related quality of life (QoL) data in a group of patients with COPD.
2. Results
2.1. Patients’ Characteristics, Genotype and Allele Frequencies
The study involved 165 Caucasian patients, 31.1% of whom were females, with a median age of 67 years (range 59–72 years). These patients had a smoking history of an average of 50 pack-years (range 37–70 pack-years) and had been living with the disease for an average of 60 months (range 23–120 months). Their post-bronchodilator FEV1% predicted value was 59% (range 49–67%), and their post-bronchodilator diffusing capacity for carbon monoxide (DLCO SB)% predicted value was 61.5% (range 48–78%) (Table 1).
Table 2 displays the genotype and allele frequencies of the rs11915920 and rs793391 polymorphisms in the SUMF1 gene. The genotype distributions were consistent with the Hardy–Weinberg equilibrium, as indicated by both p values being greater than 0.88 (Table 2). LD analysis showed that rs11915920 and rs793391 are not in strong linkage disequilibrium (r^2^ = 0.145, D = –0.39), consistent with their independent distribution in our cohort.
2.2. Association of SUMF1 Polymorphisms with Lung Function, Histological and Blood-Sampling Parameters at Baseline
There were no significant associations of the rs11915920 and rs793391 polymorphisms with any of the lung function parameters at baseline (Supplementary Table S2).
Patients homozygous for the SUMF1 rs11915920 (TT) exhibited a higher eosinophil tissue infiltration (p = 0.006) (Supplementary Table S3). Rs11915920 heterozygotes (CT) had significantly lower values of ASMC area, assessed in endobronchial biopsies (p = 0.015) (Supplementary Figure S1 and Table S3).
Patients heterozygous for the SUMF1 rs11915920 (CT) presented with higher blood neutrophils (p = 0.013) (Supplementary Table S4). Blood eosinophils were marginally higher in patients homozygous for the reference allele (TT) of SUMF1 rs793391 (p = 0.050) (Supplementary Table S4).
2.3. Association of SUMF1 Polymorphisms with Response to Treatment with ICS
FEV1 change over 12 months was similar in all genotypes of the rs793391 and rs11915920 polymorphisms when patients were receiving LAMA/LABA/placebo (Figure 1a,b). However, for COPD patients receiving LAMA/LABA/ICS there was a significant impact of the rs793391 polymorphism on FEV1 change over 12 months (p = 0.008) (Figure 1a).
Further analysis between the treatment groups revealed significant differences in FEV1 change over 12 months between patients treated with LAMA/LABA/placebo and those on LAMA/LABA/ICS across the various genotypes of rs793391. Heterozygous individuals (TG) receiving LAMA/LABA/ICS demonstrated a significant, mean increase in FEV1 of 71.8 mL (95% CI: −22.1–165.6 mL) after 12 months of treatment, that is, 212.8 mL more compared to patients who were given LAMA/LABA/placebo (95% CI: −247.9–34.2 mL) (p = 0.017). Patients homozygous for the alternative allele (GG) who underwent triple therapy (LAMA/LABA/ICS) exhibited a decrease in FEV1, with an adjusted mean loss of 149.44 mL compared to patients treated with LAMA/LABA/placebo (Figure 2a).
Consistent with the previously presented FEV1 changes, TG carriers of the rs793391 genotype who received LAMA/LABA/ICS treatment showed a mean, clinically meaningful reduction of 5.5 units in the SGRQ total score compared to those with the same genotypes receiving LAMA/LABA/placebo over 12 months (Figure 2a). Although statistical significance was not reached, similar trends were observed in the CAT and SF-36 General Health scores: TG carriers treated with LAMA/LABA/ICS tended to have lower, mean CAT scores (−2.68 units) and higher, mean SF-36 scores compared with those on LAMA/LABA/placebo, suggesting a potential benefit of triple therapy in this genotype subgroup (Table 3 and Table 4).
To explore the genetic architecture of rs793391 and ICS responsiveness, both dominant and over-dominant inheritance models were assessed. In the dominant model (TT vs. TG + GG), ICS treatment was associated with a statistically significant improvement in FEV_1_ slope (p = 0.004) (Supplementary Figure S2a) and absolute change (mL) in carriers of the G allele (p = 0.038) (Supplementary Figure S3a). However, this effect appeared to be driven primarily by heterozygous TG individuals, as the number of GG homozygotes was very small (n = 9) and insufficient to influence the model independently.
To further explore the association between rs793391 and ICS response, we applied an over-dominant model (TG vs. TT + GG). As shown in Figure 3, this model confirmed the findings from the main analysis and revealed a significant treatment effect for the ICS group. Specifically, TG carriers exhibited a significantly greater improvement in FEV_1_ over the 12-month period when treated with LAMA/LABA/ICS compared to LAMA/LABA/placebo (p = 0.002). No significant differences were observed between the genotype groups in the placebo arm (p = 0.549), suggesting that the beneficial effect of ICS was specific to the TG genotype.
Consistent with the trajectory plots, slope-based regression analysis (Figure 4) further demonstrated that TG carriers in the ICS group had a statistically significant increase in FEV_1_ over time compared to TT + GG carriers. Additionally, a meaningful reduction in SGRQ total score was observed for TG carriers receiving ICS, exceeding the threshold for clinically relevant improvement (≥4 units). These findings support a genotype-specific response to ICS treatment, both in terms of lung function and health-related quality of life.
The recessive model (GG vs. TT + TG) did not yield statistically significant associations for FEV_1_ or SGRQ outcomes, which is not surprising given the very small number of GG homozygotes in our cohort (n = 9, 4 and 5 per treatment group), precluding meaningful analysis (Supplementary Figures S2b and S3b).
The response to treatment in patients with various genotype combinations was further explored. Combinations of SNPs were considered only if each combination had five or more patients for each treatment group. Heterozygotes for both SNPs (CT/TG) exhibited a significantly better response (p = 0.039) to treatment with LAMA/LABA/ICS (median improvement 17.1 mL, IQR: −96.4–128.3 mL) compared with patients with the same genotypes who received LAMA/LABA/placebo (median loss of 59.4 mL, IQR: −172.9–−35.1 mL) (Supplementary Figure S2).
To explore potential genotype-specific effects on exacerbation risk, adjusted annual AECOPD exacerbation rates were analyzed in relation to rs793391 genotype and treatment allocation. Overall, exacerbation rates were relatively low in both treatment arms, which may limit statistical power and the reliability of comparisons. Among patients in the ICS group, TG carriers exhibited the lowest exacerbation rate (0.61 [95% CI: 0.30–0.92]), with a statistically significant difference compared to GG carriers (1.67 [95% CI: 0.85–2.49], p = 0.036), while the difference compared to TT carriers (0.76 [95% CI: 0.48–1.05]) was not significant (p = 0.720). In the placebo group, no significant differences in exacerbation rates were observed across genotypes: TG carriers had a rate of 1.05 (95% CI: 0.65–1.45), compared to 0.87 (95% CI: 0.55–1.18) in TT carriers (p = 0.711) and 0.46 (95% CI: –0.58–1.49) in GG carriers (p = 0.483) (Supplementary Table S5).
COPD patients carrying the rs11915920 variant and receiving LAMA/LABA/ICS showed a mean improvement in FEV_1_ over 12 months of 68 mL, 99 mL, and 144 mL for CC, CT, and TT genotypes, respectively, compared with patients receiving LAMA/LABA/placebo. Among these, only TT carriers treated with ICS demonstrated a net gain in FEV_1_; however, this improvement did not reach statistical significance (Figure 2b). In terms of patient-reported outcomes, only heterozygous CT carriers receiving LAMA/LABA/ICS showed a marginally clinically relevant improvement, with a mean reduction of 4.7 units in SGRQ total score compared to placebo (Figure 2b). Additionally, TT carriers showed a trend toward improved general health, with a mean increase of 5.97 units in the SF-36 General Health score. However, no clinically meaningful differences were observed in SGRQ or CAT scores within this subgroup (Table 3 and Table 4).
3. Discussion
The present study examined two SNPs, rs11915920 and rs793391, within the SUMF1 gene that were previously associated with COPD prevalence and altered lung function. Our findings suggest that the rs793391 SUMF1 polymorphism may influence the response to treatment with ICS, particularly budesonide, combined with LAMA/LABA, in a well-characterized cohort from the HISTORIC study. Additional analyses using different inheritance models, particularly the dominant and over-dominant models, reinforced this observed pharmacogenetic association.
At baseline, there were no significant differences in lung function characteristics among different genotypes of the rs11915920 and the rs793391 polymorphisms. However, a statistically significant and clinically meaningful association emerged between rs793391 and ICS treatment at the end of the 12-month study. TG carriers receiving triple therapy showed a mean FEV1 improvement of 212.8 mL compared to those in the placebo group. To better understand this association, we further explored alternative genetic models. The dominant model (TG + GG vs. TT) revealed statistically significant treatment–genotype interactions, primarily driven by the TG subgroup, as GG carriers were rare (n = 9). The over-dominant model confirmed this trend, while the recessive model (GG vs. TT + TG) lacked statistical power due to low sample size and is of limited interpretive value.
In our study, TG carriers of rs793391 (n = 35) responded significantly better to LAMA/LABA/ICS treatment compared to the other two genotypes (n = 46) who received either triple or dual therapy. This pattern is consistent with a potential heterozygote advantage, where individuals with the TG genotype derive greater therapeutic benefit than either homozygous group. Conversely, GG carriers demonstrated less favorable outcomes when treated with ICS, including a decline in FEV1 and deterioration in health-related quality of life over 12 months, raising the hypothesis that ICS may be detrimental in this genotype. Although limited by the small sample size of this group, these observations warrant further investigation.
In a previous population-based cohort study of both COPD patients and controls, Jarenbäck et al. showed that there is a link of multiple SNPs in SUMF1 with COPD prevalence, identifying rs793391 as a particularly significant variant [15]. In their study, a group of genetic variations in the SUMF1 gene were associated with COPD prevalence and differences in lung function parameters such as FEV1 and FEV1/FVC. Specifically, it was found that TG carriers had significantly higher FEV1% predicted and FEV1/FVC ratios compared to homozygous individuals. However, such associations were not replicated in our cohort, likely due to differences in study populations: our study enrolled only moderate-to-severe COPD patients (grades B–D), while theirs included healthy individuals and patients with varying disease severity [15].
We also examined whether rs793391 genotypes influenced exacerbation risk. Overall, the exacerbation rate was low across both treatment arms, likely reflecting the clinical trial setting and stable patient population. Although no statistically significant differences were observed, TG carriers treated with ICS had numerically fewer exacerbations (0.61 vs. 0.76 events/year) than TT carriers, with a p-value of 0.06, suggesting a trend that may merit further investigation. Due to the low number of exacerbations and absence of emergency visit data, these findings should be interpreted with caution.
While there is an established association between rs793391 and SUMF1 expression [16], the specific molecular mechanisms connecting it to COPD are still undefined. Considering its intronic location, it is conceivable that this SNP could serve as a precursor for small RNA molecules, like microRNA, suggesting an avenue for further investigation into its functional role.
Our study has several limitations. First, the absence of a second, independent validation cohort and the relatively small sample size (n = 165), which may reduce statistical power and contribute to false negatives. Post hoc power analysis indicated ~80% power to detect a 150 mL difference in FEV1 change, consistent with the minimal clinically important difference (MCID) in COPD [17], but smaller genetic effects may have gone undetected. Second, all patients received budesonide as the ICS component, and our findings may not generalize to other ICS compounds with different pharmacokinetic or pharmacodynamic profiles. Third, the low exacerbation rate and limited number of GG carriers reduce the reliability of some subgroup analyses.
Despite these limitations, the study has important strengths. It is based on a well-characterized randomized cohort, and combines robust clinical outcomes (FEV1, QoL) with genetic data. The results highlight a potential role for pharmacogenetic testing in identifying COPD patients most likely to benefit from ICS therapy.
While the prospect of SUMF1 genotyping is attractive, practical considerations such as cost, turnaround time, and clinical feasibility must be addressed. Furthermore, validation in larger, ethnically diverse populations is necessary to confirm the utility of these findings. The impact of SUMF1 on lung physiology is well-established [15,16]. Additionally, the effect of rs793391 on various lung function characteristics is evident, as demonstrated by consistent studies showing its association with lung function and COPD across diverse groups, including healthy active smokers, former smokers, and even never-smokers. Our findings further extend its impact to treatment response with LAMA/LABA/ICS. If independently confirmed, this outcome (i) suggests the clinical usefulness of genotyping the rs793391 polymorphism to predict response to ICS and (ii) underscores the genetic influence on the expression and sulfation pattern of GAGs, highlighting their role in COPD and airway remodeling diseases in general.
Our findings contribute to the expanding field of COPD pharmacogenetics by highlighting a novel association between the SUMF1 rs793391 polymorphism and clinical response to ICS treatment. While prior studies have largely focused on genes involved in glucocorticoid signaling—such as GLCCI1 and FKBP5 [18,19]—with inconsistent replication, limited attention has been given to genes related to lung structure and tissue remodeling. In our recent review [20], we underscored the lack of validated pharmacogenetic markers in COPD and the challenges in translating such findings into clinical practice. By investigating SUMF1, a gene previously linked to COPD risk and altered lung expression, this study addresses a key gap.
In summary, our results point to a potential pharmacogenetic marker for ICS responsiveness in COPD, although the findings remain exploratory and hypothesis-generating. The observed genotype–treatment interactions on lung function trajectories and FEV_1_ changes are promising but should be interpreted with caution. Further validation in larger, independent cohorts with longer follow-up is needed to confirm the reproducibility, clinical relevance, and feasibility of incorporating SUMF1 genotyping into routine COPD management.
4. Materials and Methods
4.1. Study Population
The study included 165 patients diagnosed with COPD grades B-D as per the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, who were participants in the HISTORIC study, an investigator-initiated, double-blind, randomized, placebo-controlled trial conducted at the University Hospital of Basel, Switzerland [21]. Among the 190 participants who underwent bronchoscopy, endobronchial biopsies, and histological examination, DNA samples were available for 165 individuals, enabling pharmacogenetic analysis. Of these patints, 156 participated in the initial visit, and ultimately, 144 completed the study. Importantly, there was no evidence of selection bias in the availability of DNA samples, as the subset of 165 participants was representative of the overall study population in terms of key demographic and clinical characteristics (Figure 5).
Patients followed a 6-week run-in period on an open-label triple inhaled therapy consisting of aclidinium/formoterol/budesonide (ACL/FOR/BUD: 400/12/400 mcg/bid), after which they were randomized to receive either ACL/FOR/BUD or ACL/FOR/Placebo for 12 months. Ethical approval was granted by the institutional review board (EKNZ 2016-6-01880), and the trial was registered on 15/11/2016 with the International Standard Randomised Controlled Trial Number (ISRCTN11017699) [22], adhering to the Declaration of Helsinki and good clinical practice guidelines. Written informed consent for the analysis was obtained from all participants.
4.2. Sample Size and Power Justification
No formal a priori sample size calculation was performed for this pharmacogenetic sub-analysis, as it was conducted on the subset of 165 patients from the HISTORIC trial with available DNA samples. A post hoc power assessment indicated that, with approximately 82 patients in the LAMA/LABA/ICS group and 83 in the LAMA/LABA/placebo group, the study had ~80% power to detect a between-group difference in FEV_1_ change of 150 mL, assuming a standard deviation of 200 mL and a two-sided α = 0.05. This detectable difference aligns with the MCID commonly reported in COPD clinical trials [17].
4.3. DNA Extraction and Genotyping
Genomic DNA was extracted from the peripheral blood of participants using the QIAsymphony DSP DNA Kit (QIAGEN, Hilden, Germany), following the manufacturer’s protocol, and stored at −80 °C until genotyping. Genotyping of all SNPs was performed using real-time PCR and TaqMan chemistry, with probes designed via Primer Express software and produced by Applied Biosystems (ABI, Warrington, UK). Data analysis was conducted using SDS 2.0 software (ABI, Foster City, CA, USA).
4.4. Linkage Disequilibrium Analysis
To evaluate whether the two SNPs represent independent genetic signals, rs11915920 and rs793391, a linkage disequilibrium (LD) analysis was performed using binary presence of minor alleles (T for rs11915920 and G for rs793391) across the 165 genotyped individuals. LD estimates, including D and r^2^, were calculated from a 2 × 2 allele presence matrix using statsmodels (version 0.14.0) in Python.
4.5. Statistical Analysis
The study data were summarized using counts and percentages or medians with interquartile ranges. Categorical data were compared using Fisher’s exact test, and continuous data were analyzed using the Kruskal–Wallis test. The association between FEV1 change for each genotype from visit 1, treatment group, and visit number was assessed using a mixed-effects model. The treatment group and visit number (as categorical factors) were included as fixed effects, while the subject was treated as a random effect. Furthermore, changes in FEV1 over 12 months post-randomization were evaluated in a two-step process. Initially, changes for each patient were determined by linear regression of five FEV1 measurements, assuming the slope represented the change over time. Then, these slopes were analyzed based on treatment groups and genotype, with p-values adjusted for multiple comparisons using the Dunnett–Hsu method. The overall effect of treatment across polymorphisms was calculated. Health-related QoL improvement over 12 months was assessed using generalized linear models, examining the impact of treatment and genotype. Regression and mixed-effects models were adjusted for relevant clinical covariates (age, sex, baseline eosinophil count, smoking status [pack-years], and baseline FEV_1_) to minimize potential confounding. Deviations in genotype frequencies from the Hardy–Weinberg equilibrium were checked using the χ2 goodness-of-fit test, and comparisons of genotype and allele distributions were performed using the χ2 test of independence. An alpha error threshold of 0.05 was set for statistical significance. Analyses were performed using the Statistical Analysis System (SAS^®^ Institute, Cary, NC, USA), IBM SPSS Statistics (Version 28), and RStudio Team (Version 2021.09.0+351; Ghost Orchid).
5. Conclusions
In this study, we provide evidence that the rs793391 polymorphism in SUMF1 may be associated with differential response to ICS treatment, in particularly budesonide, in COPD patients receiving LAMA/LABA. Heterozygous carriers (TG) showed a favorable response to ICS when added to LAMA/LABA, as indicated by a significant improvement in FEV_1_ over 12 months. These patients also experienced a reduction in SGRQ total scores, along with improvements in CAT and General Health scores, compared to those receiving LAMA/LABA/placebo. This is the first study to link SUMF1 genetic variants to treatment response in a well-characterized COPD cohort within the setting of a randomized controlled trial. While promising, these findings should be considered exploratory and hypothesis-generating, warranting validation in larger, independent cohorts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pillai S.G. Ge D. Zhu G. Kong X. Shianna K.V. Need A.C. Feng S. Hersh C.P. Bakke P. Gulsvik A. A genome-wide association study in chronic obstructive pulmonary disease (COPD): Identification of two major susceptibility loci P Lo S Genet.20095 e 100042110.1371/journal.pgen.100042119300482 PMC 2650282 · doi ↗ · pubmed ↗
- 2Cho M.H. Mc Donald M.L. Zhou X. Mattheisen M. Castaldi P.J. Hersh C.P. Demeo D.L. Sylvia J.S. Ziniti J. Laird N.M. Risk loci for chronic obstructive pulmonary disease: A genome-wide association study and meta-analysis Lancet Respir. Med.2014221422510.1016/S 2213-2600(14)70002-524621683 PMC 4176924 · doi ↗ · pubmed ↗
- 3Cho M.H. Castaldi P.J. Hersh C.P. Hobbs B.D. Barr R.G. Tal Singer R. Bakke P. Gulsvik A. San Jose Estepar R. Van Beek E.J. A Genome-Wide Association Study of Emphysema and Airway Quantitative Imaging Phenotypes Am. J. Respir. Crit. Care Med.201519255956910.1164/rccm.201501-0148 OC 26030696 PMC 4595690 · doi ↗ · pubmed ↗
- 4Barnes P.J. Inhaled corticosteroids are not beneficial in chronic obstructive pulmonary disease Am. J. Respir. Crit. Care Med.20001613423441067316610.1164/ajrccm.161.2.16125_2 · doi ↗ · pubmed ↗
- 5Yang I.A. Ferry O.R. Clarke M.S. Sim E.H. Fong K.M. Inhaled corticosteroids versus placebo for stable chronic obstructive pulmonary disease Cochrane Database Syst. Rev.20233 CD 00299110.1002/14651858.cd 002991.pub 436971693 PMC 10042218 · doi ↗ · pubmed ↗
- 6Anzueto A.R. Kostikas K. Mezzi K. Shen S. Larbig M. Patalano F. Fogel R. Banerji D. Wedzicha J.A. Indacaterol/glycopyrronium versus salmeterol/fluticasone in the prevention of clinically important deterioration in COPD: Results from the FLAME study Respir. Res.20181912110.1186/s 12931-018-0830-z 29925383 PMC 6011394 · doi ↗ · pubmed ↗
- 7Bhatt S.P. Anderson J.A. Brook R.D. Calverley P.M.A. Celli B.R. Cowans N.J. Crim C. Martinez F.J. Newby D.E. Vestbo J. Cigarette smoking and response to inhaled corticosteroids in COPD Eur. Respir. J.201851170139310.1183/13993003.01393-201729348179 · doi ↗ · pubmed ↗
- 8Barnes P.J. Adcock I.M. Glucocorticoid resistance in inflammatory diseases Lancet 20093421905191710.1016/S 0140-6736(09)60326-319482216 · doi ↗ · pubmed ↗