Early-Life Exposure to Organic Chemical Pollutants as Assessed in Primary Teeth and Cardiometabolic Risk in Mexican American Children: A Pilot Study
Vidya S. Farook, Feroz Akhtar, Rector Arya, Alice Yau, Srinivas Mummidi, Juan C. Lopez-Alvarenga, Alvaro Diaz-Badillo, Roy Resendez, Sharon P. Fowler, Hemant Kulkarni, Vijay Golla, Mahua Choudhury, Jane L. Lynch, Donna M. Lehman, Daniel E. Hale, Ralph A. DeFronzo, John Blangero

TL;DR
This pilot study explores how early-life exposure to organic chemicals in Mexican American children may affect their cardiometabolic health.
Contribution
The study is among the first to assess organic chemical exposure in primary teeth and its link to cardiometabolic risk in Mexican American children.
Findings
MiBP was positively correlated with fat mass, fasting insulin, and insulin resistance in MA children.
APAP showed a strong negative correlation with HDL-C and a positive association with triglycerides.
MnBP and MEHP exhibited negative correlations with blood pressure and triglycerides, respectively.
Abstract
Early-life exposure to organic chemicals (OCs) may influence childhood obesity and associated cardiometabolic risk. These conditions have been shown to disproportionately affect minority populations such as Mexican Americans (MAs). However, information on the impact of organic chemicals on cardiometabolic risk in MA children is limited. Therefore, we conducted a pilot study to assess the extent to which exposure to organic chemicals influences cardiometabolic traits (CMTs) in MA children. We recalled 25 children from a previous study and collected 25 primary teeth from them. Chemical analyses of the teeth were performed using established protocols. Target analytes included acetaminophen (APAP); 3,5,6-trichloro-2-pyridinol (TCPy), 2-isopropyl-6-methyl-4-pyrimidinol (IMPy), diethyl phosphate (DEP), N,N-diethyl-m-toluamide (DEET), tris(2-butoxyethyl) phosphate (TBOEP), monoethyl phthalate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
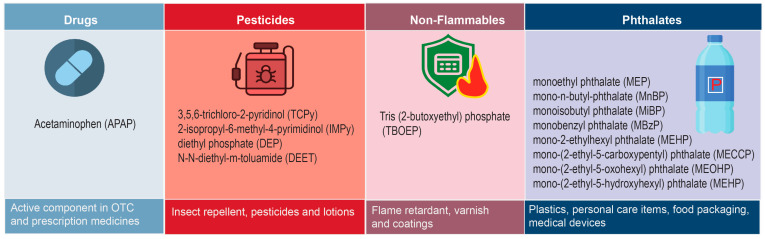 Figure 1
Figure 1- —National Center for Advancing Translational Sciences, National Institutes of Health (NIH)
- —AT&T Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · Child Nutrition and Water Access · Health, Environment, Cognitive Aging
1. Introduction
Childhood obesity is associated with both short- and long-term inimical health consequences. Rapid weight gain during infancy tracks well into adulthood, increasing the risk of type 2 diabetes (T2D), cardiovascular disease (CVD), and metabolic syndrome (MS), which refers to the clustering of cardiometabolic abnormalities including obesity, insulin resistance, dyslipidemia and hypertension, as well as premature mortality and disability later in life [1,2,3,4,5,6]. The prevalence of childhood obesity has accelerated during the past few decades, and it has become a new pandemic, leading to a widespread global health crisis [7,8,9,10,11]. In the United States (US), disparities in obesity rates are significantly evident, with higher prevalence among children and adolescents from disadvantaged backgrounds. Obesity rates among Hispanic adults and children are dramatically higher than those among non-Hispanic whites [12]. For example, based on the National Health and Nutrition Examination Survey 2017-March 2020, among adults aged 20 years and above, obesity prevalence in non-Hispanic whites was 41.4% compared to 49.9% in non-Hispanic blacks, 45.6% in Hispanics, and 16.1% in non-Hispanic Asians; the prevalence among children and adolescents aged 2–19 years was highest among Hispanics (26.2%), followed by non-Hispanic blacks (24.8%), non-Hispanic white (16.6%), and non-Hispanic Asians (9.0%) [12]. Childhood obesity has multifactorial origins [13,14]. In addition to genetic determinants of obesity, dietary intake, sedentary lifestyle, stress, microbiota, social determinants, and other environmental factors contribute to the development of obesity [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. These determinants act at multiple levels during the pre-, peri- and post-natal stages, and can induce lifelong and often irreversible derangements in the offspring’s adiposity and metabolism [29,30,31,32,33]. In addition, numerous studies have identified organic chemicals (OCs) as contributing factors for increased rates of obesity and metabolic syndrome [34,35,36,37]. By dysregulating energy metabolism and upregulating adiposity, these compounds act as obesogens (e.g., endocrine disruptors) [38,39,40]. Up to 20 different chemical classes are hypothesized to be obesogenic; these include persistent organic pollutants (POPs) and other compounds such as polychlorinated biphenyls (PCBs), hexachlorobenzene (HCB), dichlorodiphenyldichloroethylene (DDE), phthalates, bisphenol A (BPA), perfluoroalkyl substances (PFAS) and triclosan [39,41,42,43]. In addition, the OC acetaminophen (APAP) which is a widely used over-the-counter antipyretic and analgesic agent; and early-life exposures to APAP or its metabolites were found to be associated with childhood overweight or obesity [44,45,46].
Findings from several cross-sectional studies show positive association of POPs and OCs with T2D and obesity related traits in the general US population [37,47,48,49,50,51]. However, few longitudinal studies have examined the associations between early-life exposures to OCs and subsequent childhood obesity [46,52,53]. Current knowledge of exposures to low levels of OCs at critical periods of prenatal, perinatal, and postnatal development as they relate to childhood obesity and cardiometabolic risk is limited. Characterizing past exposures, especially during crucial periods, such as in utero and in early childhood, has been shown to be critical for assessing their impacts on health conditions later in life [54,55,56]. This being so, naturally shed primary teeth, due to their ability to sequester circulating semi-volatile organic compounds, offer a unique resource for measuring early-life exposures [54,55,56,57,58].
Early-life exposure to OCs could impact obesity and associated comorbid conditions such as T2D later in life, likely by altering energy metabolism and epigenetic regulation, with potential public health implications [59,60,61,62]. Therefore, we hypothesized that exposures to low levels of OCs during early life including the critical periods of prenatal, perinatal, and postnatal development, might be associated with obesity- and metabolic syndrome-related traits. To test this hypothesis, we carried out a pilot study, which measured the levels of 14 OCs in naturally shed primary teeth (Figure 1) from 25 Mexican American children and adolescents, to assess their association with childhood obesity and its related cardiometabolic traits (CMTs). These OCs represent common environmental and pharmaceutical exposures with relevance to potential disease risk, which were selected based on the published literature, particularly our own studies using established protocols that provided evidence that primary teeth can be valuable source of biomarkers of early-life exposures [63,64]. These children were participants in a previous study which revealed a high burden of overweight (53%), obesity (34%), prediabetes (13%), and metabolic syndrome (19%) [65].
2. Materials and Methods
2.1. Study Population
The data used for this study were related to 25 participants of the San Antonio Family Assessment of Metabolic Risk Indicators in Youth (SAFARI) study. SAFARI is a community-based family study designed to identify signs of metabolic syndrome and future disease risk in MA children and adolescents in San Antonio, TX and surrounding areas, and to examine their genetic basis [65]. As part of the SAFARI study, 673 children and adolescents, aged 6–17 years old, were recruited from large, predominantly lower-income MA families at increased risk of obesity and T2D, whose adult family members had previously participated in one of three community-based genetic epidemiological studies in San Antonio, TX: the San Antonio Family Diabetes/Gallbladder Study (SAFDGS), the San Antonio Family Heart Study (SAFHS), and the Veterans Administration Genetic Epidemiology Study (VAGES) [66,67,68]. Several demographic, anthropometric, and cardiometabolic traits were measured and environmental covariate data were collected as part of the SAFARI study. For this pilot study, the parents of SAFARI study participants were contacted by sending the project information (i.e., recruitment materials sent via mail) to collect primary teeth. There were no attempts to select children based on any clinical criteria (e.g., disease condition), and the children of the first 25 responders (i.e., parents of 25 children with available primary teeth) to the project request were recruited to assess the association of early-life exposure to low levels of OCs with risk of childhood obesity and related CMTs. All research procedures were approved by the Institutional Review Board of the University of Texas Health San Antonio, San Antonio, TX. Prior to the initiation of the study, informed written consent was obtained from either or both parents or the guardian of each child, and signed assent was obtained from children ≥ 7 years old.
2.2. Phenotypic Data
Data on obesity/CMTs used for this study were obtained using standard protocols as previously described by Fowler et al. 2013 [65]. Briefly, the following 13 CMTs were considered for this study: body mass index (BMI: weight [kg] divided by height [m] squared), waist circumference (WC), fat mass (FM: assessed by dual-energy-X-ray absorptiometry [DXA Hologic]), systolic (SBP) and diastolic blood pressure (DBP), fasting insulin (FI), glucose (FG), homeostasis model of assessment-insulin resistance (HOMA-IR, measured using FI and FG levels), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and aspartate aminotransferase/alanine aminotransferase ratio (AST/ALT ratio).
2.3. Tooth Preparation
Twenty five tooth crowns were pulverized and analyzed for the following 14 target analytes representing four distinct environmental sources (Figure 1): acetaminophen (APAP), 3,5,6-trichloro-2-pyridinol (TCPy), 2-isopropyl-6-methyl-4-pyrimidinol (IMPy), diethyl phosphate (DEP), N,N-diethyl-m-toluamide (DEET), tris(2-butoxyethyl) phosphate (TBOEP), monoethyl phthalate (MEP), mono-n-butyl phthalate (MnBP), monoisobutyl phthalate (MiBP), monobenzyl phthalate (MBzP), mono-2-ethylhexyl phthalate (MEHP), mono-(2-ethyl-5-carboxypentyl) phthalate (MECPP), mono-(2-ethyl-5-oxohexyl) phthalate (MEOHP), and mono-(2-ethyl-5-hydroxyhexyl) phthalate (MEHHP), using modified methods from Camann, Schultz et al. [63]. Each primary tooth crown type was identified by the study dentist who is part of this study (SC). Briefly, the crown of each exfoliated tooth was severed at the cementoenamal junction; pulp was scraped out, and any fillings, attached roots and/or cavities crown were removed with dental post-extraction tools (scalpel, engraving tool and heatless wheel). Each crown sample was placed in 1 mL of dichloromethane (DCM) and gently swirled to remove possible contamination during sample collection and preparation. The DCM-washed tooth crown was then pulverized with a mortar and pestle to a fine powder, and the powder weighed. The DCM used for the wash was retained as a quality measure to evaluate external tooth contamination.
2.4. Extraction and Analysis by Liquid Chromatograpgy-Tandem Mass Spectrometry (LC/MS/MS)
To determine target analytes approximately 25 mg of pulverized tooth sample was used in the extraction procedure [63]. Each pulverized tooth aliquot was spiked with 50 μL of labeled internal standards (labeled as APAP and MEHP surrogate) before extraction. To enhance the extraction efficacy of analytes, each aliquot of tooth was extracted under neutral and acidic conditions. The first neutral extraction employed sonication with 1 mL acetonitrile for 1 h followed by centrifugation at 3000 rpm for 5 min. The supernatant was concentrated to 25 μL and transferred to a new vial. For acidic extraction 50 μL of glacial acetic acid was added to each tooth sample aliquot and equilibrated overnight. A second extraction by repeating the acetonitrile sonication extraction was performed. The concentration of the target analytes in each powdered tooth extract was determined by high performance liquid chromatography (HPLC)/MS/MS in multiple reaction monitoring (MRM) mode with electrospray ionization. It should be noted that no biomarker validation study of OC measurement in primary teeth as we suggested [63] has yet been performed.
2.5. Statistical Analysis
The descriptive statistics and assessment of the bivariate Pearson correlations between the OCs and obesity/CMTs were carried out using the Statistical Package for the Social Sciences (SPSS) software(IBM SPSS Statistics 25). Prior to performing the correlation analyses, all obesity/CMTs were adjusted for the covariate effects of age and sex, for consistency and comparability across the models. The trait-specific residuals (i.e., residual phenotype), after accounting for the influences of age and sex through a regression analysis, were inverse normalized to address the issue of non-normality. Regarding the OCs, a similar approach was applied, but tooth type (i.e., incisor, canine, first molar, and second molar as dummy variables) was included as an additional covariate to account for differential exposure histories captured by different teeth. The trait-specific residuals (i.e., residual phenotype), after controlling for the influences of age, sex, and tooth type through a regression analysis, were inverse normalized to address the issue of non-normality. The trait-specific inverse normalized residual values were then used to obtain the bivariate Pearson correlations between OCs and obesity/CMTs (i.e., residual phenotypes). Given the pilot nature of this study, all significant (p ≤ 0.05) and suggestive (p < 0.10) correlations were considered for discussion.
3. Results
The demographic and cardiometabolic characteristics of these children (Girls: 56%, mean age: 10.5 years, and mean BMI: 22.4) are shown in Table 1. The distributions and concentrations of the selected 14 targeted OCs obtained from the 25 teeth are summarized in Table 2. The monobutyl ester phthalate metabolites MnBP and MiBP were detected in every tooth, often at high levels. Although quantification was obscured by moderate levels in some blanks, resulting in not reported (NR) values, the insect repellant DEET and the diethylhexyl phthalate metabolite MEHP were detected in nearly every tooth, often at high levels. The diethyl phthalate metabolite MEP was detected at high levels in a few teeth, though quantification was obscured by high levels in all blanks, resulting in many NR values. The secondary oxidative DEHP phthalate metabolites (MECCP, MEOHP, and MEHHP), which are present at higher levels than MEHP in urine, were rarely detected in these teeth, although a clear explanation for this observation is unknown. As reported in Table 2, the specific metabolite TCPy of the organophosphate insecticide chlorpyrifos, the analgesic APAP, the organophosphate flame retardant TBOEP, the specific metabolite IMPy of the organophosphate insecticide diazinon, and monobenzyl phthalate (MBzP) were occasionally detected in these teeth.
For data analysis, the five most frequently detected OCs in the LC/MS/MS analysis of the 25 teeth were considered: the insect repellant DEET; MnBP, MiBP, and MEHP, which are metabolites of phthalates commonly used as plasticizers; and the analgesic APAP. We replaced the non-detected values of APAP with 0.25 ng/g, which is slightly below the lowest detected APAP concentration (0.33 ng/g). The Pearson correlations, significant or suggestive, between the five most frequently detected OCs and obesity/CMTs are reported in Table 3. Of the five OCs considered for the analysis, DEET is not associated with obesity/CMTs. As shown in Table 3, of the three phthalate metabolites considered for the analyses, MiBP positively and significantly correlated with three CMTs: FM (r = 0.496, p = 0.012), FI (r = 0.594, p = 0.002), and HOMA-IR (r = 0.560, p = 0.004). MnBP exhibited significant negative correlations with both blood pressure measures: SBP (r = −0.428, p = 0.033) and DBP (r = −0.537, p = 0.006), while MEHP was found to be negatively and significantly associated with TG (r = −0.485, p = 0.019). Interestingly, APAP showed a negative and significant association with HDL-C (r = −0.518, p = 0.009), and a positive association with TG (r = 0.399) that was suggestive (p = 0.059) in nature. Its positive association with ALT (r = 0.471) was significant (p = 0.020), while its positive association with AST was suggestive (r = 0.376, p = 0.070).
4. Discussion
Environmental influences in early life including the pre-, peri-, and post-natal periods can be detrimental in shaping an individual’s developmental trajectories [69]. This is well understood in the context of obesity and diabetes, where exposures to POPs and OCs during the early stage of life are linked to the burden of adult obesity and related diseases [38]. Measuring low levels of toxic chemicals and exposures during the critical span of prenatal, perinatal, and postnatal growth phases has been an emerging field of research investigations. By exploiting the primary teeth as a biological tool for examining the accumulation of traces of chemicals, we assessed the exposures captured by them during the early developmental stages and analyzed their influence on obesity and CMTs in Mexican American children. The use of exfoliated teeth as a biomarker for past chemical exposure is promising on many counts. First, they are expected to capture early-life chemical exposures in a continuum starting from the second trimester in utero through the stage where primary teeth are shed. Second, they stably store chemicals with decade-long half-lives, unlike such common biological matrices such as urine and blood, which have short half-lives for some chemicals; and, they are non-invasive and easy to collect [57,58,63,70]. Despite their promising nature as a source of biomarkers, primary teeth are relatively understudied biospecimens for organic chemical exposures studies. Our results demonstrated that specific organic compounds can be detected in primary teeth of children. The target analytes included APAP, an active component in many over-the-counter (OTC) and prescription medicines, and metabolites of exogenous chemicals that are ubiquitous in the environment. Monobutyl ester phthalate metabolites MnBP and MiBP, the diethylhexyl phthalate metabolite MEHP, and DEET were detected in every tooth, often at high levels. These are consistent with the previous report from Camann et al. [63]. In this pilot study we found that early-life exposure to phthalate metabolites was associated with several markers of cardiometabolic risk in children. Additionally, we observed an association between APAP and lipids and liver function markers. To our knowledge this study is the first to examine the relationship between early-life exposures measured from primary teeth and several cardiometabolic traits in MA children. In our study, APAP concentration was significantly negatively associated with HDL-C (p = 0.009) and exhibited a suggestive positive correlation with triglycerides (p = 0.059). In spite of its short half-life (2 to 2.5 h), APAP readily accumulates in pediatric patients after repeated therapeutic doses [71,72]. At correct dosage, APAP use is considered safe. However, APAP over-dosage is a leading cause of drug-induced liver injury worldwide [73,74,75]. The current study revealed that APAP was significantly and positively correlated with alanine aminotransferase (ALT) levels (p = 0.020), and that aspartate aminotransferase (AST) exhibited a suggestive positive association with APAP (p = 0.07). Results from murine models and human volunteers have established the hepatotoxicity consequences of APAP overdose due a wide variety of complex and interrelated pathophysiological processes such as mitochondrial oxidative and ER stress, autophagy and inflammation [73,76]. Elevated levels of long-chain acylcarnitines, triglycerides and free fatty acids in the serum of mice and humans due to APAP-induced mitochondrial dysfunction have also been reported [77,78]. HDL-C levels were significantly higher in patients with acute liver failure caused by APAP intoxication [79]. Maternal use of APAP in pregnancy has been associated with autism spectrum disorder [80], poor communication, behavioral problems [81] and asthma in their offspring [82]. Investigations of early-life APAP exposure and obesity-related outcomes in humans are scarce. To date, a few studies have found a relationship between early-life exposure to APAP and obesity. One such study identified activation of cannabinoid receptors by APAP may promote weight gain as reviewed in [83]. Several animal studies have highlighted the important role of cannabinoid receptor activation in the hypothalamus and limbic system in promoting hunger, food intake, and increased body weight [83]. Murphy et al. showed that APAP use in infancy or childhood may be causally related to increased BMI [44]. Sorrow et al. reported a positive association between APAP metabolites at birth and childhood obesity [46].
We found higher MnBP, MiBP, and MEHP concentrations in the SAFARI children’s teeth compared to those detected in a previous study [64], which may be due to the relatively low socioeconomic status of the SAFARI study participants [84]. Of these three most-detected phthalate metabolites in our study, MiBP showed a significant positive correlation with key indicators of obesity and metabolic syndrome, including fat mass (p = 0.012), fasting insulin (p = 0.002), and insulin resistance (HOMA-IR; p = 0.0004). MnBP exhibited strong association with lower diastolic blood pressure (p = 0.006) and to a lesser extent, with lower systolic blood pressure (p = 0.033). Inverse association with triglyceride (0.019) was noted for MEHP.
While exposure studies on phthalate metabolites in adults have established direct associations with adverse health outcomes such as obesity, cardiometabolic traits, and glucose metabolism disorders [52,53,85,86,87,88,89,90,91], childhood and prenatal studies with phthalate exposure are now in focus. Low-molecular-weight metabolites such as MiBP, MnBP and MEP have been associated with childhood obesity [60,92], whereas and high-molecular-weight phthalate metabolites, with adult obesity [60,92,93]. Although, exposure to MiBP has been reported to increase the odds for elevated BMI, waist circumference and percent body fat [94], conflicting findings were reported by [95,96], who noted no significant association between phthalate metabolite and markers of childhood obesity. The multiracial/ethnically diverse study population may be the reason for the reported inconsistency. Consistent with our results, metabolites of DEHP have been associated with an increase in fasting glucose, insulin, and insulin resistance, and reduction in glucose control in adolescents, adults, and elderly adults [86,89,97,98]. Studies assessing early-life phthalate exposures in relation to insulin resistance have also yielded contradictory outcomes; early-life exposure to phthalates associated with increased HOMA-IR was found in one study [99] but not in the other [100]. Consistent with our findings, studies on the impact of phthalate exposure on lipid metabolism have shown an association of MEHP with increased TG levels [99,101]. In addition, the association of early-life exposure to phthalates and changes in blood pressure shows varying outcomes. Several studies have linked MiBP exposure to elevated systolic blood pressure in children [89,102,103]. However, as found in our study, recent evidence indicates modest reductions in systolic and diastolic BP [52,53,104].
Multiple mechanisms may be involved in linking phthalates to increased body weight, adiposity and cardiovascular risk. Phthalates are known to interfere with peroxisome proliferator-activated receptors (PPARs), key regulators of adipogenesis and energy storage [105,106]. Phthalates can modulate adipocyte differentiation and release of leptin by activating PPAR-y [107]. Laboratory studies have found that phthalate metabolites increase cytokine production [108], while biomarkers of phthalate exposure have been associated with increases in serum markers of inflammation and oxidative stress in adults. Recent findings suggest that phthalates may produce increases in low-grade albuminuria in children, a marker of vascular dysfunction associated with chronic kidney and CVD risk [109]. Moreover, epigenetic alterations including DNA-methylation modifications are suggested to be the modifiers of perinatal programming leading to later-life diseases including obesity. Also, several OCs, including phthalates, have been associated with modifications in DNA-methylation and microRNA expression [110]. These studies suggest multiple mechanisms by which phthalates and other OCs may exert their roles as modifiers of prenatal programming and thus lead to future development of obesity.
Given the exploratory nature of this pilot study, there are several inherent limitations that need to be considered. A major limitation is the small sample size used, representing a subset of an existing study. However, the collection of primary teeth at a large scale in a given study population can be challenging. Hence, the findings reported here are limited in generalizability and should be interpreted with caution. In addition, we are not able to establish causal relationships between the examined variables due to the limitations of the cross-sectional study design. Furthermore, as we previously stated [62], the developmental timing of exposure to the OCs measured in this study within the window between mineralization and tooth loss has not been established. This potentially could weaken their correspondence with cardiometabolic risk. Despite these limitations, our findings do offer valuable insights that can be leveraged for future studies. In fact, we plan to conduct validation studies in the near future to increase the reliability and generalizability of our findings. Also, similar studies in ethnically diverse populations would help to assess the applicability of our study findings to a wider population. Nevertheless, our study has some notable strengths. The approach of using primary teeth as a source of biomarkers to assess early-life exposure to organic chemicals is a major strength. The pervasive presence of OCs, POPs, and EDCs, in the primary teeth reflecting study-specific early-life environmental exposures provides a unique opportunity for future in-depth research. Furthermore, this study precisely identified certain chemical exposures significantly associated with cardiometabolic risk in children and adolescents, underscoring the potential long-term health implications of early-life environmental exposures.
5. Conclusions
This is the first study to use primary teeth as a biomarker for pre-, peri-, and post-natal low-level exposure to organic chemicals, to explore their potential role in the occurrence of obesity and associated cardiometabolic risk in Mexican American children and adolescents. Despite the small sample size, our findings suggest that early-life exposure to phthalates may exert adverse effects on children’s heath, increasing the risk of childhood obesity and its comorbid conditions. Additional studies with a larger study population are necessary to confirm these findings, as well as to determine the molecular bases of the associations observed in this study, and to develop effective intervention strategies to reduce exposure to phthalates. Thus, the findings from this study suggest the need for public awareness regarding the ill effects of organic chemicals such as phthalates that are present in commonly used products (e.g., toys, cosmetics, kitchen items, etc.). Such public health efforts are essential to reduce the harmful effects of early-life exposures to organic chemicals that have direct relevance to childhood obesity and its associated cardiometabolic risk [60,111].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arisaka O. Ichikawa G. Koyama S. Sairenchi T. Childhood obesity: Rapid weight gain in early childhood and subsequent cardiometabolic risk Clin. Pediatr. Endocrinol.20202913514210.1297/cpe.29.13533088012 PMC 7534524 · doi ↗ · pubmed ↗
- 2Deboer M.D. Ethnicity, obesity and the metabolic syndrome: Implications on assessing risk and targeting intervention Expert Rev. Endocrinol. Metab.2011627928910.1586/eem.11.1721643518 PMC 3105461 · doi ↗ · pubmed ↗
- 3Li L. Pinot de Moira A. Power C. Predicting cardiovascular disease risk factors in midadulthood from childhood body mass index: Utility of different cutoffs for childhood body mass index Am. J. Clin. Nutr.2011931204121110.3945/ajcn.110.00122221430113 PMC 3308204 · doi ↗ · pubmed ↗
- 4Zhang T. Zhang H. Li Y. Li S. Fernandez C. Bazzano L. He J. Xue F. Chen W. Long-term Impact of Temporal Sequence from Childhood Obesity to Hyperinsulinemia on Adult Metabolic Syndrome and Diabetes: The Bogalusa Heart Study Sci. Rep.201774342210.1038/srep 4342228230104 PMC 5322533 · doi ↗ · pubmed ↗
- 5Horesh A. Tsur A.M. Bardugo A. Twig G. Adolescent and Childhood Obesity and Excess Morbidity and Mortality in Young Adulthood—A Systematic Review Curr. Obes. Rep.20211030131010.1007/s 13679-021-00439-933950400 · doi ↗ · pubmed ↗
- 6Skinner A.C. Perrin E.M. Moss L.A. Skelton J.A. Cardiometabolic Risks and Severity of Obesity in Children and Young Adults N. Engl. J. Med.20153731307131710.1056/NEJ Moa 150282126422721 · doi ↗ · pubmed ↗
- 7NCD Risk Factor Collaboration Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults Lancet 20173902627264210.1016/S 0140-6736(17)32129-329029897 PMC 5735219 · doi ↗ · pubmed ↗
- 8Nyberg S.T. Batty G.D. Pentti J. Virtanen M. Alfredsson L. Fransson E.I. Goldberg M. Heikkila K. Jokela M. Knutsson A. Obesity and loss of disease-free years owing to major non-communicable diseases: A multicohort study Lancet Public Health 20183 e 490e 49710.1016/S 2468-2667(18)30139-730177479 PMC 6178874 · doi ↗ · pubmed ↗