Chemotherapy and Other Systemic Drugs Used to Treat Gynecologic Carcinosarcomas (GCSs): A Retrospective Analysis from Hospital Clínico San Carlos (HCSC), An Academic Referral Centre for Rare Gynecological Malignancies in Madrid, Spain
Gloria Marquina, Beatriz Gonzalez-Diez, Pluvio J. Coronado, Javier Garcia Santos, Mar Ramirez, Monica Bellon, Rafael Sanchez del Hoyo, Alejandro Pascual, Cristina Diaz del Arco, Noelia Sanmamed Salgado, Elena Cerezo, Ramiro Mendez, Miguel Muñoz, Jose Manuel Espejo, Angel Nava

TL;DR
This study analyzed 62 patients with gynecologic carcinosarcomas and found that despite surgery and chemotherapy, outcomes remain poor with high recurrence and short survival times.
Contribution
This is the first real-world evidence on treatment outcomes and disease progression in gynecologic carcinosarcoma patients.
Findings
Median progression-free survival was 5 months with platinum-based chemotherapy.
Median overall survival was 24 months, highlighting the aggressive nature of the disease.
Recurrence rate was 58%, even with multimodal treatment approaches.
Abstract
This retrospective study evaluated 62 patients with gynecologic carcinosarcomas (GCSs) treated at Hospital Clínico San Carlos (Madrid, Spain) between 1995 and 2024. Most patients underwent surgery followed by platinum-based chemotherapy (mainly carboplatin and paclitaxel) and, in some cases, radiotherapy. Despite this multimodal approach, outcomes remained poor, with a high recurrence rate (58%), a median progression-free survival of 5 months, and a median overall survival of 24 months. This study presents the first real-world evidence on the disease control rate, mPFS, and mOS of second and subsequent treatment lines in GCS patients, including information about the treatments administered in each line. These findings confirm the aggressive nature and limited treatment options for GCS, highlighting the urgent need for further research and novel therapies. Background/Objectives:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
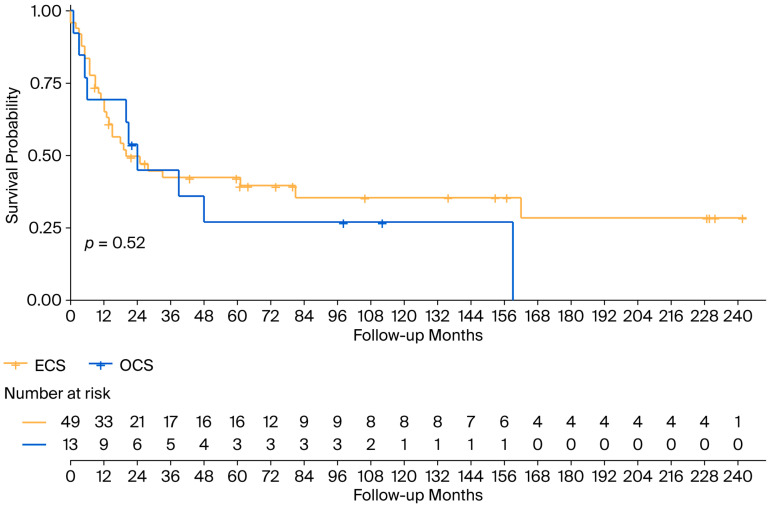 Figure 1
Figure 1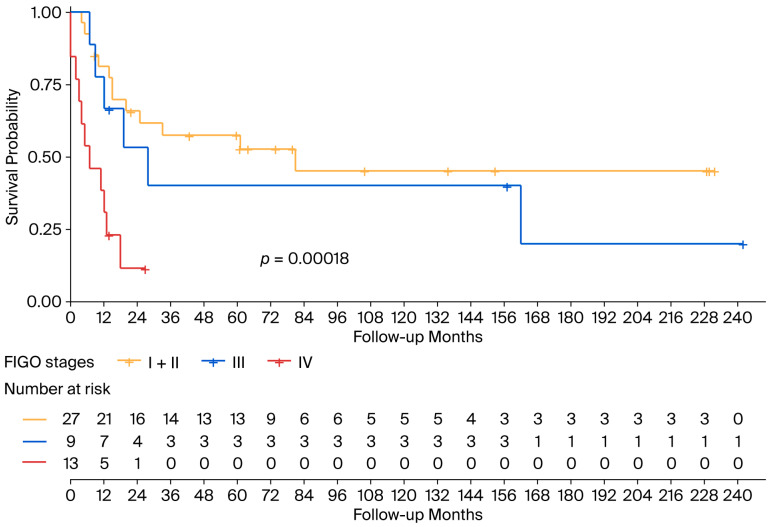 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Breast Lesions and Carcinomas
1. Introduction
Gynecologic carcinosarcomas (GCSs) are rare cancers that were formerly classified and treated as sarcomas. Since the early 2000s, GCSs have been known to be metaplastic carcinomas with molecular features that overlap adenocarcinomas [1], characterized by the presence of both carcinomatous and sarcomatous components. They account for less than 5% of uterine and ovarian malignancies [2,3], with a poor prognosis, with a 5-year overall survival (OS) of less than 30% and median OS (mOS) of less than two years [4].
GCSs mainly arise in the uterus and the ovaries. Ovarian CS (OCS) is currently considered by definition and treated as a high-grade ovarian carcinoma [5], and endometrial CS (ECS) is treated as an aggressive histological type of endometrial carcinoma [6]. In early and locally advanced stages, surgery is the backbone treatment, followed by adjuvant chemotherapy (AdjChT) in OCS patients or chemoradiotherapy in patients with ECS. In metastatic disease, the standard treatment is chemotherapy (ChT), but there is a lower response rate and poorer prognosis compared to those observed for other high-grade carcinomas [7]. A few ECS patients have recently been included in a phase III study in which immunotherapy was added to the standard platinum-based ChT, with promising results [8].
GCS are not usually included or well represented in clinical trials; therefore, real-world information about the use of systemic treatment in this rare disease is key. Thus, we describe our experience treating GCSs at Hospital Clínico San Carlos (HCSC), Madrid (Spain), as part of the European Reference Network on Rare Adult Cancers (EURACAN) referral center for rare gynecological malignancies, and discuss patients’ outcomes in terms of survival.
2. Materials and Methods
Data were collected retrospectively from patients’ physical and electronic medical records from HCSC. The data of consecutive patients with pathologically confirmed GCS were included. Clinical characteristics included age, menopausal status at diagnosis, International Federation of Gynecology and Obstetrics (FIGO) stage 2009 and 2023 for ECS [9,10] and 2014 for OCS [11], Eastern Cooperative Oncology Group (ECOG) performance status, primary tumor (uterine or ovarian), CA125 at diagnosis, ascites at diagnosis, primary treatments (surgery ± adjuvant radiotherapy (AdjRT) ± AdjChT), date of relapse (if any), sites of relapse (pelvic/ lymph nodes/ peritoneal, lung, brain, bone, and other visceral sites), number of lines administered, and the type of ChT administered at every line. ECS stages I and II were analyzed together as FIGO 2023 upstaged stage I ECS to stage II. The year of diagnosis was compiled as <2003 and ≥2003 when systemic treatment shifted from sarcoma to endometrial cancer regimens.
Qualitative variables are presented with their frequency distribution. Quantitative variables are summarized with their median and their range. Survival was studied using descriptive Kaplan–Meier graphs. The log-rank test was used to compare survival curves. A significance value of 5% was accepted for all tests. Data processing and analysis were performed using IBM SPSS Statistics v.26 statistical software and R v.4.5.1 and packages: dplyr (function “%>%” and “filter”); haven (function “read_sav”); survival (function “survfit” and “Surv”); and survminer (function “ggdurvplot”).
Overall survival (OS) was defined as the total length of time from diagnosis until the patient’s death, regardless of the cause of death. Progression-free survival (PFS) was defined as the length of time from the end of a treatment until the first evidence of disease progression or death from any cause. Time to disease relapse was defined as the total length of time (in months) from the end of a treatment until the first evidence of disease relapse. Time to disease progression was defined as the total length of time (in months) from the end of a treatment until the first evidence of disease progression.
3. Results
3.1. Patient Characteristics
Sixty-two GCS patients were treated at HCSC from 1 January 1996 to 31 December 2024, 49 ECS (79%) and 13 OCS (21%). The mean age at diagnosis was 66 (30–90), with most patients being postmenopausal (98%). Abnormal vaginal bleeding was the most commonly presenting symptom, and was reported in 50% of the patients. Information about CA125 was available for 45 patients, and it was found to be abnormal in 28 of them. The median serum CA125 at diagnosis was 48 IU/mL (5–2130 UI/mL); the upper limit in our laboratory is 35 IU/mL The main patient characteristics are summarized in Table 1.
3.2. Multidisciplinary Management as a First Treatment Approach
The information about the multidisciplinary management is summarized in Table 2. Most patients—52 (84%)—underwent surgery at diagnosis with the following FIGO stages: I, 24 patients; II, 6 patients; III, 15 patients; and IV, 7 patients.
AdjRT was administered to 20 ECS patients (32.25%). All these patients received brachytherapy; in addition, 16 patients underwent pelvic radiotherapy (RT) (25.8%) and 1 patient underwent paraaortic RT (2%). None of the OCS patients received AdjRT.
Forty-five patients (62.6%) received perioperative ChT as part of the initial multidisciplinary management. Platinum-based ChT was the AdjChT administered in most of the patients, with carboplatin and paclitaxel being the most frequent combination (administered to 23 patients); other AdjChT regimens involved administration of cisplatin and ifosfamide (6 patients) or carboplatin and epirubicin (2 patients).
After the first treatment approach, 35 patients (56.4%) achieved a complete response, 1 (1.6%) had stable disease, 23 (37%) exhibited objective disease progression and 3 (4.8%) were not evaluated due to death caused by the GCS. More specifically, at the time of data analysis, the statuses of patients treated with neoadjuvant chemotherapy (NACT) or AdjChT (45 patients) were as follows: 16 (35.5%) were alive without disease relapse, 14 (31.1%) experienced a disease relapse, and 15 (33.3%) died.
3.3. Disease Relapse
At a median follow-up (mFollow-up) of 20 months (0–242 months), 36 patients (58%) relapsed or progressed (23 relapses and 13 disease progressions) after the first multidisciplinary management or first-line treatment, respectively. The median time to disease relapse was 6 months (0–225 months) and was slightly different between ECS and OCS: 6 months (0–225 months) vs. 5 months (0–154 months), respectively. The time to disease relapse also differed between FIGO stages: stage I and II: 52 months (0–225 months); stage III: 6 months (0–161 months). As for stage IV GCS, the median time to disease progression was 0 months (0–25 months).
The number of relapses differed between FIGO stages at diagnosis. Table 3 describes the frequency of relapses according to the FIGO 2009 stage at diagnosis and the status of the patients at the time of data analysis.
At the time of relapse/progression, 19 patients (52.7%) were treated with ChT only, 1 patient underwent surgery to treat lung relapse, and 1 patient (2.7%) received palliative RT in response to bone progression. Other treatment approaches at the time of disease relapse/progression were as follows: two patients (5.5%) received ChT and RT, two patients (5.5%) underwent surgery followed by ChT, and two patients (5.5%) received the best supportive care.
The sites of disease relapse were as follows: pelvis (17 patients (47.2%)), peritoneal (13 patients (36.1%)), lymph nodes (6 patients (16.6%)), other visceral locations (5 patients (13.8%)), lung (4 patients (11.1%)), bone (2 patients (5.5%)), and brain (1 patient (2.7)).
3.4. Systemic Treatment in the First and Following Lines
Twenty-six patients (41.9%) were treated in the advanced setting, receiving first-line treatment with a median progression-free survival (mPFS) of 5 months (95% confidence interval 95% (95% CI) 4.2–5.8) and an mOS of 12 months (95% CI 6–18). Twenty patients (76.9%) received a second-line treatment and had mPFS of 2 months (95% CI 0–5). Ten patients (38.4%) received third-line treatment with an mPFS of 2 months (95% CI 1–3). Four lines of treatment were administered in six patients (23%), with an mPFS of 2 months (95% CI 0–4.4). The outcome of each of the treatment lines is shown in Table 4. The ChT regimens used in treatment along with the mPFS achieved are shown in Table 5.
3.5. Overall Survival
With an mFollow-up of 77 months from diagnosis (9–242 months), the mOS was 24 months (95% CI 13.5–34.5): 20 months (95% CI 4–36) in the ECS cohort and 24 months (95% CI 17.4–30.7) in the OCS patients (Figure 1). Regarding survival according to FIGO staging, the mOS among patients with ECS was 81 months in patients in FIGO stage I-II, 28 months (95% CI 7.6–48.4) for patients in stage III, and 7 months (95% CI 0–15.2) for patients in stage IV (Figure 2).
The median survival after GCS relapse/progression was 11 months (1–226 months). It differed between ECS and OCS: 7 months (0–226 months) vs. 11 months (0–36 months). The 3-year overall survival rate was 16.7% in the ECS cohort and 11.1% in the OCS cohort.
At the time of data analysis in December 2024, 20 patients (32.3%) were alive without disease recurrence, 2 patients (3.2%) were alive with disease, and 40 (64.5%) patients were dead.
4. Discussion
In this paper, we show real-world evidence of the initial multidisciplinary management along with a thorough description of the systemic therapies used at relapse and the outcomes of the regimens at each line of a cohort of 62 GCS patients treated at a EURACAN referral center for rare gynecological malignancies. The cohort was enriched with patients from 2003 onwards, with only 10 patients treated before the early 2000s; thus, the treatment of most of the patients is of the current standard.
Fifty-two of the sixty-two GCS patients in our cohort underwent surgery, with twenty of the ECS receiving adjRT and forty-five patients (62.6%) receiving perioperative ChT. This multimodal approach (surgery + adjRT + ChT) is the current standard in locally advanced ECS. Platinum-based ChT was the perioperative ChT regimen administered in most of the patients, with carboplatin and paclitaxel [13,14] being the most frequent combination (23 patients), accounting for a better toxicity profile and non-inferior outcomes than other regimens administered, which were cisplatin and ifosfamide (6 patients) [15] or carboplatin and epirubicin (2 patients). Several studies focusing on newly diagnosed ECS patients also used carboplatin and paclitaxel [16,17]. However, only Hoskins et al.’s publication contains information on the disease relapse rate (33%) [16], which is similar to our study (31%). Two studies mention the different ChT regimens given to GCS patients, but they do not provide any information about the outcomes of the lines or the regimens used [18,19].
In our study, 26 patients were treated [13,14] in the first-line setting. Carboplatin and paclitaxel was the most common ChT regimen used (administered to 12 patients) followed by platinum-based ChT in 9 patients. Years ago, a small number of sarcoma patients were treated with first-line ChT regimens such as doxorubicin and ifosfamide, gemcitabine and adriamycin, gemcitabine and docetaxel, gemcitabine and dacarbazine, or cisplatin and cyclophosphamide. None of the patients were treated with the triplet cisplatin, doxorubicin and ifosfamide, which was tested years ago with a high toxicity profile [20]. Carboplatin and paclitaxel is the current first-line standard combination in GCS due to its better toxicity profile and non-inferiority activity compared to the prior first-line standard, paclitaxel and ifosfamide, as shown in GOG-232B [21] and GOG-261 [22]. Our cohort showed a shorter mPFS and mOS compared to GOG-261 (5 vs. 16 months and 20 vs. 37 months, respectively). A possible explanation for the difference in mPFS is that our cohort included recurrent patients with prior exposure to carboplatin and paclitaxel; as for the difference in mOS, only half of the patients in our cohort (46%) received carboplatin and paclitaxel as a first-line treatment. Notably, our cohort includes patients treated with this combination in subsequent lines—three in the third-line treatment and one in the fifth-line treatment, with an mPFS of 1 month and 5 months, respectively—thus showing activity in further lines. Carboplatin and paclitaxel have shown improved activity in this rare disease in response to the addition of a novel promising drug: dostarlimab [8]. Two patients in our cohort received this triplet treatment, with an mPFS of 17 months. Specific data of only the 25 ECS patients included in the RUBY trial have not been published, but the results for the entire endometrial carcinoma population included showed a 24-month PFS of 56.8% [23]. A patient in our study with recurrent OCS received maintenance niraparib, a poly (ADP-ribose) polymerase (PARP) inhibitor, in line with other high-grade recurrent ovarian cancers.
Reports in the literature on second- and subsequent-line regimens in GCS are scarce. Cisplatin and ifosfamide have been studied in phase II and phase III studies in GCS patients, showing an mPFS between 2 and 4 months in phase II [24] and 6 months in phase III [25]. In our cohort, two patients received this regimen with an mPFS of 5 months, in line with the clinical trial data. Gemcitabine and docetaxel have been tested in a phase II study in second-line recurrent GCS, showing mPFS of 1.8 months [26]. Our data for two patients receiving this regimen are 1 month—in line with phase II—and 226 months—longer than in the phase II study. Another combination used in our patients is carboplatin and pegylated liposomal doxorubicin, which was tested in a phase II study mainly in newly diagnosed GCS patients. Only 1 of the 20 GCS patients had recurrent disease, showing an mPFS of 9.4 months, whereas in our cohort, the 2 patients who underwent second-line treatment and 1 patient who received fourth-line treatment had an mPFS of 5.5 and 4 months, respectively.
Table 6 summarizes the publications on real-world evidence of systemic treatment in GCS to date. There are notably significant differences between any of these published cohorts and ours: fewer patients were included in previously published cohorts [16,19,27,28]; most of these publications do not specify the ChT regimens used not only in the first line but also in subsequent lines; only one publication appropriately describes the outcomes of the first-line therapy [16]; and all but two [19,29] of these studies had a shorter median follow-up than our 29-year cohort.
As far as we are concerned, this is one of the largest GCS studies published in the literature, and it is unique as it includes a long-term follow-up of the patients and specifies the chemotherapy regimens used in each line and the outcomes in terms of survival and response rate, along with the results depending on the FIGO stage and the incorporation of new drugs such as dostarlimab. This publication has limitations, mainly due to the retrospective nature of the data collection and analysis and the treatment variability within patients.
5. Conclusions
To the best of our knowledge, this study presents the first real-world evidence on the disease control rate, mPFS, and mOS of second and subsequent treatment lines in GCS patients, including information about the treatments administered in each line. GCS is a disease for which phase III and real-word data are scarce. In the advanced stages, these patients have a dismal prognosis. Further research is needed to improve the outcomes of GCS patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berton-Rigaud D. Devouassoux-Shisheboran M. Ledermann J.A. Leitao M.M. Powell M.A. Poveda A. Beale P. Glasspool R.M. Creutzberg C.L. Harter P. Gynecologic Cancer Inter Group (GCIG) Consensus Review for Uterine and Ovarian Carcinosarcoma Int. J. Gynecol. Cancer 201424 S 55S 6010.1097/IGC.000000000000022825341582 · doi ↗ · pubmed ↗
- 2Matsuo K. Ross M.S. Machida H. Blake E.A. Roman L.D. Trends of uterine carcinosarcoma in the United States J. Gynecol. Oncol.201829 e 2210.3802/jgo.2018.29.e 2229400015 PMC 5823983 · doi ↗ · pubmed ↗
- 3Rauh-Hain J.A. Diver E.J. Clemmer J.T. Bradford L.S. Clark R.M. Growdon W.B. Goodman A. Boruta D.M. Schorge J.O. del Carmen M.G. Carcinosarcoma of the ovary compared to papillary serous ovarian carcinoma: A SEER analysis Gynecol. Oncol.2013131465110.1016/j.ygyno.2013.07.09723906658 · doi ↗ · pubmed ↗
- 4Garg G. Shah J.P. Kumar S. Bryant C.S. Munkarah A. Morris R.T. Ovarian and uterine carcinosarcomas: A comparative analysis of prognostic variables and survival outcomes Int. J. Gynecol. Cancer 20102088889410.1111/IGC.0b 013e 3181 dc 829220606539 · doi ↗ · pubmed ↗
- 5Ledermann J. Matias-Guiu X. Amant F. Concin N. Davidson B. Fotopoulou C. González-Martin A. Gourley C. Leary A. Lorusso D. ESGO–ESMO–ESP consensus conference recommendations on ovarian cancer: Pathology and molecular biology and early, advanced and recurrent disease Ann. Oncol.20243524826610.1016/j.annonc.2023.11.01538307807 · doi ↗ · pubmed ↗
- 6Oaknin A. Bosse T. Creutzberg C. Giornelli G. Harter P. Joly F. Lorusso D. Marth C. Makker V. Mirza M. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up Ann. Oncol.20223386087710.1016/j.annonc.2022.05.00935690222 · doi ↗ · pubmed ↗
- 7Collet L. González López A.M.G. Romeo C. Méeus P. Chopin N. Rossi L. Rowinski E. Serre A.-A. Rannou C. Buisson A. Gynecological carcinosarcomas: Overview and future perspectives Bull. Cancer 20231101215122610.1016/j.bulcan.2023.07.00537679206 · doi ↗ · pubmed ↗
- 8Mirza M.R. Chase D.M. Slomovitz B.M. de Pont Christensen R. Novák Z. Black D. Gilbert L. Sharma S. Valabrega G. Landrum L.M. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer N. Engl. J. Med.20233882145215810.1056/NEJ Moa 221633436972026 · doi ↗ · pubmed ↗