Finerenone in Patients with Nondiabetic Chronic Kidney Disease—A Retrospective Study
Rehab B. Albakr, Fadel AlRowaie, Ibrahim A. Sandokji, Yazid A. Alhadlg, Khalid Almatham, Abdulaziz B. Albacker

TL;DR
This study found that finerenone reduces albuminuria and blood pressure in patients with nondiabetic chronic kidney disease without causing major side effects.
Contribution
The study provides new evidence on finerenone's efficacy and safety in a diverse ethnic population with nondiabetic CKD.
Findings
Finerenone significantly reduced albuminuria (UACR) in patients with nondiabetic CKD.
No cases of hyperkalemia or hypotension were observed during treatment.
Significant reductions in systolic and diastolic blood pressure were noted.
Abstract
Background & Objectives: Data on the efficacy and adverse effects of finerenone in patients with nondiabetic chronic kidney disease (CKD) are limited, particularly regarding ethnic diversity. This study aimed to evaluate the outcomes of finerenone in patients with nondiabetic CKD previously treated with standard therapies and investigate associated adverse effects, including hyperkalemia and hypotension. Methods: This is a retrospective exploratory study. It is a single-center study including patients with nondiabetic CKD who visited King Fahad Medical City in Riyadh, Saudi Arabia. The primary exposure was finerenone treatment, assessing its effects on albuminuria, kidney function, and blood pressure (BP), following prior use of renin–angiotensin–aldosterone system and sodium–glucose transport protein 2 inhibitors. The measured outcomes were the urine albumin-to-creatinine ratio (UACR)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
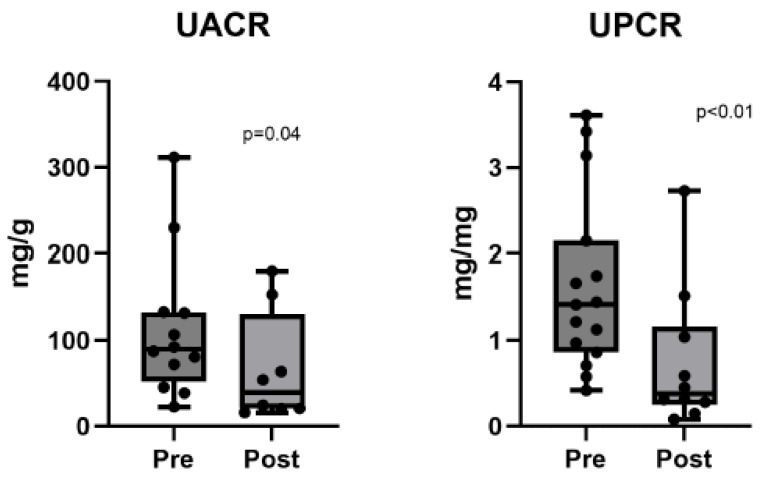 Figure 1
Figure 1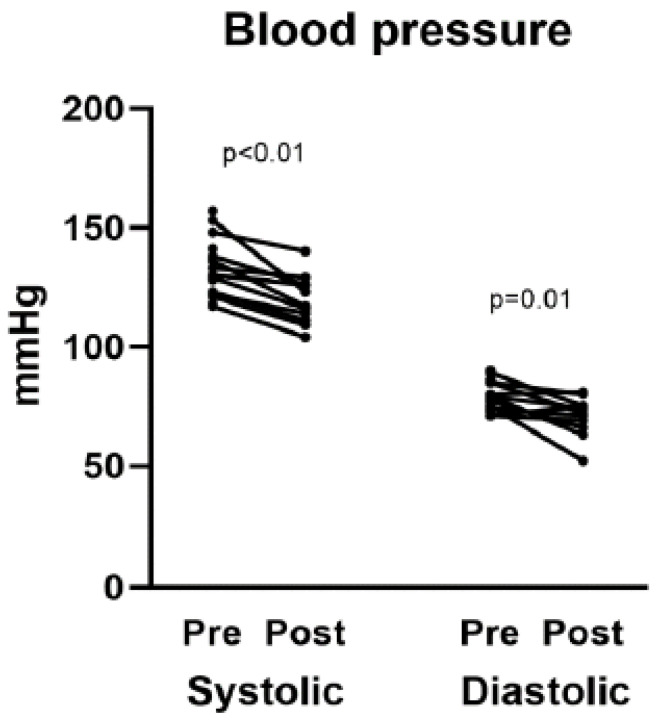 Figure 2
Figure 2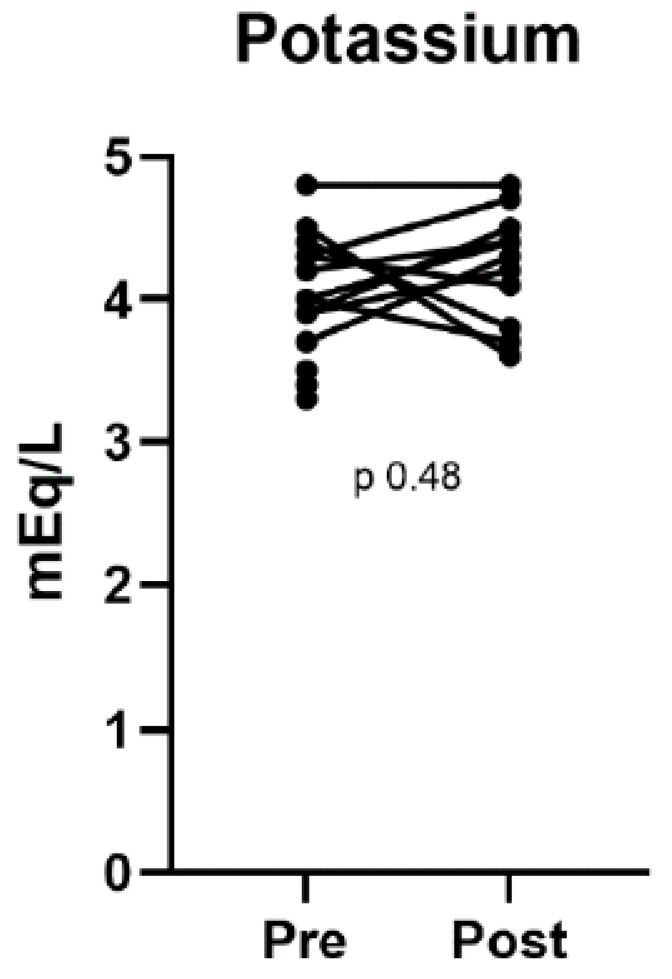 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Diet and metabolism studies · Blood Pressure and Hypertension Studies
1. Introduction
Mineralocorticoid receptor antagonists (MRAs) have shown promise in the treatment of cardiac insufficiency, resistant hypertension, and various kidney disorders. Finerenone, a selective nonsteroidal MRA, exhibits high potency with reduced adverse effects. It has been associated with improved renal and cardiovascular outcomes for high-risk individuals suffering from chronic kidney disease (CKD). By blocking the effects of mineralocorticoids, finerenone decreases the risk of worsening renal function and cardiovascular incidents in patients with CKD linked to type 2 diabetes mellitus (T2DM). However, its effectiveness and safety in individuals with nondiabetic CKD still require comprehensive validation [1,2]. Although there are distinctions between selective and non-selective MRAs, finerenone has demonstrated superior results regarding reductions in albuminuria and BNP levels without causing significant increases in potassium levels [3].
Finerenone is characterized as a nonsteroidal mineralocorticoid that possesses enhanced pharmacokinetic and pharmacodynamic properties. It is favored over earlier medications like spironolactone and eplerenone due to its lower propensity for cardiorenal complications and hyperkalemia [4,5].
A double-blind study involving 5734 patients with CKD and T2DM divided participants into two groups: one receiving a placebo and the other receiving finerenone. Results indicated that finerenone significantly lowers the risk of progression of chronic renal disease as well as cardiovascular issues among these patients [6]. Another randomized controlled double-blind phase II-b trial conducted in Japan compared finerenone to eplerenone, administering either treatment for 90 days. This trial suggested good tolerance for finerenone among Japanese participants; however, due to the limited sample size, further research is necessary to ascertain its efficacy across larger populations [7].
Finerenone holds significant potential to transform therapeutic approaches for individuals with CKD. A recent study involved 20 patients with nondiabetic CKD who were treated with either finerenone or dapagliflozin over four weeks, followed by a combination therapy for another four weeks. The concurrent use of finerenone alongside dapagliflozin exhibited a favorable safety profile along with a notable decrease in albuminuria [8].
Currently, data on the efficacy of finerenone in patients with nondiabetic chronic kidney disease (CKD) are limited. This highlights a significant knowledge gap, as understanding the drug’s effects across diverse populations is crucial for optimizing treatment strategies. Further studies involving multiple ethnicities are essential to confirm finerenone’s efficacy in improving the prognosis of nondiabetic CKD and to identify potential adverse effects associated with its use in different demographic groups.
The Saudi population presents a unique opportunity for this research, as it reflects a distinct ethnic background that contributes to the global diversity of CKD experiences. Investigating the outcomes of finerenone in this cohort is particularly relevant, given the high prevalence of nondiabetic CKD in the region and the potential for genetic, environmental, and lifestyle factors to influence treatment responses.
This exploratory study aimed to evaluate the effectiveness of finerenone in patients with nondiabetic CKD who had previously been treated with standard therapeutic regimens, including renin–angiotensin–aldosterone system (RAAS) inhibitors and sodium–glucose co-transporter 2 (SGLT2) inhibitors, for managing albuminuria and estimated glomerular filtration rate (eGFR). Additionally, we investigated the adverse effects associated with finerenone, such as hyperkalemia and hypotension. The findings from this study will provide valuable insights into the use of finerenone in non diabetic chronic kidney disease and may serve as a starting point for future prospective large studies.
2. Materials and Methods
2.1. Study Design
This was a retrospective, single-center study involving patients who visited the outpatient nephrology clinics of King Fahad Medical City in Riyadh, Saudi Arabia. Only individuals with nondiabetic CKD who are on a maximum tolerated dose of RAAS and SGLT2, or not tolerating any of them, and have residual proteinuria for which they started on finerenone were included in the study, and those with a prior diagnosis of diabetes mellitus were excluded.
2.2. Albuminuria Measurement
Samples were collected during the visit. Two days before these appointments, patients provided one 24 h urine sample and two morning spot urine samples at home. The mean urine albumin-to-creatinine ratio (UACR) derived from the two-morning spot urine samples was used to minimize variability.
2.3. Glomerular Filtration Rate Estimation
The clearance of technetium-99m-DTPA from plasma was used to calculate the measured GFR (mGFR). Four samples were collected from participants with an eGFR of >40 mL/min/1.73 m^2^ at 20 min intervals, 3–4 h after injection. Five samples were collected from participants with an eGFR of ≤40 mL/min/1.73 m^2^ at 30 min intervals, 3–5 h after injection. Blood pressure (BP) was measured while the participants were seated, using a calibrated sphygmomanometer (Microlife WatchBP Office, Microlife AG, Widnau, Switzerland), after a minimum of 5 min repose. Six automated readings were obtained at 1 min intervals, and the average of the five most recent readings was calculated.
2.4. Physical Examination
Each patient underwent a physical examination, during which their weight and height were measured and recorded.
2.5. End Points
The primary outcome measure was the change in UACR among all participants during the 4-week treatment period, along with changes in BP and eGFR. The safety endpoints were adverse events reported by the investigators.
2.6. Statistical Analysis
We summarize and present the characteristics of the study participants, including baseline demographics and clinical and laboratory variables. Categorical variables, such as sex, are presented as percentages, while continuous variables, such as age, are presented as medians with interquartile ranges. The Wilcoxon signed-rank test was used to compare changes in continuous variables, such as BP, before and after therapy initiation. An alpha level of 0.05 was used as the threshold for statistical significance. Data analysis and visualization were performed using Stata version 15.1 and GraphPad Prism version 10.0, respectively.
3. Results
Sixteen patients with nondiabetic CKD were included in this study. The median age was 38.5 years (range, 35–50 years), and 56.3% of the patients were male. The median body mass index was 29.0 kg/m^2^ (27.2–30.0). Table 1 presents the baseline characteristics of the study participants. Among the patients, 50% had IgA nephropathy, 18.8% had focal segmental glomerulosclerosis (FSGS), and 31.3% had other etiologies. The baseline systolic and diastolic BPs were 131.5 mmHg (122.5–139.5) and 79 mmHg (74.5–85), respectively. The baseline estimated eGFR was 66 mL/min/1.73 m^2^ (47–82.5), with a UACR of 90.0 mg/g (58.8–132.5). No hyperkalemia was observed, with a potassium level of 4 mmol/L (3.8–4.4). Table 1 also shows the use of various medications across the sample population. RAAS inhibitors were used by all participants (100%). SGLT2 inhibitors and statins were administered to 93.8% and 81.3% of the patients, respectively. In contrast, diuretics and potassium binders were administered to only 18.8% and 12.5% of the patients, respectively. Among immunosuppressants, mycophenolate mofetil was the most commonly prescribed (37.5%), followed by prednisolone (12.5%) and hydroxychloroquine (6.3%).
Table 2 summarizes the treatment outcomes, including BP, UACR, urine protein-to-creatinine ratio (UPCR), and other laboratory values. Table 3 compares pre- and post-treatment BP and laboratory values, highlighting the statistically significant changes in BP, UACR, and UPCR. Following finerenone treatment, significant reductions in systolic and diastolic BP were observed: 117 mmHg (111–126 mmHg) for systolic BP (p < 0.01) and 72 mmHg (66–75 mmHg) for diastolic BP (p = 0.01). Albuminuria also improved significantly, as indicated by a decrease in the UACR from 90.0 to 39.3 mg/g (p = 0.04). The UPCR also decreased from 1.4 to 0.4 g/g (p < 0.01). Figure 1, Figure 2 and Figure 3 illustrate the differences in UPCR, UACR, and BP pre- and post-treatment, along with changes in potassium levels, demonstrating the overall effectiveness of finerenone in managing albuminuria and BP without significant adverse effects.
No significant changes were observed in the levels of potassium (4 mmol/L vs. 4.4 mmol/L, p = 0.48), albumin (43.5 g/L vs. 41.7 g/L, p = 0.31), or hemoglobin (14.5 g/dL vs. 13.9 g/dL, p = 0.08). Although a slight decline in eGFR from 66 to 58 mL/min/1.73 m^2^ (p < 0.01) was observed, this change was consistent with previous studies in patients with CKD using finerenone.
No adverse events, including hyperkalemia or hypotension, were reported during the treatment period. The results showed that finerenone effectively reduced albuminuria and BP in patients with nondiabetic CKD without causing significant adverse effects.
4. Discussion
Nondiabetic CKD can be classified into several subtypes depending on the underlying pathology. IgA nephropathy is the most prevalent form of nondiabetic CKD, accounting for approximately 52.68% of all cases [9,10]. The deposition of IgA antibodies in glomeruli is a defining characteristic, resulting in inflammation and injury. FSGS was the second most common pathology observed in this cohort. Scarring in particular regions of the renal filtration units is the major characteristic feature of FSGS and a primary contributor to nondiabetic CKD, which may result in progressive renal failure [11,12].
A recent study that identified significant clinical features and outcomes included over 500,000 patients with nondiabetic CKD. Ninety-four percent of patients were diagnosed with stage 3 CKD. The median age of the patients was 75 years, and 60.5% were female [13]. The baseline eGFR was within the range for patients with stage 2 CKD. The UACR is another important marker for assessing renal function and is frequently used to evaluate kidney health. A normal UACR is less than 30 mg/g, while microalbuminuria is indicated by values between 30 and 300 mg/g. Macroalbuminuria is indicated by values exceeding 300 mg/g [14,15]. An elevated UACR in individuals with nondiabetic CKD suggests the progression of renal disease and an increased risk of cardiovascular disease. The UACR in our patients clearly indicated progressive CKD.
RAAS inhibitors are the cornerstone of nondiabetic CKD management. SGLT2 inhibitors, including dapagliflozin and finerenone, have demonstrated substantial nephroprotective benefits in patients with CKD by delaying renal function decline and reducing albuminuria. These medications provide direct renal benefits independent of their impact on blood glucose levels [16,17].
Hyperkalemia, a significant adverse effect linked to finerenone, has been observed more frequently in individuals who were administered the drug during the FIDELIO-DKD clinical trial than in those who were administered a placebo. 21.4% of patients on finerenone developed moderate hyperkalemia, with serum potassium levels above 5.5 mmol/L. This starkly contrasts with 9.2% of the patients who received a placebo. Modest hyperkalemia, defined as serum potassium levels exceeding 6.0 mmol/L, was observed in 4.5% of the finerenone cohort. Conversely, this condition was observed in 1.4% of patients in the placebo cohort [18,19]. The percentage of treatment terminations, which may be attributed to hyperkalemia, was exceedingly low despite the elevated incidence [19]. The rate of finerenone use was only 2.3%, whereas the placebo rate was only 0.9%. In these investigations, no fatalities due to hyperkalemia were observed [19]. However, in the present study, none of the patients reported hyperkalemia. Potassium levels remained within the recommended range during the study period.
Finerenone has been shown to slightly reduce BP. Specifically, the mean systolic BP decreased by 2–4 mm Hg, and the diastolic BP decreased by 1–2 mm Hg during the first month of treatment. These effects persisted over time. A study assessing ambulatory BP found that finerenone significantly reduced 24 h systolic BP. Adjustments indicated that finerenone reduced systolic BP by 8.3 mmHg with a 10 mg dosage and 11.2 mmHg with a 15 mg dosage, compared to placebo [20].
In clinical trials, including FIDELIO-DKD and FIGARO-DKD, hypotension was observed in 4.6% and 3.0% of patients who received finerenone and placebo, respectively. Most hypotensive episodes were classified as mild to moderate and frequently resolved without medication cessation. The rate of hypotension-related hospitalizations was similar between the two groups, with only 0.1% of patients discontinuing finerenone owing to hypotension [20]. Similar to these findings, the blood pressure reduction reported in our cohort (≈14 mmHg systolic) is larger than in previous studies (2–4 mmHg), suggesting that the cohort is not comparable, and this should be discussed as a possible bias.
A recent study found that finerenone substantially reduced the UACR in individuals with diabetic kidney disease, suggesting its potential to lower albuminuria, a critical indicator of renal impairment [21]. A decrease in the UACR may also suggest a reduction in cardiovascular events in nondiabetic individuals and a delay in CKD [21]. Significant UACR improvement was observed in our patients, supporting the benefits of finerenone in nondiabetic CKD.
The median age of 38.5 years in our study population may not be representative of most nondiabetic CKD cohorts, as highlighted by other studies, where the median age is 75 years. This discrepancy should be considered when interpreting our findings [22].
In our cohort, eGFR declined slightly, which aligns with previous findings. The FIDELIO-DKD trial reported an initial median eGFR decrease of 3.3 mL/min/1.73 m^2^ in patients receiving finerenone after 4 months, compared to a drop of 0.8 mL/min/1.73 m^2^ in the placebo group. This initial decline, observed after discontinuation of the drug, was deemed reversible. The decline follows a power function associated with finerenone exposure, suggesting that, despite the initial reduction, long-term effects may stabilize or improve [23,24]. However, given the short duration of our study, it remains challenging to determine whether this decline represents a hemodynamic dip similar to that seen with RAAS inhibitors or a marker of CKD progression.
Nondiabetic chronic kidney disease (CKD) includes various underlying causes, such as glomerulonephritis and hypertension, which can affect treatment responses and outcomes. This study did not stratify results by specific CKD causes, making it difficult to tailor treatments for diverse patient populations.
Additionally, the small sample size (n = 16) and the absence of a comparator group limit the generalizability of the findings. Like many studies examining the effects of this drug on nondiabetic CKD over short follow-up periods, this exploratory study offers limited insights due to its retrospective design, which may introduce information biases and confounding factors. Notably, 90% of the cohort was on SGLT2 inhibitors, which can independently lower albuminuria and blood pressure. Subgroup analyses were not feasible with our current data. Finally, the study’s duration may be insufficient to assess long-term outcomes, such as kidney failure or cardiovascular events, which are essential for understanding the full impact of the treatment.
To conclude, finerenone shows promise in treating CKD, particularly among patients with diabetes. Our findings suggest that finerenone may reduce albuminuria and BP in nondiabetic CKD patients, warranting larger, controlled studies. This exploratory study provides preliminary data on its safety and efficacy in nondiabetic CKD, with no major adverse effects observed in a Saudi population, though initial eGFR decline was consistent with prior studies. Future studies should explore its long-term effects, comparative efficacy with other treatments, and potential benefits of combination therapies in diverse populations and nondiabetic CKD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marcath L.A. Finerenone Clin. Diabetes 20213933133210.2337/cd 21-005034421212 PMC 8329022 · doi ↗ · pubmed ↗
- 2Stompór T. Adamczak M. Kurnatowska I. Naumnik B. Nowicki M. Tylicki L. Winiarska A. Krajewska M. Pharmacological Nephroprotection in Non-Diabetic Chronic Kidney Disease—Clinical Practice Position Statement of the Polish Society of Nephrology J. Clin. Med.202312518410.3390/jcm 1216518437629226 PMC 10455736 · doi ↗ · pubmed ↗
- 3Rico-Mesa J.S. White A. Ahmadian-Tehrani A. Anderson A.S. Mineralocorticoid receptor antagonists: A comprehensive review of finerenone Curr. Cardiol. Rep.20202214010.1007/s 11886-020-01399-732910349 · doi ↗ · pubmed ↗
- 4Kolkhof P. Jaisser F. Kim S.-Y. Filippatos G. Nowack C. Pitt B. Steroidal and novel non-steroidal mineralocorticoid receptor antagonists in heart failure and cardiorenal diseases: Comparison at bench and bedside Heart Fail.201724327130510.1007/164_2016_7627830348 · doi ↗ · pubmed ↗
- 5Marzolla V. Infante M. Armani A. Rizzo M. Caprio M. Efficacy and safety of finerenone for treatment of diabetic kidney disease: Current knowledge and future perspective Expert Opin. Drug Saf.2022211161117010.1080/14740338.2022.213088936174659 · doi ↗ · pubmed ↗
- 6Bakris G.L. Agarwal R. Anker S.D. Pitt B. Ruilope L.M. Rossing P. Kolkhof P. Nowack C. Schloemer P. Joseph A. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes N. Engl. J. Med.20203832219222910.1056/NEJ Moa 202584533264825 · doi ↗ · pubmed ↗
- 7Sato N. Ajioka M. Yamada T. Kato M. Myoishi M. Yamada T. Kim S.-Y. Nowack C. Kolkhof P. Shiga T. A randomized controlled study of finerenone vs. eplerenone in Japanese patients with worsening chronic heart failure and diabetes and/or chronic kidney disease Circ. J.2016801113112210.1253/circj.CJ-16-012227074824 · doi ↗ · pubmed ↗
- 8Mårup F.H. Thomsen M.B. Birn H. Additive effects of dapagliflozin and finerenone on albuminuria in non-diabetic CKD: An open-label randomized clinical trial Clin. Kidney J.202417 sfad 24910.1093/ckj/sfad 24938186886 PMC 10768792 · doi ↗ · pubmed ↗