An Immuno-Fragile Profile Is Associated with Mortality Risk in Patients with Chronic Kidney Disease
Noemí Ceprián, Irene Martínez de Toda, Paula Jara Caro, Claudia Yuste, Gemma Valera-Arévalo, Ignacio González de Pablos, Andrea Figuer, Matilde Alique, Rafael Ramírez, Enrique Morales, Julia Carracedo

TL;DR
This study finds that a combination of immune dysfunction and frailty, called an immuno-fragile profile, is linked to higher mortality in chronic kidney disease patients.
Contribution
The study introduces the concept of an 'immuno-fragile profile' as a novel prognostic tool for CKD mortality.
Findings
CKD patients, especially those on hemodialysis, show reduced lymphocyte counts and increased proinflammatory monocytes.
Frailty is most common in hemodialysis patients and correlates with higher mortality risk.
The immuno-fragile profile independently predicts mortality in CKD patients.
Abstract
Background/Objectives: Patients with chronic kidney disease (CKD) face higher risks of infections, poor vaccine responses, and cardiovascular diseases, leading to increased morbidity and mortality due to immune dysfunction and frailty. This study aims to evaluate immune status and frailty in CKD patients across different treatments, examine the influence of frailty on immune status, and link these factors to mortality. Methods: A total of 174 participants were included (end-stage renal disease, ESRD n = 40; hemodialysis, HD n = 40; peritoneal dialysis, n = 36; kidney transplant patients, n = 40; healthy subjects n = 18). Immunophenotyping of lymphocyte and monocyte subpopulations was performed, and frailty was assessed using the Edmonton Frail Scale. Principal component analysis (PCA) integrated immune and frailty variables to define an “immuno-fragile profile,” and survival was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
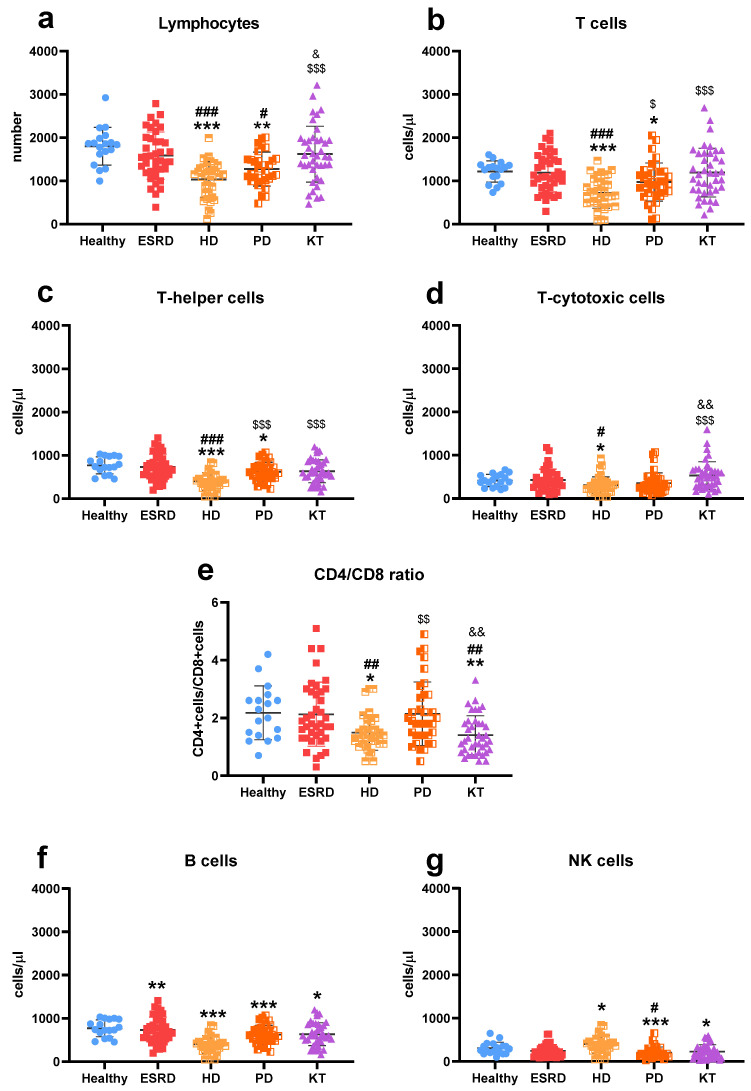 Figure 1
Figure 1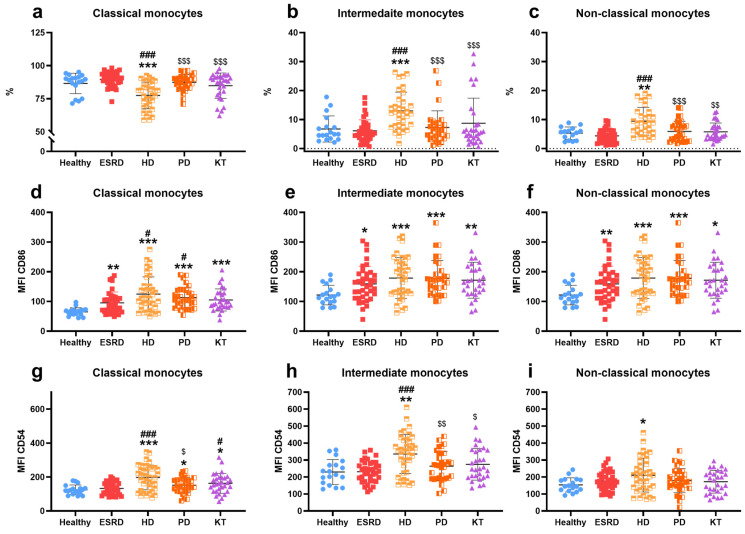 Figure 2
Figure 2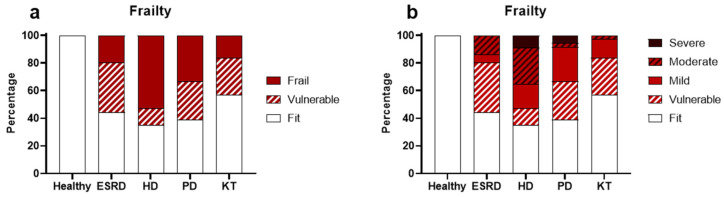 Figure 3
Figure 3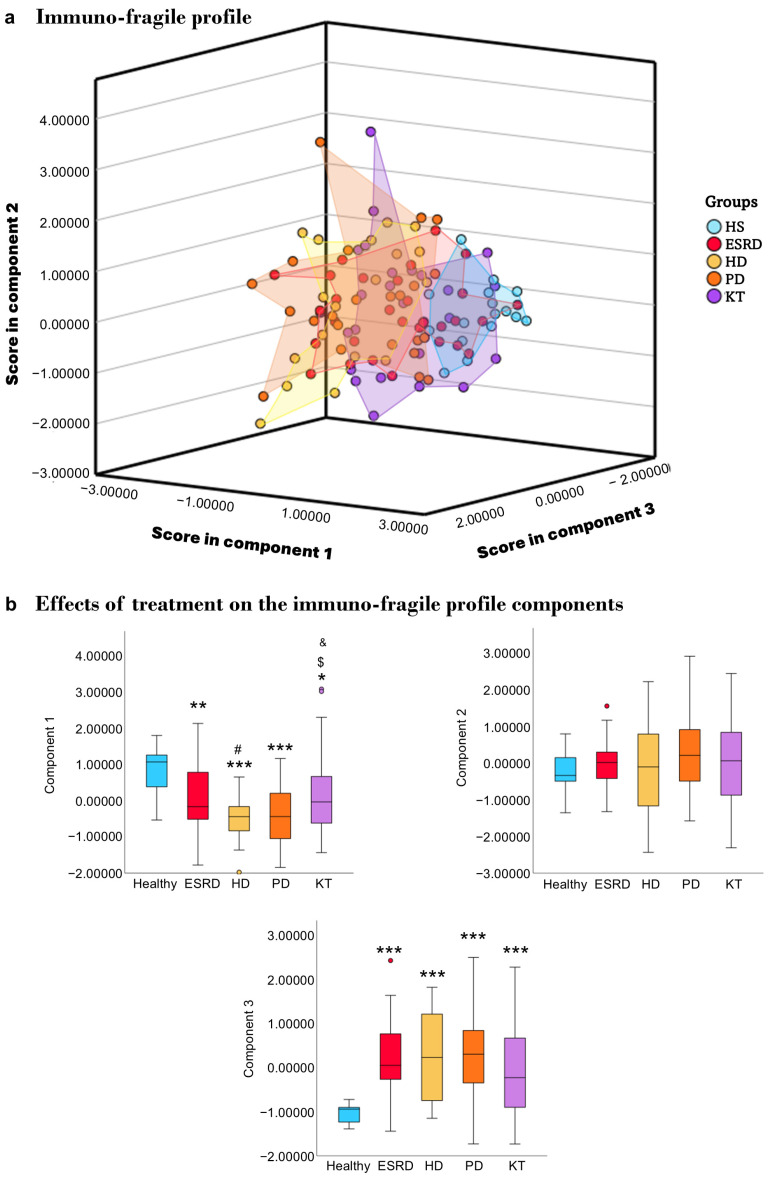 Figure 4
Figure 4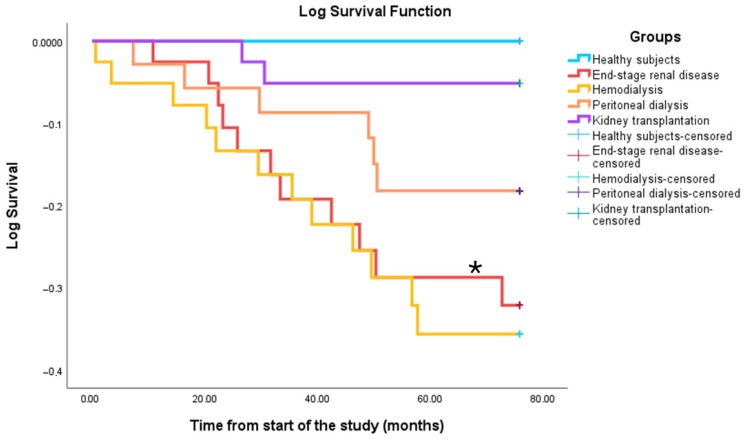 Figure 5
Figure 5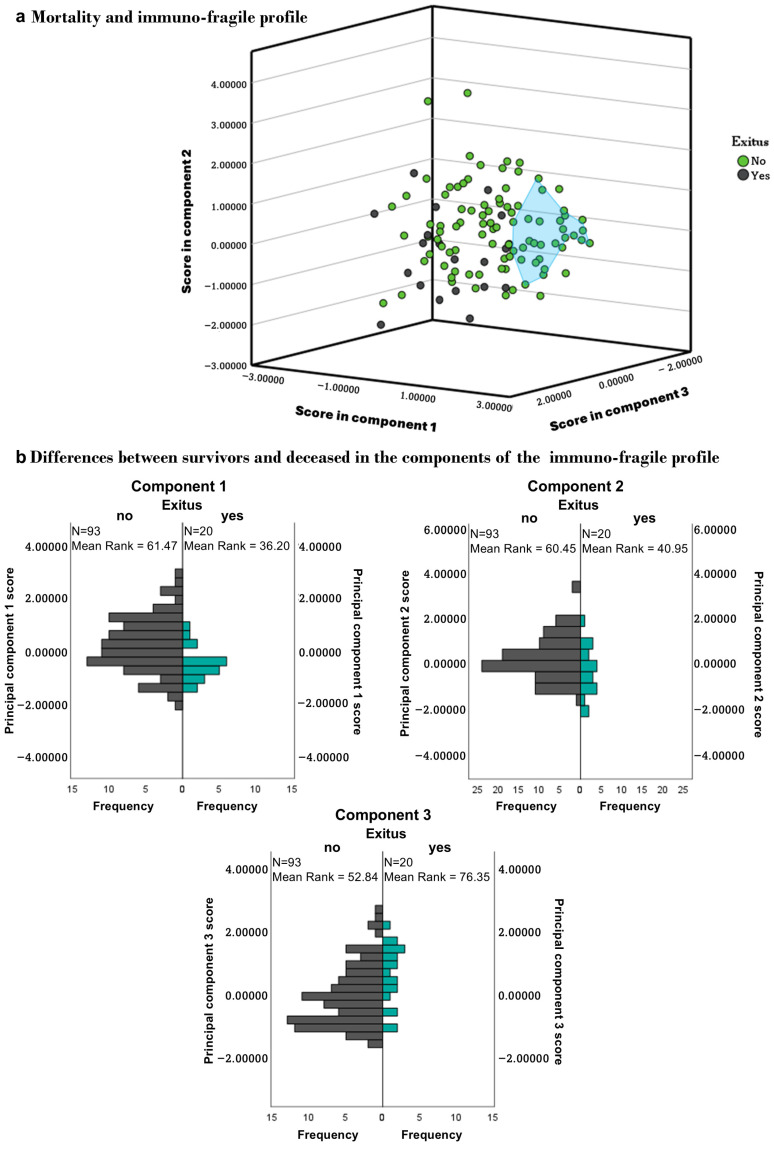 Figure 6
Figure 6- —Instituto de Salud Carlos III
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Adolescent and Pediatric Healthcare · Electrolyte and hormonal disorders
1. Introduction
Chronic kidney disease (CKD) is a significant public health issue and one of the leading causes of death, affecting over 10% of the global population [1,2,3]. Recently, the incidence and prevalence of CKD have risen due to an increase in risk factors such as diabetes mellitus, hypertension, obesity, and aging [4,5,6,7,8].
CKD is considered a disease that occurs with accelerated and premature aging [9,10,11]. Patients with CKD display traits similar to those observed with aging, such as a high rate of cardiovascular disorders, the establishment of low-grade chronic inflammatory stress, immunosenescence, oxidative stress, osteoporosis, and increased frailty, all of which contribute to a shorter life expectancy compared to the general population [7,9,11,12,13].
In this context, the leading causes of death in these patients are cardiovascular disease and increased susceptibility to infections, both of which are closely related to the immune system [8,14,15,16,17]. The fibrosis process in the kidney, along with rising levels of uremic toxins in the blood (notably indoxyl sulfate and p-cresol), leads to immunosenescence, chronic low-grade inflammation or inflammaging, increased oxidative stress, endothelial dysfunction, and disruption of the gut barrier with microbial translocation [14,18,19,20,21]. In turn, this results in lymphopenia, reduced naïve T and B cell populations, an imbalance in the Th1/Th2 ratio, elevated proinflammatory cytokine production, and impaired antigen-specific responses [4,15,18,20,22,23,24,25]. These factors contribute to a higher frequency and severity of infections, decreased vaccine effectiveness, and impaired tumor surveillance [13,24,25,26,27,28].
Furthermore, immunosenescence, inflammaging, and oxidative stress in CKD patients cause endothelial dysfunction and senescence, as well as the expansion of proinflammatory monocyte subsets (intermediate CD14++CD16+ and non-classical CD14+CD16+ monocytes), which exhibit impaired regulation of apoptosis [14,29,30]. Additionally, these monocytes express high levels of adhesion molecules, which promote vascular infiltration and contribute to microinflammation, plaque formation, and endothelial senescence [31,32,33]. All of these factors increase the risk of atherosclerosis and cardiovascular disease in these patients.
CKD patients are especially vulnerable to frailty [34]. Frailty is an age-related condition characterized by decreased homeostatic capacity resulting from declining physiological function and increasing susceptibility to stress, illness, and death [34,35]. Frail individuals may face hospitalization or disability from minor stresses [36]. It is a major predictor of adverse outcomes such as falls, fractures, and reduced quality of life, leading to increased healthcare utilization and polypharmacy [36,37,38]. However, the underlying mechanisms of frailty are still not well understood. Contributing factors may include chronic inflammation, immune activation, anemia, low hematocrit levels, obesity, and other comorbidities [38]. In CKD, research shows that the risk of frailty increases as glomerular filtration rate decreases [39], especially among elderly patients, women, and those with diabetes [40]. Indeed, frailty is an independent risk factor for death or progression to dialysis [34].
Given the significance of immune disorders and frailty on the health and quality of life of CKD patients, this study aimed to assess the immune status in patients with end-stage renal disease, undergoing hemodialysis, peritoneal dialysis, or kidney transplantation, compared to healthy subjects. The relationship between immune status and frailty was also examined across different patient groups.
2. Materials and Methods
2.1. Study Design, Patient Population
This observational study included both cross-sectional and prospective components. It involved a total of 116 CKD participants from three distinct treatment groups: end-stage renal disease (n = 40, ESRD) stage 4–5, hemodialysis (n = 40, HD), and peritoneal dialysis (n = 36, PD). Additionally, 40 participants were undergoing initial kidney transplantation (KT), and 18 healthy subjects (HS) were included. All participants were stable and had been receiving the same treatment for at least six months. Those with neoplasms, infections, or active inflammatory or autoimmune diseases were excluded. The research was conducted at the Nephrology Department of Hospital Universitario “12 de Octubre” in Madrid, Spain, from May 2018 to March 2022. Participants who wished to continue in the study were monitored until September 2024, with the date and cause of death recorded if applicable. At the end of the study, 28 participants were lost due to their decision to leave or change medical centers, including 10 participants with ESRD, 10 with HD, 6 with PD, and 2 with KT. A summary of the experimental design and patients at each stage is presented in Figure S1. All procedures were conducted in accordance with the Declaration of Helsinki, as adopted by the World Medical Association, and the Declaration of Istanbul, endorsed by the Transplantation Society and the International Society of Nephrology. The protocol received approval from the Ethics Committee of Instituto de Investigación Sanitaria Hospital 12 de Octubre (CEIC: 17/407). All patients provided written informed consent.
2.2. Sample Collection and Measurements
Peripheral blood samples were collected from patients and healthy subjects using ethylenediaminetetraacetic acid (EDTA)-coated tubes. Samples were collected during periodic medical reviews and, in the case of hemodialysis patients, prior to initiating hemodialysis. All samples were analyzed within 18 h.
Biochemical and lymphocyte population analyses were performed at the Department of Clinical Analysis and the Department of Immunology at “12 de Octubre” Hospital. Monocyte characterization was conducted at the Department of Genetics, Physiology, and Microbiology at the Complutense University of Madrid, Spain. Lymphocyte and monocyte phenotyping followed established protocols [41]. Total lymphocytes, T cells (CD3+), T-helper cells (CD3+CD4+), T-cytotoxic cells (CD3+CD8+), B cells (CD19+), and NK cells (CD56+) were quantified using a FACSCanto II cytometer (BD Biosciences, San Jose, CA, USA) and FACSDiva software v8 (BD Biosciences). For monocytes, the percentages of classical (CD14++CD16-), intermediate (CD14++CD16+), and non-classical (CD14+CD16+) subtypes were evaluated, along with the expression of co-stimulatory molecules ICAM-1 (CD54+) and B7.2 (CD86+). They were analyzed at the Flow Cytometry and Fluorescence Microscopy Core Facility of the Complutense University of Madrid, using a FACSCalibur cytometer (BD Biosciences) and FlowJosoftware v10 (Tree Star, Ashland, OR, USA).
Patient frailty was evaluated using the Edmonton Frail Scale (EFS) [42], which has been validated in the Spanish language and assesses nine domains: cognition, health status, functional independence, social support, medication use, nutrition, mood, continence, and performance. Patients complete an eleven-question questionnaire, and their frailty level is determined by a score out of 17, with higher scores indicating greater frailty. According to the official EFS website (Edmontonfrailscale.org), categories include Fit (0–3), Vulnerable (4–5), Mildly Frail (6–7), Moderately Frail (8–9), and Severely Frail (≥10).
2.3. Statistical Analysis
Statistical analysis was conducted using SPSS v28.0 (IBM Corp., Armonk, NY, USA). Categorical variables were compared with the chi-squared test. In contrast, continuous variables were analyzed using the Kruskal–Wallis test, with adjusted post hoc pairwise comparisons, and presented as mean ± SD or range. Principal component analysis (PCA) was applied to selected immune parameters and frailty scores, retaining components with eigenvalues greater than 1 and employing varimax rotation. PCA variables were selected beforehand based on clinical or biological relevance in CKD, immunosenescence, and frailty (lymphocyte subsets, monocyte activation markers, and frailty score), as well as empirical contribution in preliminary analyses (retaining indicators that provided non-redundant information). Survival analysis was performed with Kaplan–Meier curves and the log-rank test. A multivariable Cox proportional hazards model was used to examine the relationship between PCA-derived components and mortality, adjusting for conventional prognostic factors (age, sex, diabetes, and baseline cardiovascular disease). Hazard ratios (HR) and p-values were reported, with p ≤ 0.05 considered statistically significant.
3. Results
3.1. Characteristics of Participants
Table 1 summarizes the clinical and demographic characteristics of the patients. Although age, sex, and etiopathology were similar across the groups, patients with end-stage renal disease (ESRD) had a higher average age (61 ± 17 years) than healthy subjects (HS, 51 ± 16 years, p = 0.02). Body mass index (BMI) was higher in ESRD (27.4 ± 5.4) and kidney transplant (KT) patients (27.0 ± 5.2) compared to HS (24.6 ± 3.6, p = 0.04 vs. ESRD), hemodialysis (HD) (24.3 ± 4.0, p = 0.01 vs. ESRD, p = 0.02 vs. KT), and peritoneal dialysis (PD) (24.8 ± 4.1, p = 0.03 vs. ESRD).
Cardiovascular risk factors, including hypertension and dyslipidemia, were consistent across groups: ESRD (90% and 78%), HD (83% and 58%), PD (92% and 61%), and KT (98% and 53%). Notably, diabetes mellitus was more common in ESRD (45%, p = 0.01) and KT (40%, p = 0.03) than in HD (18%).
The biochemical analysis (Table 2) revealed lower serum albumin (ESRD: 4.3 ± 0.4; HD: 4.1 ± 0.4; PD: 3.8 ± 0.5), total proteins (HD: 6.7 ± 0.7; PD: 6.4 ± 1.4), and hemoglobin (ESRD: 11.7 ± 2.2; HD: 12 ± 1.6; PD: 11.7 ± 1.5) levels in chronic kidney disease (CKD) patients compared to HS and KT recipients (p < 0.001). Elevated serum creatinine levels were observed in all CKD patients (ESRD: 4.3 ± 1.2; HD: 7.8 ± 1.9; PD: 7.3 ± 2.5) compared to HS (0.8 ± 0.2, p < 0.001 vs. ESRD, HD, PD; p = 0.04 vs. KT). Uric acid levels were higher in ESRD (6.5 ± 1.9, p = 0.01) and KT (6.9 ± 1.5, p < 0.001) than in HS (5.0 ± 1.2). C-reactive protein levels were also increased in all patient groups (ESRD: 0.5 ± 0.4, p = 0.01; HD: 0.9 ± 2.1, p < 0.001; PD: 0.9 ± 1.9, p = 0.01; KT: 0.5 ± 0.9, p = 0.03) compared to controls (0.3 ± 0.5).
3.2. Immune Cells Characterization
The number of lymphocytes (Figure 1a) in the blood was lower in dialysis patients (HD: 1033 ± 410, PD: 1274 ± 392) compared to HS (1737 ± 345, p < 0.001 and p = 0.01, respectively), ESRD (1585 ± 549, p < 0.001 and p = 0.02, respectively), and KT (1620 ± 647, p < 0.001 and p = 0.01, respectively). T cell levels (Figure 1b; HS: 1218 ± 247, ESRD: 1188 ± 440, HD: 721 ± 351, PD: 975 ± 440, KT: 1195 ± 563), especially T-helper cells (Figure 1c; HS: 770 ± 194, ESRD: 732 ± 296, HD: 398 ± 206, PD: 625 ± 214, KT: 1195 ± 563), were lower in PD than in HS (p = 0.03 and p = 0.05), and in HD compared to other groups (p < 0.001 in all cases minus T-cell levels vs. PD with p = 0.02). HD patients (308 ± 191) had fewer T-cytotoxic cells (Figure 1d) than healthy subjects (417 ± 142, p = 0.02), ESRD (429 ± 251, p = 0.02), and KT patients (531 ± 321, p < 0.001). All these findings resulted in a lower helper/cytotoxic ratio (Figure 1e) in HD (1.5 ± 0.6) and KT (1.5 ± 1.0) compared to HS (2.2 ± 0.9, p = 0.011 and p = 0.01), ESRD (2.1 ± 1.1, p = 0.01 and p = 0.002), and PD (2.1 ± 1.1, p = 0.01 and p = 0.002). The number of B cells (Figure 1f) was decreased in all patients (ESRD: 131 ± 116, p = 0.002; HD: 119 ± 125, p < 0.001; PD: 95 ± 64, p < 0.001; KT: 137 ± 93, p = 0.02) compared to healthy subjects (199 ± 87). Similarly, NK cell counts (Figure 1g; HS: 303 ± 140; HD: 203 ± 129, p = 0.01; PD: 160 ± 80, p < 0.001; KT: 225 ± 161, p = 0.02) were also reduced.
The percentage of classical monocytes (Figure 2a) was reduced in HD (77 ± 10) compared to other groups (HS: 87 ± 8, ESRD: 90 ± 5, PD: 87 ± 6, KT: 85 ± 10, p ≤ 0.001 in all cases). Meanwhile, the percentages of intermediates (Figure 2b) and non-classical monocytes (Figure 2c) increased in HD (13 ± 6 and 9 ± 5, respectively) (HS: 7 ± 5, p < 0.001; 5 ± 2, p = 0.01; ESRD: 6 ± 4, p < 0.001; 4 ± 2, p < 0.001; PD: 7 ± 6, p < 0.001; 6 ± 4, p < 0.001; KT: 9 ± 9, p < 0.001; 6 ± 3, p = 0.003). Additionally, the expression levels of CD86/B7.2 on classical (Figure 2d), intermediate (Figure 2e), and non-classical (Figure 2f) monocytes increased in ESRD (95 ± 36, p = 0.002; 159 ± 59, p = 0.01; 157 ± 51, p = 0.01), HD (125 ± 58, p < 0.001; 179 ± 69, p < 0.001; 181 ± 80, p < 0.001), PD (113 ± 35, p < 0.001; 178 ± 60, p < 0.001; 188 ± 58, p < 0.001), and KT (105 ± 37, p < 0.001; 172 ± 61, p = 0.002; 161 ± 79, p = 0.01) compared to HS (65 ± 13, 122 ± 33, 119 ± 25). Regarding ICAM-1/CD54 expression by monocytes, it was higher in hemodialysis patients (197 ± 73, p < 0.001; 335 ± 114, p < 0.001; 210 ± 99, p = 0.02) across all three monocyte subtypes (Figure 2g–i) versus HS (125 ± 28, 229 ± 74, 153 ± 42). Furthermore, the expression of this molecule was increased in PD (152 ± 45, p = 0.04) and KT (163 ± 59, p = 0.02) in classical monocytes compared to HS. Lastly, the percentage of B7.2/CD86 positive monocytes was higher in patients (Figure S2a–c), and the rate of ICAM-1/CD54 positive monocytes was elevated in HD and KT compared to HS (Figure S2d–f) in classical and intermediate monocyte populations.
3.3. Frailty
The patients’ frailty status, as assessed by the Edmonton Frail Scale (EFS), is shown in Figure 3. A higher proportion of patients exhibited frailty (defined as a score above 6 on the EFS) in the following groups: ESRD at 19% (p < 0.001), PD at 33% (p < 0.001), and KT at 16% (p = 0.004), compared to HS at 0%. Notably, hemodialysis patients had the highest number of patients with frailty, at 53% (p < 0.001, Figure 3a). Additionally, significant sex differences were observed among patients on HD, with 91% of women classified as frail compared to 38% of men (p = 0.012). When frailty was categorized into different levels (Figure 3b), patients on HD showed the highest percentage of severe frailty (a score over 10 on the EFS) at 9%, versus HS (0%, p < 0.001), ESRD (0%, p = 0.02), PD (6%, p = 0.04), and KT (0%, p = 0.01). Due to the small number of patients with severe and moderate frailty in the other groups, further subdivision of frailty levels was not performed for the remaining data analysis.
3.4. Frailty and Immune Cells in CKD Patients
Frailty was associated with distinct immune alterations across CKD treatment groups, as detailed in Supplementary Table S1. In ESRD patients, frail individuals tended to have lower T-helper cell counts (43 ± 8 vs. 49 ± 10; p = 0.08) and higher T-cytotoxic cell counts (31 ± 10 vs. 23 ± 9; p = 0.06) compared to fit patients, although these differences did not reach statistical significance. Conversely, the helper/cytotoxic (CD4/CD8) ratio was significantly lower in frail individuals (1.6 ± 0.7 vs. 2.5 ± 1.2; p = 0.03), indicating an imbalance in T-cell populations.
In the hemodialysis group, vulnerability to frailty was linked to significantly lower NK cell counts (105 ± 56 vs. 234 ± 99 in fit patients, p = 0.03) and a higher percentage of intermediate monocytes (20 ± 1% vs. 13 ± 6%, p = 0.09). Compared to frail patients (185 ± 70 NK cells; 10 ± 4% intermediate monocytes), vulnerable individuals showed intermediate values (p = 0.08 and p = 0.04, respectively). Additionally, frail patients had lower percentages of ICAM-1/CD54^+^ classical and non-classical monocytes (77 ± 10% and 81 ± 14%) compared to fit patients (87 ± 11%, p = 0.05; and 91 ± 8%, p = 0.09). CD54 expression levels were also reduced in frail individuals (classical: 145 ± 56 vs. 210 ± 82, p = 0.09; non-classical: 129 ± 61 vs. 199 ± 71, p = 0.02).
Among patients on peritoneal dialysis, frail individuals had lower T-cell counts compared to fit patients (786 ± 447 vs. 1163 ± 438, p = 0.04). The percentage of ICAM-1/CD54^+^ classical monocytes was also reduced in frail patients (84 ± 8%) compared to fit (91 ± 9%, p = 0.08) and vulnerable individuals (95 ± 7%, p = 0.04). Vulnerable patients exhibited higher frequencies of intermediate CD54^+^ (99 ± 1%) and classical CD86^+^ monocytes (92 ± 10%) than fit (p = 0.09 and p = 0.07, respectively) and frail patients (p = 0.004 and p = 0.06, respectively). Additionally, non-classical monocytes expressing CD86/B7.2 were more common in vulnerable than in fit patients (85 ± 20% vs. 71 ± 23%, p = 0.06), and their expression levels were significantly higher in frail individuals compared to vulnerable ones (209 ± 46 vs. 167 ± 89, p = 0.02).
In kidney transplant recipients, frail patients had higher T-cell (1607 ± 592) and T-cytotoxic cell counts (841 ± 409) compared to both fit (1147 ± 625, p = 0.09; 531 ± 313, p = 0.07) and vulnerable patients (1045 ± 327, p = 0.07; 380 ± 173, p = 0.01). Vulnerable patients showed lower B-cell counts (92 ± 43 vs. 147 ± 104 in fit patients, p = 0.06) and higher NK cell counts (296 ± 184 vs. 187 ± 152, p = 0.09). Finally, classical monocyte ICAM-1/CD54 expression (95 ± 8%) and intermediate monocyte CD86/B7.2 expression (98 ± 3%) were elevated in vulnerable patients compared to fit individuals (89 ± 9%, p = 0.07; and 94 ± 7%, p = 0.03, respectively).
3.5. Immuno-Fragile Profile
After confirming how frailty affects various immune parameters, we performed a principal component analysis (PCA) to identify a combined immuno-fragile profile by integrating key immune markers with frailty scores. The PCA identified three components with eigenvalues greater than 1. Sampling adequacy was considered appropriate (KMO = 0.695), and Bartlett’s test confirmed the data’s suitability for factor analysis (p < 0.001). Overall, these components explained 70% of the total variance, with Component 1 accounting for 38%, Component 2 for 19%, and Component 3 for 13%. As shown in Table 3, Component 1 was mainly characterized by lymphocyte subsets, Component 2 by monocyte subsets, and Component 3 by frailty indicators.
The scores for each patient in each component were recorded, and a graph was created to clearly show the profiles of each patient group studied (Figure 4a). To verify that the patients indeed had distinct profiles, the score differences within each component for each group were analyzed (Figure 4b). Regarding component 1, where lymphocytes are the main participants, we observed that healthy individuals had different scores from patients with ESRD (p = 0.007), HD (p ≤ 0.001), PD (p ≤ 0.001), and KT (p = 0.013). Additionally, HD patients also showed differences in this component compared to ERCA (p = 0.025) and KT (p = 0.015), while DP patients differed from KT (p = 0.043). In component 2, where monocytes are primarily involved, no differences were observed between patients and healthy individuals. Finally, in the third component, where frailty plays a significant role, differences were noted between healthy individuals and patients regardless of treatment (p ≤ 0.001).
3.6. Survival
Between May 2018 and September 2024, 27 patients died: 11 with ESRD (37%), 12 on HD (40%), 2 on PD (7%), and 2 were KT recipients (5%). Survival rates were significantly lower in the HD (p = 0.01) and ESRD groups (p = 0.02) compared to healthy controls (Figure 5). Deceased patients had significantly lower counts of T, CD4, CD8, and B lymphocytes (p < 0.001). Component scores also differed between survivors and non-survivors: Component 1 (p = 0.002), Component 2 (p = 0.02), and Component 3 (p = 0.004) (Figure 6). A history of acute cerebrovascular accident (ACVA) was linked to higher mortality, particularly in HD patients (100% ACVA vs. 26% non-ACVA).
3.7. Validation of the Immunofragile Profile as a Prognostic Marker
To evaluate the prognostic value of the immuno-fragile profile, we conducted a multivariable Cox proportional hazards regression including the three PCA-derived components alongside established prognostic factors (age, sex, diabetes, and baseline cardiovascular disease). The overall model was significant (χ^2^ (7) = 40.0, p < 0.001). Higher scores in Component 1 (lymphocyte subsets) and Component 2 (monocyte subsets) were associated with a lower risk of death (HR = 0.502, 95% CI 0.27–0.93, p = 0.024; HR = 0.456, 95% CI 0.27–0.77, p = 0.004, respectively), whereas Component 3 (frailty indicators) was still associated with a higher risk of death (HR = 1.722, 95% CI 1.08–2.75, p = 0.023). Among the traditional risk factors, baseline cardiovascular disease showed the strongest link to mortality (HR = 13.744, 95% CI 2.56–73.7, p = 0.003). These findings show that the immuno-fragile profile offers prognostic information that is independent of established clinical factors predictors.
4. Discussion
In this cross-sectional study, we examined the phenotypic changes in lymphocytes and monocytes, the frailty levels of patients with chronic kidney disease (CKD), and the impact of varying degrees of frailty on immunity in patients with end-stage renal disease (ESRD), hemodialysis (HD), peritoneal dialysis (PD), and kidney transplantation (KT), compared to healthy individuals. Our findings indicate that patients with advanced CKD have an altered immune response and increased frailty, which correlates with higher mortality rates, especially among those on HD. This leads to distinct immuno-fragile profiles across different treatment modalities, which are important for understanding survival outcomes.
To our knowledge, this is the first study to evaluate CKD patients’ immune profiles and frail status across various therapeutic options within the same population. The immune system is a critical marker of health and longevity [43] and modulates aging. In chronic kidney disease (CKD), immunity plays a key role in the disease’s development and progression, as well as in adverse outcomes and the onset of comorbidities [13,14,15]. The build-up of uremic toxins contributes to immune dysfunction, chronic inflammation, and cellular senescence [44,45,46]. Despite advances in hemodialysis techniques, immune issues continue to persist, leading to increased morbidity and mortality among these patients [47].
Dialysis patients show lower total lymphocyte counts, including T lymphocytes and T-helper cells, with particularly notable reductions in those on hemodialysis. This condition is also associated with decreased T-cytotoxic cell counts and altered helper/cytotoxic ratios. Similar findings have been reported in other studies [48,49]. In ESRD, while some studies document lymphopenia [50], others report no significant differences [41]. In renal transplantation, lymphocyte levels typically remain stable except for changes in the helper/cytotoxic ratio, which aligns with our previous observations [41]. Regarding B cell counts, most studies indicate a decrease in B cells among CKD patients, regardless of treatment [22,51,52], consistent with our current findings. The decline in both lymphocyte types correlates with worsening renal function, loss of naïve T and B lymphocytes, and increased apoptosis caused by uremia [22,49,50,51,52,53]. These changes in lymphocyte profiles are linked to higher infection risk and poorer vaccine responses in CKD patients [16]. Additionally, B-lymphopenia has been associated with higher mortality rates among those on HD [22].
Intermediate and non-classical monocytes exhibit pro-inflammatory and atherogenic characteristics [14,26,54,55] and are found in increased numbers in hemodialysis patients [55,56], consistent with our results. The co-stimulatory molecule B7.2 plays a crucial role in mediating T-cell activation, and our study indicates that B7.2 expression is elevated in all patients examined. The existing literature presents conflicting findings; some studies report no significant changes [57], while others observe either an increase [41] or a decrease [58] in expression. ICAM-1, an adhesion molecule involved in the leukocyte synapse, showed increased expression solely in HD patients, aligning with prior reports [56]. Additionally, elevated B7.2 and ICAM-1 expression in CKD has been documented in intermediate and non-classical monocytes [41,59]. The upregulation of co-stimulatory molecules may reflect compensatory mechanisms in monocytes aimed at facilitating communication and activation of lymphocytes in response to previously noted alterations. Notably, increased ICAM-1 expression has been associated with enhanced activation of cytotoxic T-lymphocytes [60].
Notably, patients undergoing HD showed the highest level of immunosenescence, marked by lymphopenia, a lower CD4/CD8 ratio, and the expansion of pro-inflammatory monocyte subsets. Despite improvements in membrane biocompatibility, HD still exposes circulating cells to oxidative and antigenic stress and activates the complement system as blood flows through the dialyzer. These processes maintain chronic, low-grade inflammation (inflammaging) and accelerate immune aging, leading to a state of persistent immune dysfunction [61,62]. This provides a biological explanation for why patients with HD in our cohort exhibited the most severe immune impairment.
Frailty is a key indicator of biological aging. Several methods exist for assessing it, with the Edmonton Frail Scale validated for use even by non-geriatricians [42,63]. Studies consistently show that frailty increases as chronic kidney disease progresses and is especially common among patients on hemodialysis [64], as seen in our cohort. In this group, changes in bone and mineral metabolism along with muscle mass loss contribute to physical impairment, which is linked to cognitive decline, malnutrition, depression, reduced quality of life, cardiovascular and metabolic issues, and a higher risk of hospitalization, institutionalization, and death [64,65]. Additionally, oxidative and inflammatory stress in CKD has been directly connected to muscle dysfunction and greater frailty [66]. Importantly, our findings showed not only a higher prevalence of frailty in HD patients but also greater severity, with more individuals classified as moderately or severely frail. Recent prospective studies have confirmed that increased frailty severity in HD patients is associated with significantly higher mortality [67,68].
Although some research relates inflammation and oxidative stress, key factors in premature aging and frailty, the impact of frailty on the immune system remains scarce. A connection has been identified between frailty and proinflammatory cytokines, inadequate vaccine responses, and immune system impairments in frail patients [69,70,71,72]. Our study highlights notable variations in immune alterations among frail individuals; T lymphocyte populations and the expression of co-stimulatory molecules ICAM-1 and B7.2 in monocytes are generally compromised. Alterations in lymphocyte populations, particularly reducing T-helper and cytotoxic T cells [73], along with a proinflammatory monocyte phenotype [74], have been associated with frailty. Furthermore, interactions between these cell types are associated with increased osteoclast production, leading to an imbalance in bone metabolism [75]. Both sarcopenia and osteoporosis, closely related conditions, are characteristic of frailty [35,76]. Furthermore, recent studies show a high prevalence of sarcopenia in patients with CKD, especially those on dialysis [77].
Given the notable variability observed within each therapeutic group, we performed a principal component analysis to define an immune-fragile profile. This approach enables clear and straightforward monitoring of differences between the therapeutic groups and the healthy control population. Although external validation is needed, these profiles could aid in identifying patients at higher risk for comorbidities, as suggested for aging [43,78,79]. Some studies propose that immune profiles could serve as potential biomarkers for chronic kidney disease [48,80,81,82]. In this context, HD patients show the most significant variability and differences compared to the healthy population. These patients are not only prone to immunosenescence, inflammaging, and frailty [22,61,67,83,84] but also experience a high prevalence of chronic infectious diseases, cardiovascular problems, and increased mortality rates [85,86].
Our findings show a lower survival rate among patients undergoing hemodialysis (HD), consistent with existing literature. This decreased survival may result from significant immune alterations and increased frailty seen in this patient group [87,88,89]. Notably, patients who died had lymphopenia across all analyzed lymphocyte populations. Additionally, studies suggest a possible link between these immune changes and cardiovascular events [14], with higher mortality observed in patients with ACVA. Furthermore, the predictive ability of the immuno-fragile profile is supported by a Cox proportional hazards regression model, which confirms that the three components from the principal component analysis—lymphocytes, monocytes, and frailty—are independently associated with mortality risk. Higher scores in lymphocyte counts and co-stimulatory molecules in monocytes, which may indicate better immune competence and compensatory immune responses, are linked to lower mortality. In comparison, higher frailty scores correlate with increased risk. These results offer initial validation of the immuno-fragile profile as a potential clinical tool for both prognostic assessment and diagnostic stratification of CKD patients. However, larger and more diverse studies are necessary to confirm these findings, establish their broader applicability, and refine the profile’s definition. If validated, this composite immuno-fragile profile could become a valuable tool for identifying at-risk patients and guiding early, personalized intervention strategies.
5. Conclusions
In conclusion, this study provides strong evidence of premature immunosenescence and increased frailty in patients with chronic kidney disease, especially those on hemodialysis. Combining immune parameters and frailty scores through principal component analysis helped identify an immuno-fragile profile that not only distinguishes patient subgroups but also predicts survival outcomes. The independent association between this profile and mortality, as shown by Cox regression analysis, highlights its potential as both a diagnostic and prognostic tool in clinical practice.
While these findings are promising, they should be approached with caution. The small sample size, single-center design, and lack of internal and external validation of the PCA require further confirmation in larger and more diverse populations. Future research is necessary to confirm the consistency and clinical usefulness of the immuno-fragile profile. If verified, this method could aid in early risk detection and support personalized treatments designed to improve patients’ quality of life and outlook.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Francis A. Harhay M.N. Ong A.C.M. Tummalapalli S.L. Ortiz A. Fogo A.B. Fliser D. Roy-Chaudhury P. Fontana M. Nangaku M. Chronic Kidney Disease and the Global Public Health Agenda: An International Consensus Nat. Rev. Nephrol.20242047348510.1038/s 41581-024-00820-638570631 · doi ↗ · pubmed ↗
- 2Ying M. Shao X. Qin H. Yin P. Lin Y. Wu J. Ren J. Zheng Y. Disease Burden and Epidemiological Trends of Chronic Kidney Disease at the Global, Regional, National Levels from 1990 to 2019 Nephron 202414811312310.1159/00053407137717572 PMC 10860888 · doi ↗ · pubmed ↗
- 3Kovesdy C.P. Epidemiology of Chronic Kidney Disease: An Update 2022 Kidney Int. Suppl. (2011)20221271110.1016/j.kisu.2021.11.00335529086 PMC 9073222 · doi ↗ · pubmed ↗
- 4Tang Y. Jiang J. Zhao Y. Du D. Aging and Chronic Kidney Disease: Epidemiology, Therapy, Management and the Role of Immunity Clin. Kidney J.202417 sfae 23510.1093/ckj/sfae 23540034487 PMC 11873799 · doi ↗ · pubmed ↗
- 5Chesnaye N.C. Ortiz A. Zoccali C. Stel V.S. Jager K.J. The Impact of Population Ageing on the Burden of Chronic Kidney Disease Nat. Rev. Nephrol.20242056958510.1038/s 41581-024-00863-939025992 · doi ↗ · pubmed ↗
- 6He Y. Tang W. Chen J. Tang J. Zheng Y. Wang X. Xing B. Li X. Xu Y. Wang X. Global Burden of Chronic Kidney Disease Due to Hypertension (1990–2021): A Systematic Analysis of Epidemiological Trends, Risk Factors, and Projections to 2036 from the Gbd 2021 Study BMC Nephrol.20252644810.1186/s 12882-025-04386-840783694 PMC 12335775 · doi ↗ · pubmed ↗
- 7Bikbov B. Purcell C.A. Levey A.S. Smith M. Abdoli A. Abebe M. Adebayo O.M. Afarideh M. Agarwal S.K. Agudelo-Botero M. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017 Lancet 202039570973310.1016/S 0140-6736(20)30045-332061315 PMC 7049905 · doi ↗ · pubmed ↗
- 8Lv J.C. Zhang L.X. Prevalence and Disease Burden of Chronic Kidney Disease Adv. Exp. Med. Biol.2019116531510.1007/978-981-13-8871-2_131399958 · doi ↗ · pubmed ↗