Mirikizumab impact on disease clearance in patients with moderately to severely active ulcerative colitis: analysis of a pre-specified LUCENT trial endpoint
Jean-Frederic Colombel, Jianmin Wu, Taku Kobayashi, Baojin Zhu, Jerome Paulissen, Agni Dhanabal, Vipul Jairath, Corey Siegel, Britta Siegmund, Isabel Redondo, Richard Moses, Fernando Magro

TL;DR
Mirikizumab helps patients with ulcerative colitis achieve disease clearance, which is linked to better outcomes and improved quality of life over time.
Contribution
This study shows that early disease clearance with mirikizumab predicts better long-term clinical outcomes in ulcerative colitis.
Findings
51.3% of patients achieved disease clearance by week 104 with mirikizumab.
Early disease clearance at week 12 was associated with better long-term clinical outcomes.
Disease clearance was linked to greater improvements in patient-reported outcomes.
Abstract
Concurrent achievement of symptomatic, endoscopic, and histologic remission, known as disease clearance, has been proposed as a treatment target in ulcerative colitis. Mirikizumab, an anti-interleukin-23p19 antibody, has demonstrated long-term efficacy and safety, as reported in the LUCENT Phase 3 trials (NCT03518086, NCT03524092, and NCT03519945). The current analysis evaluates the impact of mirikizumab on disease clearance and its association with other clinical and patient-reported outcomes (PROs). LUCENT methods have previously been reported. The proportion of patients achieving disease clearance was determined through week (W)104. Association analyses were assessed between disease clearance and PROs (IBDQ, SF-36, WPAI: UC, PGRS, and PGRC), and early disease clearance and subsequent clinical outcomes (clinical, corticosteroid-free, endoscopic, histological, histologic-endoscopic,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
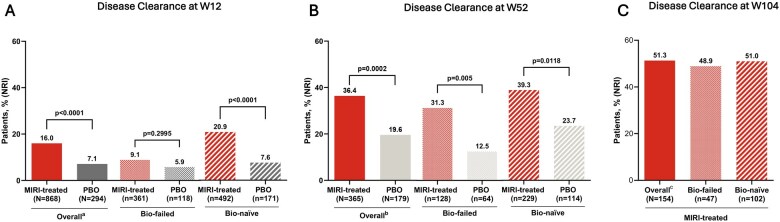 Figure 1
Figure 1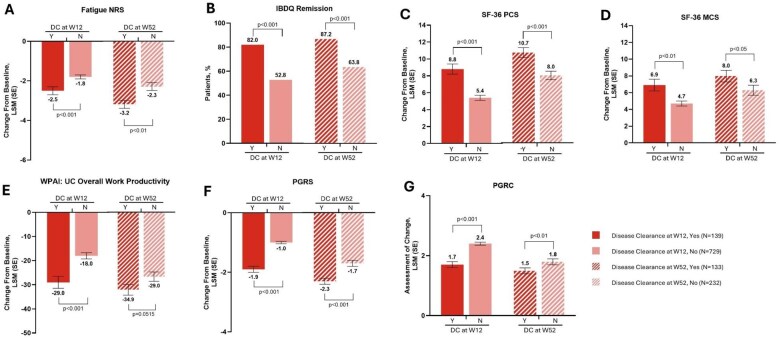 Figure 2
Figure 2| Disease clearance | |
|---|---|
|
| Disease clearance defined as symptomatic remission and HEMR. |
|
| Disease clearance defined as symptomatic remission, HEMR, and fecal calprotectin <250 μg/g. |
|
| |
|
| Modified Mayo score (MMS) Stool Frequency subscore (SF) = 0 or SF = 1 with a ≥ 1-point decrease in MMS SF from baseline; Rectal bleeding (RB) = 0; and MMS endoscopic subscore (ES) = 0 or ES = 1 (excluding friability). |
|
| SF = 0 or SF = 1 with a ≥ 1-point decrease in MMS SF from baseline; RB = 0. |
|
| ES = 0 or 1 (excluding friability). |
|
| Geboes scoring of ≤2B.0 (Geboes subscores of 0 for grades 2 b [lamina propria neutrophils], 3 [neutrophils in epithelium], 4 [crypt destruction], 5 [erosion or ulceration]). |
|
| Week (W)52 (LUCENT-2): W52 clinical remission, W40 symptomatic remission, and no corticosteroid (CS) use ≥12 weeks before W52. W104 (LUCENT-3): W104 clinical remission and no CS use ≥12 weeks before W104. |
|
| Geboes scoring of ≤2B.0 (Geboes subscores of 0 for grades 2 b [lamina propria neutrophils], 3 [neutrophils in epithelium], 4 [crypt destruction], 5 [erosion or ulceration]) and ES = 0 or ES = 1 (excluding friability). |
|
| Urgency numeric rating scale (NRS) score = 0 or 1. |
|
| MMS SF = 0 with a decrease of ≥1-point from induction baseline. |
|
| MMS RB = 0. |
|
| |
|
| 11-point NRS scale (0 = no fatigue to 10 = fatigue as bad as you can imagine; change from baseline). |
|
| 7-point Likert scale (7 = not a problem at all to 1 = a very severe problem, total score ≥170 indicates disease remission). |
|
| Scores of 0–100 (higher scores indicate better health or function). Comprises physical component summary and mental component summary components (change from baseline). |
|
| WPAI: UC scores (absenteeism, presenteeism, work productivity loss in employed patients, and activity impairment in all patients), ranging from 0 to 100 (higher scores indicate greater limitation). |
|
| 1-item patient-rated questionnaire designed to assess patients’ rating of their disease symptom severity over the past 24 hours using a 6-point scale (1 = none to 6 = very severe). |
|
| Patient-rated instrument designed to assess patients’ rating of change in their symptom(s) using a 7-point Likert scale (1 = very much better to 7 = very much worse). |
| Clinical outcome at Week 52 | Achieved DC at Week 12 ( | Did not achieve DC at Week 12 ( |
| Odds Ratio (95% CI) |
|---|---|---|---|---|
|
| 59 (63.4) | 123 (45.2) | <0.01 | 2.1 (1.3, 3.4) |
|
| 55 (59.1) | 109 (40.1) | <0.01 | 2.2 (1.3, 3.5) |
|
| 64 (68.8) | 150 (55.1) | <0.05 | 1.8 (1.1, 3.0) |
|
| 60 (64.5) | 117 (43.0) | <0.001 | 2.4 (1.5 3.9) |
|
| 55 (59.1) | 103 (37.9) | <0.001 | 2.4 (1.5, 3.8) |
|
| 44 (47.3) | 114 (41.9) | 0.365 | 1.2 (0.8, 2.0) |
|
| 79 (84.9) | 195 (71.7) | <0.05 | 2.2 (1.2, 4.2) |
|
| 83 (89.2) | 208 (76.5) | <0.01 | 2.6 (1.3, 5.2) |
|
| 74 (79.6) | 190 (69.9) | 0.071 | 1.7 (1.0, 3.0) |
|
| 76 (81.7) | 213 (78.3) | 0.485 | 1.2 (0.7, 2.3) |
| Clinical outcome at Week 104 | Achieved DC at Week 52 ( | Did not achieve DC at Week 52 ( |
| Odds Ratio (95% CI) |
|---|---|---|---|---|
|
| 73 (65.8) | 56 (43.8) | <0.001 | 2.5 (1.5, 4.2) |
|
| 71 (64.0) | 55 (43.0) | <0.01 | 2.4 (1.4, 4.0) |
|
| 87 (78.4) | 69 (53.9) | <0.001 | 3.1 (1.8, 5.5) |
|
| 71 (64.0) | 53 (41.4) | <0.001 | 2.5 (1.5, 4.2) |
|
| 68 (61.3) | 46 (35.9) | <0.001 | 2.8 (1.7, 4.8) |
|
| 58 (52.3) | 62 (48.4) | 0.557 | 1.2 (0.7, 1.9) |
|
| 82 (73.9) | 87 (68.0) | 0.318 | 1.3 (0.8, 2.3) |
|
| 85 (76.6) | 88 (68.8) | 0.178 | 1.5 (0.8, 2.6) |
|
| 91 (82.0) | 96 (75.0) | 0.193 | 1.5 (0.8, 2.8) |
|
| 90 (81.1) | 104 (81.3) | 0.974 | 1.0 (0.5, 1.9) |
- —Eli Lilly and Company10.13039/100004312
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Celiac Disease Research and Management · Immunodeficiency and Autoimmune Disorders
1. Introduction
In the search for optimal therapeutic strategies for ulcerative colitis (UC), disease clearance (DC)—the concurrent achievement of symptomatic, endoscopic, and histologic remission—has been proposed as an aspirational target, a shift from traditional treatment goals.1–3 In the past, the primary focus of UC management has been symptom relief, sometimes neglecting gut healing and complete remission. This limitation has hindered long-term disease control and outcomes.
The specific benefits of achieving DC in the treatment of UC could include improved disease course, better long-term outcomes, enhanced quality of life (QoL), and predictive value regarding the efficacy of treatment(s).1 Patients with DC have a lower risk of disease recurrence, hospitalization, and surgery, leading to better overall control of UC and improved QoL.4 Additionally, histologic remission, a component of DC, is predictive of sustained clinical remission and lower relapse rates.5 Thus, achieving DC may improve the management and prognosis of UC. Additionally, data from an Australian multicenter retrospective study indicated that 61% of patients achieved clinical remission, of whom 57% also showed endoscopic remission. In total, 35% of these patients showed combined clinical and endoscopic remission, and 16% had combined clinical, endoscopic, and histologic remission.6 Together these results demonstrate that DC in UC is an achievable goal.
The introduction of mirikizumab, a novel anti-interleukin-23p19 monoclonal antibody, has marked an advancement in the treatment landscape of UC. Empirical evidence from the LUCENT Phase 3 trials underscores the robust efficacy of mirikizumab, as evidenced by its impact on individual and composite clinical endpoints.7–9 However, traditional endpoints may not fully encapsulate the comprehensive benefits of achieving DC.
This analysis examines the effects of mirikizumab on achieving DC across 2 years within the LUCENT trials. It also investigates the association between DC and a range of clinical and patient-reported outcomes (PROs), offering a more detailed understanding of the drug’s impact on DC and its associated effect on other clinical outcomes.
2. Methods
2.1. LUCENT-1, -2, and -3 study overviews
The LUCENT-1, LUCENT-2, and LUCENT-3 study designs have been reported previously.7^,^9 These studies comprised 2 sequential, parallel-group, double-blind, randomized, placebo (PBO)-controlled trials, followed by an open-label long-term extension in adult patients with moderately to severely active UC who had an inadequate response or loss of response to, or were unable to, tolerate at least 1 of the following: corticosteroids, 6-mercaptopurine, azathioprine, biologic therapy (tumor necrosis factor inhibitors or vedolizumab), or tofacitinib. LUCENT-1 was a 12-week induction study, followed by the 40-week LUCENT-2 randomized withdrawal maintenance study in patients who responded to mirikizumab induction therapy in LUCENT-1. LUCENT-3 included patients from the phase 3 maintenance study LUCENT-2 who completed the Week (W)52 (W40 LUCENT-2) visit on blinded subcutaneous therapy and, per investigator opinion, would benefit from continuing treatment with mirikizumab in LUCENT-3 (Figure S1).
The studies were conducted in compliance with the consensus ethics principles derived from international ethics guidelines, including the Declaration of Helsinki, the International Council for Harmonisation, and applicable laws and regulations. All patients provided written informed consent before participating in the study. An independent data monitoring committee monitored LUCENT-1, LUCENT-2, and LUCENT-3. The trials were registered at Clinical Trials.gov: NCT03518086, NCT03524092, and NCT03519945, respectively.
2.2. Study assessments
The primary and major secondary endpoints for LUCENT-1 and LUCENT-2 have been previously reported.7^,^ 10 The baseline data for the current analyses were the induction baseline data from LUCENT-1. The endpoint of DC and related analyses were pre-specified in the LUCENT trial Statistical Analysis Plan. The definition of DC and other endpoints associated with the current analyses can be found in Table 1. It is important to note that the Patient Global Rating of Change (PGRC) ranges from 1 to 7, where 1 equals “very much better” (symptoms) and 7 equals “very much worse”; thus, a lower PGRC reflects symptom improvement.11 Patient Global Rating of Severity (PGRS) assesses disease symptom severity of patients over the past 24 hours using a 6-point scale where 1 equals “none” (symptoms) to 6 equals “very severe symptoms”. DC achievement was further evaluated based on the concurrent achievement of symptomatic remission, histologic-endoscopic mucosal remission (HEMR), and fecal calprotectin (fCal) <250 μg/g (alternative DC [aDC]).
2.3. Statistical analyses
The assessment of DC among patients was conducted at W12, W52, and W104. The modified intent-to-treat population, including all patients who received any study treatment during this study and excluding patients impacted by an electronic clinical outcome assessment transcription error in Poland (*n *= 112) and Turkey (*n *= 6) (see D’Haens et al., 2023 Supplementary Appendix for details7), regardless of whether the patient received the correct treatment or did not otherwise follow the protocol, was used to perform efficacy analyses at the indicated time points. Subgroup analyses were conducted based on the following subgroups: patients with no prior biologic or tofacitinib treatment exposure (bio-naïve) and patients with prior biologic or tofacitinib treatment failure (bio-failed). Prior biologic or tofacitinib treatment failure was defined as discontinuation of prior treatment due to loss of response, inadequate response, or intolerance to the therapy.
In the modified intent-to-treat population, treatment comparisons for binary outcomes involved a Cochran–Mantel–Haenszel (CMH) test adjusted for randomization factors (prior biologic or tofacitinib failure [yes/no], baseline corticosteroid use [yes/no], baseline disease activity assessed by the modified Mayo score [MMS, 4–6 or 7–9], and region [North America/Europe/Other]) for LUCENT-1. For LUCENT-2, the adjustment included all the above factors except the modified Mayo score, and additionally included clinical remission status at LUCENT-1 W12 (yes/no).
The associations between PROs and DC were evaluated for patients treated with mirikizumab at W12 and W52, respectively. A CMH test was also used to assess associations between DC and binary outcomes, while analysis of covariance with modified baseline observation carried forward was used to assess the association of DC with continuous outcomes. The associations between DC at W12 and baseline factors, and between DC at W52 and baseline factors, were evaluated using univariable and multivariable logistic regression analyses. Variables with P <.05 in the univariable models were included in the multivariable analyses. Moreover, the association between early achievement of DC and subsequent long-term clinical outcomes was evaluated in mirikizumab-treated patients. Specifically, DC at W12 was assessed for its relationship with clinical outcomes at W52, and DC at W52 with outcomes at W104. Pearson’s chi-square test was used to evaluate these associations, with odds ratios and 95% confidence intervals provided to quantify the strength of the relationships.
Nonresponder imputation (NRI) was used for all binary outcome analyses, including DC (yes/no). Observed Case (OC) analysis was also performed in some supplemental results at W104 to assess the proportion of mirikizumab-treated patients achieving DC among W52 clinical responders. The methods have been described previously in OC analyses, patients with missing data were excluded, and no imputation was applied.
3. Results
3.1. Achievement of DC during induction, maintenance, and long-term treatment
In the modified intent-to-treat population, a significantly greater proportion of mirikizumab-treated patients achieved DC versus placebo at W12 (16.0% vs 7.1%; P <.0001; Figure 1A). At W52, 36.4% of patients treated with mirikizumab achieved DC versus 19.6% with placebo (P <.001). Overall, a higher proportion of patients treated with mirikizumab achieved DC compared to those receiving placebo, in both the bio-naïve and bio-failed subgroups at Weeks 12 and 52. Notably, in the bio-failed subgroup at W52, 31.3% of patients receiving mirikizumab achieved DC versus 12.5% in the placebo group. Similarly, in the bio-naïve subgroup, 39.3% of patients on mirikizumab achieved DC compared to 23.7% with placebo (Figure 1B). About 51.3% of patients on mirikizumab achieved DC at W104 among those who achieved clinical remission at W52, and the rates of patients achieving DC were similar to those of the overall population in both the bio-failed (48.9%) and bio-naïve (51.0%) subgroups (Figure 1C). Results were similar when assessing patients with a baseline modified Mayo Score (mMS) of 5–9 (excluding patients with baseline mMS of 4) per updated FDA guidelines (Figure S2).12 DC achievement in the long-term study was also explored in patients who achieved clinical response on mirikizumab (W52 clinical responders). About 40.6% of the W52 clinical responders achieved DC at W104 (Figure S3). Among patients who achieved DC at W12 with mirikizumab induction, completed LUCENT-2 on mirikizumab 200 mg Q4W subcutaneous and enrolled in LUCENT-3 (*N *= 69, NRI), 52.2% achieved clinical remission, 50.7% achieved CSF remission, 52.2% achieved HEMR, and 75.4% achieved IBDQ remission at W104.
(A) The proportion of patients achieving DC at W12 in LUCENT-1. (B) The proportion of patients achieving DC at W40 in LUCENT-2 (52-week treatment in total). (C) Proportion of patients achieving DC at W104 among patients who achieved clinical remission at W52 and subsequently entered the LUCENT-3. a5 patients receiving PBO and 15 patients receiving MIRI were previously exposed to but had no biologic or JAK inhibitor failure and were excluded from the biologic subgroup analysis. b1 patient receiving PBO and 8 patients receiving MIRI were previously exposed to but had no biologic or JAK inhibitor failure and were excluded from biologic subgroup analysis. c5 patients were previously exposed to but had no biologic or JAK inhibitor failure and were excluded from the biologic subgroup analysis. DC = symptomatic remission + histologic-endoscopic mucosal remission. DC, disease clearance; JAK, Janus kinase; MIRI, mirikizumab; NRI, nonresponder imputation; PBO, placebo; W, Week.
When including assessment of fecal calprotectin in the composite DC endpoint, alternative DC (aDC), a higher proportion of mirikizumab-treated patients achieved aDC at W12 (13.1% vs 4.4%; P <.0001) and W52 (31.0% vs 16.8%; P = .0013; Figure S4). This effect was significant in the bio-naïve subgroup at both timepoints, and in the bio-failed subgroup at W52. In addition, a significantly higher proportion of patients in the bio-naïve subgroup on mirikizumab achieved aDC at both timepoints.
3.2. Association between DC achievement and PROs
The change in Fatigue numeric rating scale (NRS) score, Work Productivity and Activity Impairment Questionnaire: Ulcerative Colitis (WPAI: UC), Overall Work Productivity, Patient Global Rating of Severity (PGRS), and PGRC from baseline and achievement of PROs (Inflammatory Bowel Disease Questionnaire [IBDQ] Remission, 36-Item Short Form Survey [SF-36] physical component summary, and SF-36 mental component summary) at W12 and W52 were compared based on achievement of DC (yes vs no) with mirikizumab at W12 and W52, respectively (Figure 2). Patients who achieved DC at W12 had significantly higher rates of achievement of PROs and larger improvements from baseline of PROs versus patients who did not achieve DC (all P <.01). The trend continued among patients who achieved DC at W52 versus those who did not, but this trend was not seen for WPAI: UC Overall Work Productivity (P = .0515). While not statistically significant, there was a larger improvement in WPAI: UC Overall Work Productivity at W52 among those who achieved DC at W52 than among those who did not (change from baseline of −34.9 vs −29.0).
Association between achievement of DC and patient-reported outcomes in mirikizumab-treated patients; fatigue NRS (a), IBDQ remission (B), SF-36 PCS (C), SF-36 MCS (D), WPAI: UC overall work productivity (E), PGRS (F), and PGRC (G) at W12 and W52. DC, disease clearance; IBDQ, inflammatory bowel disease questionnaire; LSM, least-squares mean; MCS, mental component summary; N, no; NRS, numeric rating scale; PCS, physical component summary; PGRC, patient global rating of change; PGRS, patient global rating of severity; SF-36, 36-item short form health survey; UC, ulcerative colitis; WPAI, work productivity and activity impairment questionnaire.
3.3. Association of early achievement of DC and subsequent achievement of long-term positive clinical outcomes
Achievement of DC at W12 was significantly associated with achievement of clinical remission, corticosteroid (CS)-free remission, endoscopic remission, HEMR, stool frequency (SF) remission, and rectal bleeding (RB) remission at W52 (P <.05; Table 2). Notably, achievement of DC at W12 was not associated with bowel urgency (BU) remission, IBDQ response, and IBDQ remission at W52. The trend continued where the achievement of DC at W52 was associated with the achievement of the same positive clinical outcomes, including CS-free remission, at W104 (P <.05; Table 3), except for SF and RB remission at W104 which were not significantly associated with DC at W52.
3.4. Univariable and multivariable prognostic analyses of association between baseline demographics and characteristics, and DC
Baseline age, body mass index, disease duration, MMS, and prior UC therapies were similar between patients who achieved DC at W12 and those who did not (Table S1).
Associations between demographic and disease characteristics at induction baseline and DC at W12 were analyzed in patients randomized to mirikizumab 300 mg IV in LUCENT-1. Characteristics including left-sided colitis/proctitis, fCal ≤250 μg/g, C-reactive protein [CRP] ≤6 mg/L, baseline MMS, endoscopic subscore (ES) = 2, SF subscore <3, and no prior biologic or tofacitinib failure were significantly associated with DC at W12 in the univariable analysis (Table S2). In the multivariable model, CRP ≤6 mg/L, baseline MMS, ES = 2, SF subscore <3, and no prior biologic or tofacitinib failure were significantly positively associated with DC at W12 (Table S3). Univariable analysis showed that only baseline disease location was significantly associated with DC at W52 (P = .017). Since multivariable analysis selects significant variables from the univariable model and only 1 variable is significant for W52, no multivariable analyses for W52 were assessed (data not shown).
4. Discussion
This analysis demonstrates achievement of DC with mirikizumab treatment in the LUCENT trials based on stringent definitions of DC that include the concurrent achievement of symptomatic remission (SF = 0 or SF = 1 with a ≥ 1-point decrease in MMS SF from baseline; RB = 0), endoscopic remission (ES = 0 or ES = 1, excluding friability), and histologic remission (Geboes scoring of ≤2B.0 [Geboes subscores of 0 for grades 2 b (lamina propria neutrophils), 3 (neutrophils in epithelium), 4 (crypt destruction), 5 (erosion or ulceration)]). The impact of mirikizumab on DC remained consistent despite using the alternative DC which is stringently defined by including biomarker fCal normalization and DC.
Our results suggest that DC was successfully achieved with mirikizumab treatment in up to 16% of patients at W12 and 36% of patients at W52. The consistent achievement of DC across various study stages—induction, maintenance, and open-label extension—indicates the drug’s sustained efficacy. Additionally, achievement of this outcome irrespective of prior biologic treatment implies the potential effectiveness of mirikizumab in patients regardless of treatment experience as both bio-failed and bio-naïve treated patients showed a significant response compared to those with placebo at W52. Patients who achieved DC at W12 showed a higher likelihood of achieving other clinical outcomes at W52. Likewise, achievement of DC at W52 demonstrated an association with achievement of other clinical outcomes at W104.
In this analysis of LUCENT-1 data, the univariable analysis identified left-sided colitis/proctitis, lower fCal level, lower CRP level, baseline MMS, lower ES, lower SF subscore, and no prior biologic or tofacitinib failure as candidate prognostic factors for patients achieving DC at W12. Interestingly, in the LUCENT-2 study only baseline disease location was significantly associated with DC status at W52. This may be attributed to the randomized withdrawal design, in which only mirikizumab responders entered the LUCENT-2 trial. Additionally, while this study, and others, demonstrated that histologic remission was associated with positive clinical outcomes, other studies have not found the same relationship.13 The reason for this discrepancy remains unclear, however, it may result from factors such as the retrospective nature of the study design, variability in histologic scoring reproducibility, differences in patient population or disease states, and the timing of treatment and/or disease longevity. Future work will be needed to clearly dissect the role that endoscopic and histologic remission plays in the resolution of UC.
From multivariable analysis, lower CRP level, baseline MMS, lower ES, lower SF subscore, and no prior biologic or tofacitinib failure were significant prognostic factors for achieving DC at W12 among patients receiving mirikizumab. Although this study did not identify factors that were predictive of mirikizumab efficacy over placebo, the multivariable analyses suggest that less severe disease inflammatory activity at baseline is associated with mirikizumab patients achieving DC at W12.
To date, clinical remission and endoscopic mucosal healing are the main treatment targets in patients with UC, while DC (symptomatic, endoscopic, and histologic remission) has more recently been proposed as the ultimate goal in the treatment of UC.14 The formal definition of DC, however, is still variable and not established by the medical community. Different definitions of symptomatic and endoscopic-histologic mucosal healing for DC have been suggested based on variable degrees of endoscopic healing (ES = 0 or ES = 1) and with/without inclusion of fCal. Other criteria have been consistent across several definitions of DC, including the requirement for reduced SF and no RB, as well as histologic remission with a Geboes score ≤2B.0, which is aligned with the European Crohn’s and Colitis Organization’s criteria of absence of neutrophils in the mucosa and absence of ulcers or erosions.15^,^16
In one multicenter, retrospective, cohort study, DC was defined as concurrent clinical (partial-Mayo score ≤2), endoscopic (endoscopic-Mayo score = 0), and histological (Nancy index = 0) remission. By this definition, patients with UC who had DC had a significantly lower risk for future hospitalization and surgery.17 In the VARSITY trial, however, DC was defined as a composite outcome with the following criteria, which are less stringent than the definition used in this present analysis: (1) clinical remission, partial Mayo score ≤2 and no individual subscore >1 (excluding sigmoidoscopy subscore); (2) endoscopic improvement, endoscopic subscore ≤1, and (3) absence of active histologic disease (minimum histological disease activity: Robarts Histology Index <5). At W52, 29.2% and 16.3% of patients in the 2 treatment groups had achieved DC.18 Meanwhile, in the ongoing VERDICT trial, DC was defined as achievement of a corticosteroid-free Mayo rectal bleeding subscore of 0 plus endoscopic improvement (Mayo Endoscopic Score ≤1) and histologic remission (Geboes score <2B.0). At W16, 34% of patients enrolled in the target group (corticosteroid-free symptomatic remission with endoscopic improvement and histologic remission) had achieved this target.19 Although a concept for “comprehensive disease control” has been proposed by Schreiber et al., including rectal bleeding, stool frequency, bowel urgency, abdominal pain, extraintestinal manifestations, disease-related quality of life (QoL), endoscopy, histological inflammatory activity, inflammatory biomarkers, use of corticosteroids, fatigue, and sleep disturbance, this disclosure focuses on the definitions of DC described above.20 Future disclosures may address “comprehensive DC” if appropriate data is available. Together, these trials show that DC is a very high bar to achieve, which is reflected by the overall low percentage of patients able to reach it. In our analysis, an alternative definition of DC included the concurrent achievement of symptomatic remission, HEMR, and fCal <250 μg/g, which is a more difficult endpoint to achieve than DC alone. As expected, DC and aDC results were aligned, as fCal is a surrogate for endoscopic and histological disease activity in UC even though thresholds may vary.
This analysis reveals that a significant number of patients achieved DC after 1 year of treatment with mirikizumab, and approximately 1 out of 2 patients attained this outcome after 2 years. This gradual increase in DC rates over time indicates a potential cumulative benefit of continued mirikizumab treatment. Additionally, the association between DC and the improvement of PROs is particularly noteworthy, suggesting that the clinical benefits of mirikizumab lead to tangible enhancements in patients’ QoL, a critical aspect of long-term treatment success. Finally, early achievement of DC by W12, which is associated with better long-term clinical outcomes, is encouraging; this implies that early responders to mirikizumab could anticipate more favorable long-term results, which healthcare providers should consider when making treatment decisions. Achievement of DC was not significantly associated with BU remission, indicating that BU may involve additional unique underlying mechanisms or correlates.
This analysis reveals evidence with DC that surpasses the current standard, supporting a more comprehensive approach to treating UC. The study demonstrates the effectiveness of mirikizumab in achieving DC, promoting a treatment goal. Furthermore, it establishes a clear connection between DC and improved clinical outcomes and PROs. This highlights the potential of mirikizumab to alleviate symptoms and alter the disease course, providing hope for patients seeking an enhanced QoL. Overall, the data support that mirikizumab is effective in achieving and sustaining DC in patients and has the potential for long-term benefits. The study promotes a more complete remission goal, demonstrating the need for a formal definition of DC to ensure consistency in clinical trials, improve comparability of outcomes, and support clinical decision-making.1
It is important to consider the limitations of the study. First, to date, there is no formal definition of DC. Within this disclosure 2 definitions are assessed and as discussed other definitions have been proposed by others. As all current definitions for DC use various combinations of clinical outcomes, studies specifically designed to formally define DC would greatly support both clinical trial design and, ultimately, clinical practice. Additionally, the association of early DC and later achievement of endoscopic remission, histologic remission, HEMR, and other clinical outcomes may be inherently correlated because those endpoints are DC components. Ideally, a prospective study assessing DC would be useful in providing a formal definition of DC. Interestingly, at W52 in the placebo group, 19.6% of patients achieved DC (Figure 1B), while 16.8% achieved aDC (Figure S4B), This relatively high PBO response rate was also observed in other primary and secondary outcome measures during LUCENT-1 and LUCENT-2 trials. A possible explanation for this is prior exposure to mirikizumab in the induction phase (Weeks 0-12).7^,^21–23 NRI is a conservative method used to handle missing data in clinical trials by classifying all patients with missing outcomes as nonresponders. While this approach can prevent overestimation of treatment effects, it may also underestimate efficacy, particularly when missing data are unrelated to treatment failure, potentially introducing bias and reducing statistical power. Last, as the study lacks multiplicity as a clinical trial it may not represent the broader real-world patient population.
5. Conclusion
Mirikizumab-treated patients are able to achieve and sustain disease clearance, improving patient outcomes over both short- and long-term treatment periods.
Supplementary Material
jjaf124_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D’Amico F , Magro F, Siegmund B, et al Disease clearance as a new outcome in ulcerative colitis: a systematic review and expert consensus. Inflamm Bowel Dis. 2024;30:1009-1017. 10.1093/ibd/izad 15937549104 · doi ↗ · pubmed ↗
- 2Ramos L , Teo-Loy J, Barreiro-de Acosta M. Disease clearance in ulcerative colitis: setting the therapeutic goals for future in the treatment of ulcerative colitis. Front Med (Lausanne). 2022;9:1102420. 10.3389/fmed.2022.110242036698823 PMC 9868775 · doi ↗ · pubmed ↗
- 3Hassan SA , Kapur N, Sheikh F, et al Disease clearance in ulcerative colitis: a new therapeutic target for the future. World J Gastroenterol. 2024;30:1801-1809. 10.3748/wjg.v 30.i 13.180138659483 PMC 11036494 · doi ↗ · pubmed ↗
- 4Andronic AM , Toader E. P 398 Disease clearance: a potential target for management of patients with ulcerative colitis. J Crohn’s Colitis. 2023;17:i 529-i 529. 10.1093/ecco-jcc/jjac 190.0528 · doi ↗
- 5Nascimento C , Réves J, Ramos LR, et al P 406 Disease clearance in patients with ulcerative colitis treated with aminosalicylates. J Crohn’s Colitis. 2022;16:i 398-i 398. 10.1093/ecco-jcc/jjab 232.533 · doi ↗
- 6Bryant RV , Costello SP, Schoeman S, et al Limited uptake of ulcerative colitis “treat-to-target” recommendations in real-world practice. J Gastroenterol Hepatol. 2018;33:599-607. 10.1111/jgh.1392328806471 · doi ↗ · pubmed ↗
- 7D’Haens G , Dubinsky M, Kobayashi T, et al; LUCENT Study Group. Mirikizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2023;388:2444-2455. https://www.nejm.org/doi/full/10.1056/NEJ Moa 220794037379135 10.1056/NEJ Moa 2207940 · doi ↗ · pubmed ↗
- 8Magro F , Pai RK, Kobayashi T, et al Resolving histological inflammation in ulcerative colitis with mirikizumab in the LUCENT induction and maintenance trial programmes. J Crohns Colitis. 2023;17:1457-1470. 10.1093/ecco-jcc/jjad 05037057827 PMC 10588772 · doi ↗ · pubmed ↗