A ‘second hit’ mouse model for group 2 and 3 pulmonary hypertension: combination of aortic banding and hypoxia exposure
Laura K Pallos, Michaela Matthey, Michael Hesse, Bernd K Fleischmann, Wilhelm Röll, Daniela Wenzel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
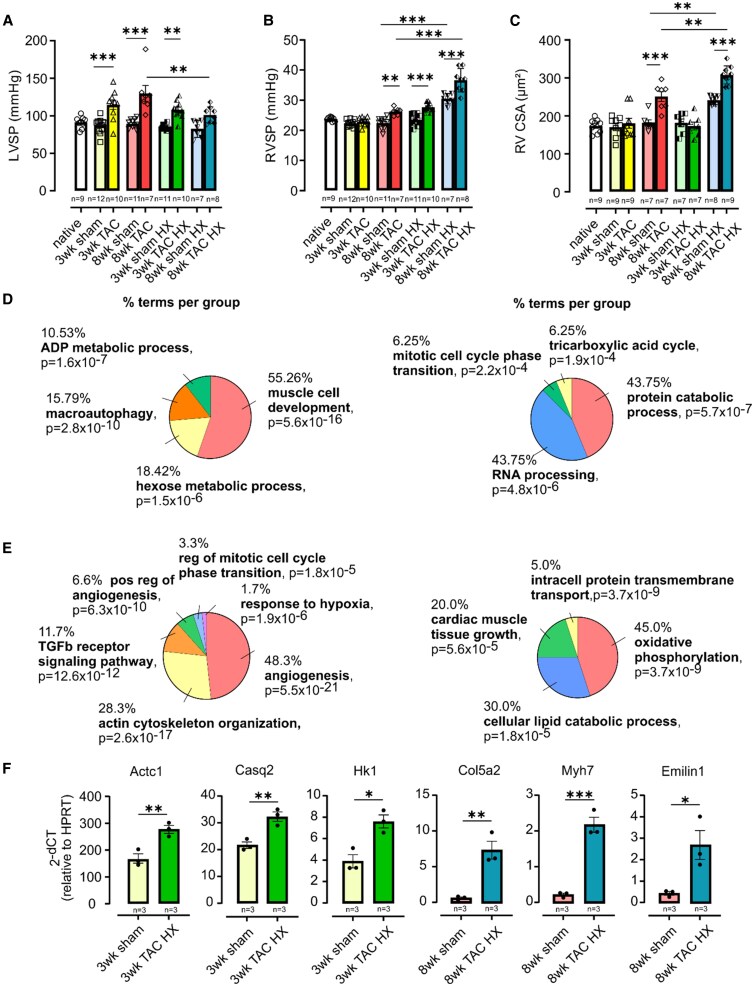 Figure 1
Figure 1- —BONFOR
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments
Group 2 pulmonary hypertension (PH) (due to left heart disease) and Group 3 PH (due to lung disease) are the most common and lethal forms of PH.^1,2^ Because not all patients with heart or lung disease develop PH, a ‘second hit’ model was proposed.^3^ This reflects the clinical situation, as many patients are diagnosed with an overlap of Group 2 and 3 PH, suggesting that either heart or lung disease may represent a ‘second hit’ that triggers the disease. We have therefore established a mouse model for combined Group 2 and 3 PH to test the ‘second hit’ hypothesis for these triggers of PH.
First, we established a model for Group 2 PH applying mild transverse aortic constriction (TAC) using a 26-gauge needle in C57BL/6 mice. Analysis was performed after 3 and 8 weeks. Macroscopic images of hearts and heart weight to body weight or tibial length measurements demonstrated increased organ size in the TAC group compared to sham-operated animals. As expected, functional analysis with echocardiography and Millar catheter revealed impaired LV function, an increase in LV systolic pressure (LVSP) (Figure 1A), and enhanced cross-sectional cardiomyocyte area (CSA) in the LV at both timepoints. RVSP and CSA in the RV were unaltered 3 weeks after TAC, but after 8 weeks, both parameters increased (Figure 1B and C), reflecting the time-dependent development of Group 2 PH. Sirius red staining showed fibrotic remodelling in the RV already as early as 3 weeks, which continued to progress through 8 weeks. We also found elevated pulmonary vascular wall thickness and lung fibrosis at both timepoints demonstrating lung remodelling.
To develop a ‘second hit’ mouse model for combined Group 2 and Group 3 PH, we exposed animals to mild TAC and additionally to hypoxia (HX, 10% O_2_) during the last 10 days of the 3-week and 8-week protocols. Successful TAC was again reflected by elevated heart weight and compromised LV function in TAC HX vs. sham HX animals.
At 3 weeks, the combination of TAC and HX resulted in elevated RVSP, indicating the development of PH already after 3 weeks, thereby aggravating the effects of TAC alone (Figure 1B). LVSP, LV CSA, RV CSA (Figure 1C), RV collagen deposition, and lung remodelling were similar to TAC alone.
At 8 weeks, HX during the last 10 days further increased RVSP but reduced LVSP compared to TAC alone (Figure 1A and B). This suggests an amplified contractile response to elevated afterload in the RV and potential early LV failure, as supported by echocardiography. RV hypertrophy was more pronounced (Figure 1C), whereas LV CSA remained unchanged compared to TAC alone. The stronger response in the 8-week sham HX animals compared to the 3-week animals may be related to their older age at the time of the experiment. Interestingly, RV and lung collagen deposition were reduced in TAC HX at 8 weeks compared to TAC alone.
To examine changes in the gene expression pattern of the RV, we performed RNA-seq analysis on sham, TAC, sham HX, and TAC HX animals at 3 and 8 weeks. To characterize the consequences of combined Group 2 and 3 PH on the RV, we analysed the unique genetic alterations of TAC HX vs. sham that were neither regulated in TAC vs. sham nor sham HX vs. sham. At 3 weeks, we found 658 differentially expressed genes (DEGs) uniquely regulated in TAC HX vs. sham (287 upregulated, 371 downregulated), and at 8 weeks, there were 468 DEGs (206 upregulated, 262 downregulated). Gene ontology (GO) analysis revealed upregulation of genes related to muscle development, angiogenesis, hexose metabolism/glycolysis, and response to HX (Figure 1D and E, left). Genes associated with catabolism, mitosis, and tricarboxylic acid (TCA) cycle/oxidative phosphorylation and also certain genes related to cardiac growth were downregulated (Figure 1D and E, right). The results were confirmed by qPCR analysis of key genes that are uniquely upregulated by TAC HX after 3 or 8 weeks (Figure 1F). These changes illustrate the biological and metabolic processes reflecting cardiac remodelling.
Herein, we propose a ‘second hit’ mouse model for PH by combining mild TAC with HX. Neither of the treatments alone could induce PH within 3 weeks, but their combination resulted in elevated RVSP, indicating the onset of PH. After TAC alone, our findings suggest that the pathomorphological changes occur later in the RV than in the LV, as proposed earlier by Platt et al.^4^ in a 26-gauge TAC model, where a delayed increase in RVSP and RV CSA was reported compared to LVSP and LV CSA. Fibrosis in both ventricles in our study correlates with pressure increase and hypertrophy in the LV but precedes the onset of haemodynamic changes in the RV. Such biventricular remodelling has previously been reported after inducing RV pressure overload and was attributed either to the mechanical interdependence of both heart chambers or to hormones and growth factors that affect the whole heart.^5,6^ There was no synergistic effect of TAC and HX on RV and lung collagen deposition, but a reduction after 8 weeks, possibly due to anti-remodelling effects of HX, as reported at least for the LV.^7^ Nevertheless, the RV genetic profile after TAC HX reflects a stress response, with upregulation of HX/HIF-1a-related genes, predicting pathological remodelling at 3 weeks and indicating established remodelling or hypertrophy at 8 weeks.^8,9,10^ Thus, we demonstrate the establishment of a mouse model for Group 2 and 3 PH, where heart or lung disease acts as a ‘second hit’ for PH development.
All animal experiments were conducted in compliance with the National Institutes of Health animal protection guidelines and approved by the local authorities [Landesamt für Natur, Umwelt und Verbraucherschutz, Nordrhein-Westfalen (LANUV), NRW, Germany].
For TAC surgery 30 min before the intervention, mice were injected with buprenorphine (0.1 mg/kg s.c.) for analgesia. Then, animals were anaesthetized by inhalation of 4–5% isoflurane and intubated with a 22 G needle. For maintenance of anaesthesia, isoflurane levels were reduced to 1.0–2.5%. For postoperative analgesia, buprenorphin (0.1 mg/kg s.c.) was injected twice a day and applied via the drinking water (1 mg/kg) overnight for 3 days. For transaortic echocardiographic analysis, mice were anaesthetized with 4–5% isoflurane, and for maintenance, 1.0–1.5% isoflurane was applied. For haemodynamic analysis, mice were anaesthetized with 4–5% isoflurane, intubated, ventilated, and placed on a heating plate (37°C). Then, ketamine (50 mg/kg) and xylazine (5 mg/kg) were applied i.p. For maintenance of anaesthesia, isoflurane levels were reduced to 1–1.5%. After the haemodynamic measurements, mice were sacrificed by cervical dislocation.
Authors’ contributions
L.K.P. performed animal and catheter measurements as well as echocardiography and histology and analysed data and contributed to the writing of the manuscript. M.M. analysed histological sections. M.H. performed RNA-seq analysis. B.K.F. discussed data and contributed to the writing of the manuscript. W.R. supervised animal experiments and analysis. D.W. designed the study, supervised the experiments, and wrote the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rosenkranz S, Gibbs JS, Wachter R, De Marco T, Vonk-Noordegraaf A, Vachiery JL. Left ventricular heart failure and pulmonary hypertension. Eur Heart J 2016;37:942–954.26508169 10.1093/eurheartj/ehv 512PMC 4800173 · doi ↗ · pubmed ↗
- 2Singh N, Dorfmuller P, Shlobin OA, Ventetuolo CE. Group 3 pulmonary hypertension: from bench to bedside. Circ Res 2022;130:1404–1422.35482836 10.1161/CIRCRESAHA.121.319970 PMC 9060386 · doi ↗ · pubmed ↗
- 3Yuan JX, Rubin LJ. Pathogenesis of pulmonary arterial hypertension: the need for multiple hits. Circulation 2005;111:534–538.15699271 10.1161/01.CIR.0000156326.48823.55 · doi ↗ · pubmed ↗
- 4Platt MJ, Huber JS, Romanova N, Brunt KR, Simpson JA. Pathophysiological mapping of experimental heart failure: left and right ventricular remodeling in transverse aortic constriction is temporally, kinetically and structurally distinct. Front Physiol 2018;9:472.29867532 10.3389/fphys.2018.00472 PMC 5962732 · doi ↗ · pubmed ↗
- 5Friedberg MK, Cho MY, Li J, Assad RS, Sun M, Rohailla S, Honjo O, Apitz C, Redington AN. Adverse biventricular remodeling in isolated right ventricular hypertension is mediated by increased transforming growth factor-beta 1 signaling and is abrogated by angiotensin receptor blockade. Am J Respir Cell Mol Biol 2013;49:1019–1028.23841477 10.1165/rcmb.2013-0149 OC · doi ↗ · pubmed ↗
- 6Andersen S, Birkmose Axelsen J, Ringgaard S, Randel Nyengaard J, Holm Nielsen S, Genovese F, Asser Karsdal M, Adler Hyldebrandt J, Brandt Sorensen C, de Man FS, Jan Bogaard H, Erik Nielsen-Kudsk J, Andersen A. Pressure overload induced right ventricular remodeling is not attenuated by the anti-fibrotic agent pirfenidone. Pulm Circ 2019;9:2045894019848659.30997866 10.1177/2045894019848659 PMC 6540527 · doi ↗ · pubmed ↗
- 7Froese N, Szaroszyk M, Galuppo P, Visker JR, Werlein C, Korf-Klingebiel M, Berliner D, Reboll MR, Hamouche R, Gegel S, Wang Y, Hofmann W, Tang M, Geffers R, Wende AR, Kuhnel MP, Jonigk DD, Hansmann G, Wollert KC, Abel ED, Drakos SG, Bauersachs J, Riehle C. Hypoxia attenuates pressure overload-induced heart failure. J Am Heart Assoc 2024;13:e 033553.38293923 10.1161/JAHA.123.033553 PMC 11056135 · doi ↗ · pubmed ↗
- 8Su Z, Liu Y, Zhang H. Adaptive cardiac metabolism under chronic hypoxia: mechanism and clinical implications. Front Cell Dev Biol 2021;9:625524.33604337 10.3389/fcell.2021.625524 PMC 7884626 · doi ↗ · pubmed ↗