Aphasia and Chronic Subdural Hematoma Evacuation: A Retrospective Cohort Study
Surya Patil, John J. Francis, Michelot Michel, Takuma Maeda, Anand Veeravagu, David Bonda, Peyton L. Nisson

TL;DR
This study examines aphasia recovery in patients undergoing chronic subdural hematoma evacuation, finding that most patients experience improvement or complete resolution of aphasia after surgery.
Contribution
The study is the first to report aphasia recovery rates after chronic subdural hematoma evacuation, providing insights for patient management and rehabilitation.
Findings
Left-sided chronic subdural hematomas are strongly associated with aphasia onset.
90% of patients showed aphasia improvement by discharge, with 73% achieving complete resolution.
Aphasia resolved in 83% of patients at follow-up within 180 days post-surgery.
Abstract
The incidence of subdural hematomas (SDH) is expected to climb precipitously in the coming decades. Aphasia is one of the most common operative neurological symptoms of left-sided SDH. However, the rates of aphasia recovery after SDH evacuation have not been reported as neurological outcomes have been limited to mostly functional assessment scores and mortality. This study represents the first detailed analysis on aphasia and recovery in patients undergoing chronic SDH (cSDH) evacuation. Adult patients who underwent evacuation of subacute or cSDH at a tertiary academic medical center between November 2013 and December 2021 were retrospectively identified using ICD 9 and 10 billing codes. Patients were categorized by the presence or absence of aphasia at initial presentation. Other clinical and demographic variables were also collected. After surgical evacuation, improvement and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
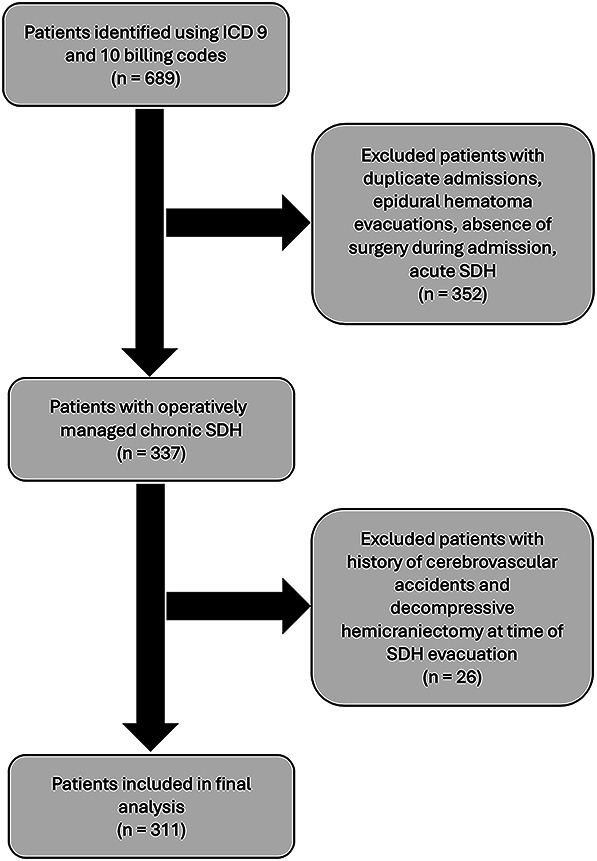 FIGURE 2
FIGURE 2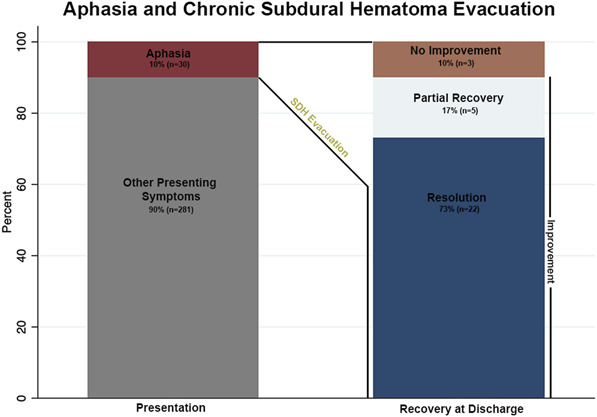 FIGURE 3
FIGURE 3| Characteristics | Aphasia | |||
|---|---|---|---|---|
| Absent | Present | Total | ||
| No. of patients | 281 (90) | 30 (10) | 311 | |
| Mean age, y (SD) | 71 (15) | 70 (15) | .83 | 71 (15) |
| Age range (y) | 22-100 | 30-89 | 22-100 | |
| Males | 214 (76) | 22 (73) | .73 | 236 (76) |
| Mean SDH size, mm (SD) | 21 (7) | 20 (8) | .50 | 21 (7) |
| Mean symptom duration, d (SD) | 9 (16) | 11 (20) | .54 | 9 (16) |
| Laterality | ||||
| Right | 110 (39) | 3 (10) |
| 113 (37) |
| Left | 103 (37) | 22 (73) | 123 (40) | |
| Bilateral | 68 (24) | 5 (17) | 73 (23) | |
| Midline shift present | 228 (82) | 21 (72) | .21 | 249 (81) |
| Surgery type | ||||
| Craniotomy | 234 (83) | 27 (90) | .44 | 261 (84) |
| Burr hole | 47 (17) | 3 (10) | 50 (16) | |
| Medical comorbidities | ||||
| Hypertension | 108 (38) | 15 (50) | .22 | 123 (40) |
| Diabetes mellitus | 38 (14) | 4 (13) | 1 | 42 (14) |
| Coronary artery disease | 35 (12) | 3 (10) | 1 | 38 (12) |
| Chronic heart failure | 11 (4) | 2 (7) | .47 | 13 (4) |
| Atrial fibrillation | 24 (9) | 2 (7) | .77 | 26 (8) |
| Aspirin use (Y) | 85 (30) | 6 (21) | .28 | 91 (29) |
| Plavix/brilinta (Y) | 20 (7) | 1 (3) | .70 | 21 (7) |
| Anticoagulation (Y) | 45 (16) | 4 (13) | 1 | 49 (16) |
| GCS at time of arrival | ||||
| 3-8 | 1 (0) | 0 | 1 (0) | |
| 9-12 | 16 (6) | 1 (3) | .81 | 17 (6) |
| 13-15 | 264 (94) | 29 (97) | 293 (94) | |
| GCS at time of discharge | ||||
| 3-8 | 8 (3) | 1 (3) | 9 (3) | |
| 9-12 | 3 (1) | 1 (3) | .57 | 4 (1) |
| 13-15 | 270 (96) | 28 (93) | 298 (96) | |
| Outcomes | Aphasia | |||
|---|---|---|---|---|
| Absent (n = 281) | Present (n = 30) | Total | ||
| Complications | ||||
| Urinary tract infection | 7 (3) | 0 | 1 | 7 (2) |
| Pneumonia | 5 (2) | 1 (3) | .46 | 6 (2) |
| Deep venous thrombosis/pulmonary embolism | 1 (0) | 0 | 1 | 8 (0) |
| Infection | 11 (4) | 1 (3) | 1 | 12 (4) |
| Seizure | 16 (6) | 4 (13) | .12 | 20 (7) |
| Trach/PEG placed (Y) | 13 (5) | 1 (3) | 1 | 14 (5) |
| Average length of stay days (SD) | 9.5 (10) | 15.5 (32) | .39 | 10.1 (14) |
| Reoperation | 36 (13) | 5 (17) | .57 | 41 (13) |
| Discharge location | ||||
| Nursing facility | 52 (19) | 3 (10) | .45 | 55 (18) |
| Rehab | 77 (28) | 12 (40) | 89 (29) | |
| Home | 140 (51) | 14 (47) | 154 (50) | |
| Hospice | 8 (3) | 1 (3) | 9 (3) | |
| Poor outcome at discharge (GOS 1-3) | 22 (8) | 1 (3) | .71 | 23 (7) |
| Inpatient mortality | 9 (3) | 1 (3) | 1 | 10 (3) |
| Logistic regression | Odds ratio | SE | 95% CI | |
|---|---|---|---|---|
| Age (y) | 1 | 0.01 | .93 | 0.98-1.03 |
| Sex (male) | 0.86 | 0.38 | .73 | 0.37-2.02 |
| cSDH laterality | ||||
| Right or bilateral |
|
|
|
|
| Left | 4.83 | 2.07 |
| 2.07-11.23 |
| SDH size (mm) | 0.97 | 0.28 | .33 | 0.92-1.03 |
| Midline shift (mm) | 0.95 | 0.04 | .186 | 0.87-1.03 |
| Hypertension | 1.6 | 0.62 | .22 | 0.75-3.41 |
| Patient no. | Age | Sex | SDH size (mm) | Laterality | Midline shift (mm) | Aphasia type | Postoperative improvement | Pertinent postoperative imaging findings | In Patient mortality | Resolution at FU | FU time (d) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 86 | M | 16 | L | 7.7 | Expressive | No | Residual blood products | No | No | 0 |
| 2 | 84 | M | 24 | L | 0 | Expressive | No | Infarct along L motor cortex | No | No | 90 |
| 3 | 72 | M | 14 | L | 8 | Expressive | No | No | No | No | 30 |
| 4 | 89 | M | 11 | L | 8 | Expressive | Yes | No | No | Yes | 90 |
| 5 | 75 | F | 14 | L | 0 | Expressive | Yes | Epidural hematoma (revision surgery) | No | Yes | 180 |
| 6 | 30 | M | 18 | L | 0 | Expressive | Yes | No | No | Yes | 30 |
| 7 | 83 | M | 24 | L | 14 | Expressive | Yes | Punctate Infarcts along L Anterior cerebral artery + Middle cerebral artery | Yes | No | 0 |
| 8 | 77 | M | L 12/R 16 | BL | 2 | Expressive | Yes | No | No | No | 90 |
| Authors | Location | Study type | Data date range | No. of patients presenting with aphasia | Recovery of aphasia (n (%)) |
|---|---|---|---|---|---|
| Moster et al | USA | SC case series | 1976-1980 | 9 | — |
| Dell et al | USA | SC case series | 1983 | 4 | 4 (100) |
| Kaminski et al | USA | SC case series | 1991 | 3 | 2 (66.7) |
| Rahimi et al | USA | SC case report | 2000 | 1 | — |
| Kuwahara et al | Japan | SC case report | 2004 | 1 | — |
| Blaauw et al | Netherlands | MC retrospective analysis | 2005-2019 | 45 | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurosurgical Procedures and Complications · Traumatic Brain Injury and Neurovascular Disturbances · Intracerebral and Subarachnoid Hemorrhage Research
The incidence of chronic subdural hematomas (cSDH) has increased significantly in recent years.^1^ This is likely a multifactorial phenomenon attributed to an aging population, rise in anticoagulant use, improvement in diagnostic tools and screening, and a higher incidence of traumatic brain injury-related incidents.^2-5^ According to the U.S. Census Bureau, by 2030, 20% of the U.S. population will be older than 65 years.^6^ This demographic shift can similarly be observed globally, with the United Nations projecting that by 2050, 1.5 billion individuals worldwide will be older than 65, with those aged 80 and older representing the fastest growing segment in developed countries.^7^
Elderly patients are particularly at risk of subdural hematoma (SDH)-related morbidity and mortality, because of factors such as increased use of antithrombotic medications, rising rates of neurodegenerative diseases such as Alzheimer's, and cerebral atrophy.^8^ cSDH are typically located along the convexity surface of the cerebrum and can present with a wide range of symptoms. Some of these can include headache, seizures, imbalance, lethargy, limb weakness, numbness, and aphasia.^9,10^ Despite the hematoma often spanning across the cerebral hemisphere's surface, it remains unclear why certain symptoms—such as aphasia—are selectively affected in some patients while others are spared. A schematic of the common treatment paradigm and features of SDHs is provided in Figure 1.
Aphasia, in particular, can have a profound impact on an individual's quality of life. Patients may face challenges with physical and psychological functioning, interpersonal relationships, and loss of independence, leading to increased risk of emotional distress and social isolation.^11,12^ Yet, few studies have focused specifically on aphasia in the context of cSDH.^13-18^ It is still uncertain whether certain risk factors, such as older age, size, or anticoagulation therapy, increase the likelihood of developing aphasia. Moreover, the rate of recovery of aphasia after cSDH evacuation has not been previously reported, which would be valuable in counseling patients and setting expectations after surgery. Most existing studies on SDH outcomes rely on general scoring systems such as the Glasgow Outcome Scale (GOS) or modified Rankin Scale, but few have addressed the recovery of specific neurological deficits.^19-24^
In this study, we present the first detailed analysis of aphasia and its recovery in a predominantly elderly patient population who underwent cSDH evacuation. In addition, we explore the frequency of aphasia and other symptoms at the time of diagnosis, as well as the respective recoveries.
METHODS
Patients consecutively treated at a tertiary academic center for SDH evacuation by a neurosurgeon were retrospectively identified from November 2013 to December 2021. The study included adult patients aged 18 and older. For patients with multiple admissions, only the initial encounter at the time of the primary surgery was recorded. Using International Classification of Diseases 9 and 10 billing codes, 689 patients were initially identified. After excluding 195 patients because of duplicate admissions, epidural hematoma evacuations, absence of surgery during admission, or acute SDH cases (157 patients), the focus narrowed to cSDH cases. SDHs were defined as chronic based on the presence of a primary hypodense, isodense, or mixed-density subdural collection.
Patients with a history of cerebrovascular accidents (23 patients) or those undergoing decompressive hemicraniectomy for cerebral edema at the time of SDH evacuation (3 patients) were also excluded to reduce confounding factors, leaving 311 patients for the final analysis (Figure 2).
Flow-chart demonstrating study design. SDH, subdural hematomas.
Data were extracted from electronic medical records, including demographic information (age, sex), medical comorbidities, anticoagulant or antiplatelet use, surgical type (craniotomy vs burr hole), and cSDH characteristics (size, laterality, midline shift). Neurological examinations at admission and discharge were recorded, including the Glasgow Coma Scale (GCS) score. If the GCS score was not explicitly stated, it was calculated from the neurological examination findings by research staff. Aphasia (present or absent) was assessed based on bedside neurological examinations performed by neurosurgeons. Aphasia was classified as expressive (motor), receptive (sensory), or mixed (both expressive and receptive components), per neurosurgeon documentation. Only patients who had aphasia consistently before surgery, as shown in their examinations, were counted as having aphasia for the study. Patients with globally poor neurological examinations (eg, GCS 3-8) without focal deficits such as aphasia were not classified as aphasic; only 1 patient presented with a GCS score of 3 to 8. Aphasia status postevacuation was tracked during hospitalization and at discharge, alongside inpatient evaluation by a speech-language pathologist (SLP) evaluation. For 1 patient with aphasia who died inpatient, aphasia was recorded as present at death for data collection purposes.
Postoperative anti-seizure medication was administered as clinically indicated. Complete resolution of aphasia during admission was determined based on the presence or absence of aphasia listed in the physical examination at the time of discharge or the time of most recent follow-up for persistent cases, with improvement defined as reduced aphasia deficits compared with admission on physical examination. Patients with persistent symptoms were followed until their latest neurosurgical follow-up. GOS scores were calculated at discharge from neurological examination findings, per McMillan et al definitions provided, with scores of 1 to 3 classified as poor outcomes.^25^ Data collection and GOS scoring were conducted by research staff, including 2 senior medical students and a neurosurgery resident, all trained in GOS assessment. All patients in the study were assessed, with no exclusions due to inability to calculate a GOS score.
This retrospective clinical study received approval from the hospital's institutional review board, with a waiver of patient consent for data collection. Statistical analyses were performed using STATA 14 software (Stata-Corp LP). Patients were stratified by preoperative aphasia status (present or absent) and logistic regression was used to identify predictors of aphasia. Continuous variables were compared using Student's t-test for parametric data or the Wilcoxon rank-sum test for nonparametric data. Categorical variables were analyzed with the χ^2^ test, or Fischer's Exact test when expected frequencies in any category were <5. Univariate and multivariable logistic regression analyses were conducted with aphasia as the dependent variable. To avoid insufficient cases in a single group, right-sided and bilateral cSDHs were combined into 1 category and compared against left-sided cSDH. In addition, for this same reason, only hypertension was included from the medical comorbidities recorded. A significance level of P < .05 was applied throughout, and any missing data were left blank during the analysis.
RESULTS
A total of 311 patients were included in this study. The mean age was 71 years, and most patients were men (76%, 236/311). The mean SDH size was 21 mm (range 7-40 mm), with midline shift present in 81% (249/311). A small craniotomy was the most commonly performed surgery, comprising 84% (261/311) of procedures, whereas the remainder were burr hole evacuations (16%, 50/311).
Ten percent of patients presented with aphasia as a symptom of cSDH (30/311). Most cases were holohemispheric (86.7%, 26/30) with the remainder localized to the frontal region. Expressive aphasia (25/30) predominated, whereas mixed aphasia occurred in the remaining patients (16.7%, 5/30). A comparison of demographics and SDH characteristics between patients with and without aphasia is presented in Table 1. Patients with aphasia had a significantly higher proportion of left-sided cSDH (73%, 22/30) than right (10%, 3/30) or bilateral (17%, 5/30). No significant differences were observed in age, sex, surgery type, medical comorbidities, antiplatelet use, or anticoagulation use. Outcomes were then compared between the cohort of patients with aphasia and those without. No significant differences were found including postoperative complications, length of stay, reoperation rate, discharge location, poor outcomes, mortality, and follow-up (Table 2).
Univariate logistic regression was then used to evaluate for risk factors of aphasia, including age, sex, SDH laterality (left vs right and bilateral), SDH size (mm), midline shift (mm), and hypertension (Table 3). Only left-sided SDH laterality was significantly associated with aphasia (odds ratio [OR] 4.89, 95% CI, 2.1-11.4, P < .001). A multivariable logistic model, adjusting for age, sex, and SDH laterality confirmed a similar association (OR 4.89, 95% CI, 2.09-11.41, P < .001).
After surgical evacuation, 90% (27/30) of patients had documented improvement in aphasia. Seventy-three percent (22/30) had complete resolution of aphasia by the time of discharge. Figure 3 summarizes the distribution of patients who presented with aphasia and the rates of recovery after surgery at discharge. Most of the patients (23/30) worked with SLP in the postoperative recovery period while inpatient. Of the 7 that did not, 1 died, 5 had resolved aphasia immediately after surgery, and 1 was transferred to an outside hospital.
Distribution of patients who presented with aphasia and the rates of recovery after surgery at discharge.
Patients with unresolved aphasia at discharge (n = 8) had their neurological examination at the most recent neurosurgery follow-up visits recorded. Table 4 provides a summary of these patients. Of the 3 without any improvement from the time of surgery, the first had persistent expressive aphasia with dysarthric speech and a small amount of residual acute blood products on the postoperative scan; no MRI or further follow-up occurred after discharge. The second had expressive aphasia with dysarthric speech that persisted at 90 day follow-up. Postoperatively, an MRI revealed a small infarct along the left motor cortex attributed to a small vessel bleeding near the pia that was identified after irrigation and cauterized during surgery. The third patient had nonfluent aphasia characterized by paraphasic errors and word retrieval deficits that persisted at the 30 day follow-up. Computed tomography of the head after surgery showed expected postoperative changes; no MRI was completed after surgery.
DISCUSSION
This study contributes to the limited literature on surgical outcomes and recovery in patients presenting with aphasia after cSDH evacuation. With the projected increase in cSDHs incidence over the coming years, neurological deficits such as aphasia are likely to become more prevalent among neurosurgical patients, underscoring the need for targeted research and interventions.^26,27^ In our cohort, 10% of patients requiring cSDH evacuation exhibited preoperative aphasia, a condition known to impair quality of life by affecting emotional well-being and social functioning.^11,12^ Of these, 90% demonstrated improvement by discharge, including 73% who achieved complete resolution, a rate that rose to 83% at the most recent follow-up. No significant differences were observed in outcomes or complication rates—including length of stay, reoperation rate, discharge location, poor outcomes (GOS 1-3), or mortality—between patients with and without aphasia. These findings offer valuable prognostic insights for counseling patients and families about expected recovery trajectories after surgery.
Regarding risk factors, left-sided lesion laterality was the only significant predictor of aphasia (OR 4.89). This increased risk in patients with left-sided SDH aligns with language lateralization to the left cerebral hemisphere in most individuals.^28^ Injuries to key language areas—most commonly Broca's area, Wernicke's area, the supplementary motor area, or the arcuate fasciculus—in the dominant hemisphere often result in aphasia. However, damage to deep subcortical structures, such as the internal capsule, caudate nucleus, or thalamus, may also contribute.^29^
Assessing aphasia in patients with cSDH may be challenging at times, because altered mental status, confusion, or depressed consciousness may obscure or mimic aphasic symptoms. In this cohort, however, 94% (292/311) of patients presented with high GCS scores of 13 to 15, facilitating reliable aphasia evaluation. One patient with a GCS score of 3 to 8 was intubated at presentation and classified as without aphasia; no aphasia was noted postextubation during that admission. Among the 17 patients with GCS scores of 9 to 12, only 1 exhibited aphasia. Given their small proportion (5.5%, 18/311) of the study population, patients with lower GCS likely had minimal impact on the overall detection of aphasia. Nevertheless, subtle language impairments may exist in some patients or persist in others undetected during standard neurosurgical examinations, which are also subject to interobserver variability.^30^ For instance, Blaauw et al^31^ conducted cognitive testing with the Telephonic Interview of Cognitive Status-modified 3 months post-cSDH evacuation and found that 54% of patients exhibited impaired cognition, scoring significantly lower in verbal memory and language/reasoning domains. These findings suggest that people who did not present with aphasia (90%) may still have subtle language deficits, emphasizing the potential need for more sensitive, standardized assessments to accurately detect aphasia in this population.
Few studies have reported on aphasia in the context of cSDH (Table 5).^13-18^ Two of the largest investigations by Blaauw et al and Moster et al, examined aphasia among cSDH patients, including 45 and 9 patients, respectively.^13-18^ These studies primarily focused on transient neurological deficits (TNDs), such as transient aphasia, potentially linked to seizures or cortical spreading depolarization, which may differ mechanistically from continuous, nonepisodic aphasia observed in our cohort.^32,33^ For example, Moster et al^13^ described the TNDs that resolved within 30 minutes or less in the 3 listed case reports, although 1 did have “mild global aphasia” as well present on examination that resolved after surgery. Blaauw et al^18^ had 1 patient with a 24-hour duration TND, although the median was 10 minutes, suggesting variability in the duration and severity of language deficits. As such, the exact timeframe used to classify TNDs as transient vs persistent preoperative neurological deficits remains unclear in the literature. Consistent with our results, Blaauw et al^18^ found no difference in age, sex, recurrence rate, mortality, or functional outcome between those with TNDs-including aphasia-and those without.
In addition to TNDs, cognitive impairment is also prevalent and may intersect with aphasia. A systematic review of cognitive impairment recovery reported a preoperative prevalence of 61% that dropped to 18% postsurgery, reflecting a 71% resolution rate.^34^ By contrast, our study found a lower preoperative aphasia prevalence (10%), but a similar resolution rate (73% at discharge). This discrepancy in prevalence may suggest underdetection of subtle language deficits in our cohort, potentially misclassified as broader cognitive impairment, whereas the similar resolution rates highlight the overlap between aphasia and cognitive impairment in language-related deficits.
With some isolated exceptions, most of the patients with aphasia in this cohort were evaluated and treated by SLPs during their hospital admission. Speech and language therapy plays a valuable role in recovery. A Cochrane review by Brady et al^35^ found that patients randomized to formal SLP intervention, compared with standard care, showed significant improvements in functional communication, reading, writing, and expressive language. Although this evidence stems from a poststroke population, many of these strategies are likely applicable to patients with cSDH. For example, Constraint-Induced Language Therapy, an intensive approach, restricts nonverbal communication alternatives to compel the brain to re-engage damaged language networks, promoting neuroplasticity.^36^
An intriguing finding in our study was the predominance of expressive aphasia, with no patients exhibiting isolated receptive aphasia. This may reflect selective vulnerability of motor neurons to injury in the content of cSDH. Motor neurons, which are relatively large and have high metabolic demands, may be more susceptible to the toxic effects of extravasated blood.^37^ Whole blood contains thrombin, hemoglobin, and free iron at concentrations far exceeding those required to induce neuronal death, with levels in whole blood reaching 7.5 times the thrombin, ∼1000 times the hemoglobin, and 1 to 3 times the free iron concentrations needed for half-maximal neuronal death.^38^ In addition, the large axons of motor neurons require a significant amount of energy, consuming 1 adenosine triphosphate molecule for every 8-nm displacement of cargo during axonal transport.^39^ This high dependence for continuous energy makes them especially vulnerable to energetic stress such as that may be induced by the mass effect and ischemia associated with cSDH.^40^ The predominance of expressive aphasia, which involves motor control of speech articulation, may also be influenced by the anatomic distribution of the hematomas in our cohort, which were more commonly located over the frontal lobe, potentially affecting the primary motor cortex and Broca's area. Alternatively, the absence of isolated receptive aphasia may suggest that sensory neurons in Wernicke's area, typically located in the temporal lobe, are less affected by the hematoma's location or have lower metabolic demands, although this requires further investigation.
Limitations of this study include its retrospective design, which may introduce selection bias, and its dependence on the accuracy of clinical documentation. Although most patients improved after cSDH evacuation, outpatient speech-language pathology interventions may have further enhanced aphasia recovery. However, the absence of documentation from contracted speech-language pathology facilities in the medical charts, coupled with loss to follow-up, precluded assessment of this contribution. Furthermore, the small number of aphasia cases (n = 30) likely underpowered the study, limiting detection of weaker associations in the logistic regression analysis. Similarly, with only 8 patients (27%) having residual aphasia at discharge, we were unable to robustly compare factors influencing recovery, such as age, hematoma characteristics, or SLP intervention, between those who did and did not regain full language function. Last, it would have been informative if all patients with persistent aphasia postoperatively had undergone MRI to evaluate for the presence of an infarct, which could explain incomplete recovery; however, this was not routinely performed. Future studies with prospective designs, standardized documentation, and larger sample sizes are needed to address these limitations and better elucidate the factors influencing aphasia recovery in cSDH patients.
CONCLUSION
Despite being a relative common pathology with a growing incidence, very few studies have specifically reported on aphasia associated with cSDHs. In this analysis, aphasia was found present in 10% of the 311 patients who underwent cSDH evacuation. Among these patients, all exhibited an expressive (83%) or mixed phenotype (17%), but none presented exclusively with receptive aphasia. With the exception of left-sided laterality, no patient characteristics, medical comorbidities, or antithrombotic medication use was identified as a risk factor of aphasia. After surgery, the majority improved and nearly three-quarters resolved by discharge, which increased to 83% at the most recent follow-up. These findings represent the first and largest series to address this topic, which may help guide treatment decisions and counseling for patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nouri A Gondar R Schaller K Meling T. Chronic subdural hematoma (c SDH): a review of the current state of the art. Brain Spine. 2021;1:100300.36247395 10.1016/j.bas.2021.100300 PMC 9560707 · doi ↗ · pubmed ↗
- 2Neifert SN Chaman EK Hardigan T Increases in subdural hematoma with an aging population-the future of American cerebrovascular disease. World Neurosurg. 2020;141:e 166-e 174.32416236 10.1016/j.wneu.2020.05.060 · doi ↗ · pubmed ↗
- 3Dossett LA Riesel JN Griffin MR Cotton BA. Prevalence and implications of preinjury warfarin use: an analysis of the national trauma databank. Arch Surg. 2011;146(5):565-570.21242422 10.1001/archsurg.2010.313 · doi ↗ · pubmed ↗
- 4Chen H Colasurdo M Malhotra A Gandhi D Bodanapally UK. Advances in chronic subdural hematoma and membrane imaging. Front Neurol. 2024;15:1366238.38725642 10.3389/fneur.2024.1366238 PMC 11079242 · doi ↗ · pubmed ↗
- 5Taylor CA Bell JM Breiding MJ Xu L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths - United States, 2007 and 2013. MMWR Surveill Summ. 2017;66(9):1-16.10.15585/mmwr.ss 6609 a 1PMC 582983528301451 · doi ↗ · pubmed ↗
- 6Vespa J Medina L Armstrong DM. Demographic Turning Points for the United States: Population Projections for 2020 to 2060. U.S. Census Bureau; 2020.
- 7UN Department of Economic and Social Affairs. Leaving No One Behind in an Ageing World. New York: United Nations Publications; 2023.
- 8Tenny S Thorell W. Intracranial Hemorrhage. Stat Pearls [Internet]; 2024.29262016 · pubmed ↗