PAIN2.0: study protocol for a multicentre randomised controlled trial to evaluate the efficacy of a 10-week outpatient interdisciplinary multimodal pain therapy to manage recurrent pain for patients with risk factors of developing chronic pain in Germany—update
Sandra Meyer-Moock, Daniel Szczotkowski, Leonie Schouten, Frank Petzke, Lena Milch, Beatrice Metz-Oster, Louise Zinndorf, Christian Geber, Greta Hoffmann, Anke Preißler, Ursula Marschall, Felix Rottke, Anja Waidner, André Möller, Thomas Isenberg, Gabriele Lindena, Anne Gärtner

TL;DR
PAIN2.0 is a German trial testing a 10-week outpatient therapy to prevent chronic pain in patients with recurring pain.
Contribution
The study introduces and evaluates an interdisciplinary multimodal outpatient pain therapy for chronic pain prevention.
Findings
The trial aims to reduce pain intensity and disability in patients at risk of chronic pain.
The intervention's effects will be analyzed through a 6-month follow-up and pre-post comparisons.
The study addresses recruitment challenges and adjusts its design to ensure meaningful results.
Abstract
Up to 27% of the German population suffers from recurrent or persistent pain (lasting more than 3 months). Therefore, prevention of chronic pain is one major object of pain management interventions. The aim of this nationwide, multicentre, randomised controlled trial is to evaluate the efficacy of a 10-week ambulatory (outpatient) interdisciplinary multimodal pain therapy (A-IMPT) for patients with recurrent pain and at risk of developing chronic pain. This project was initiated by the German Pain Society (Deutsche Schmerzgesellschaft e.V.) and the public health insurance provider BARMER. It is currently funded by the German Innovation Fund (01NVF20023). The study PAIN2.0 focuses on reducing pain intensity and pain-related disability and investigates whether this intervention can improve physical activity, psychological well-being, and health literacy. PAIN2.0 is designed as a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
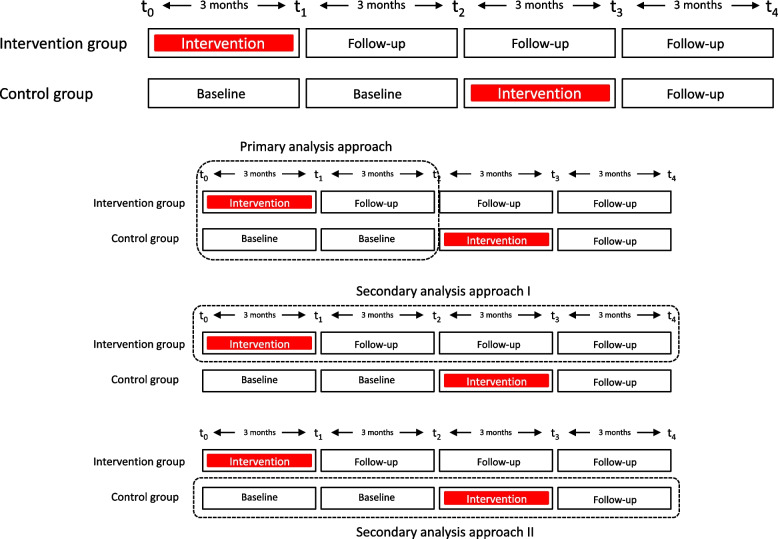 Figure 1
Figure 1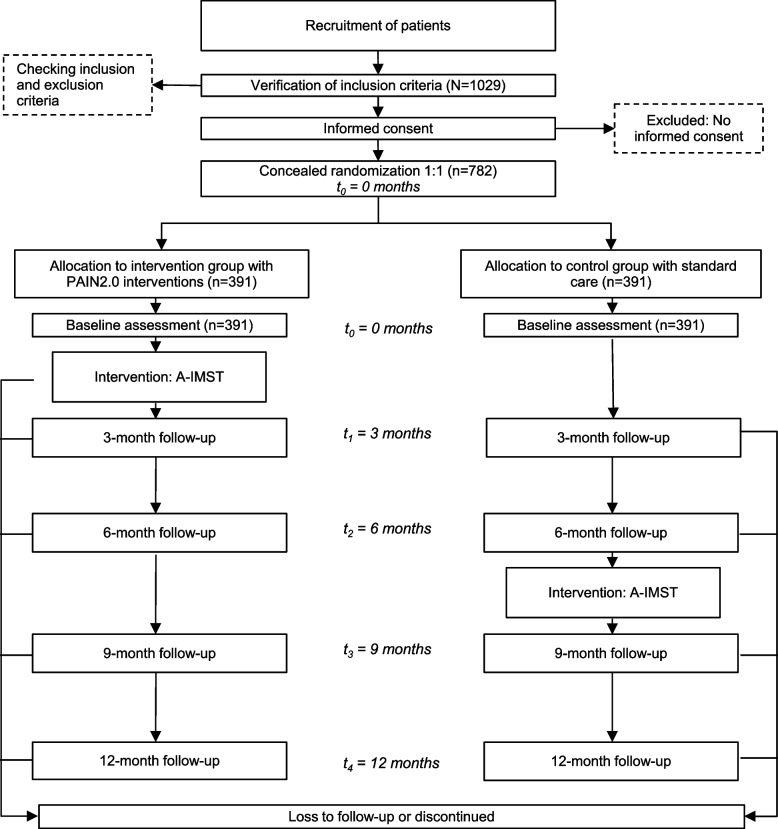 Figure 2
Figure 2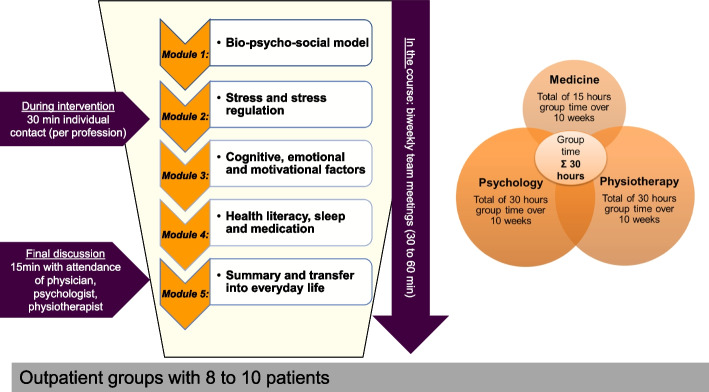 Figure 3
Figure 3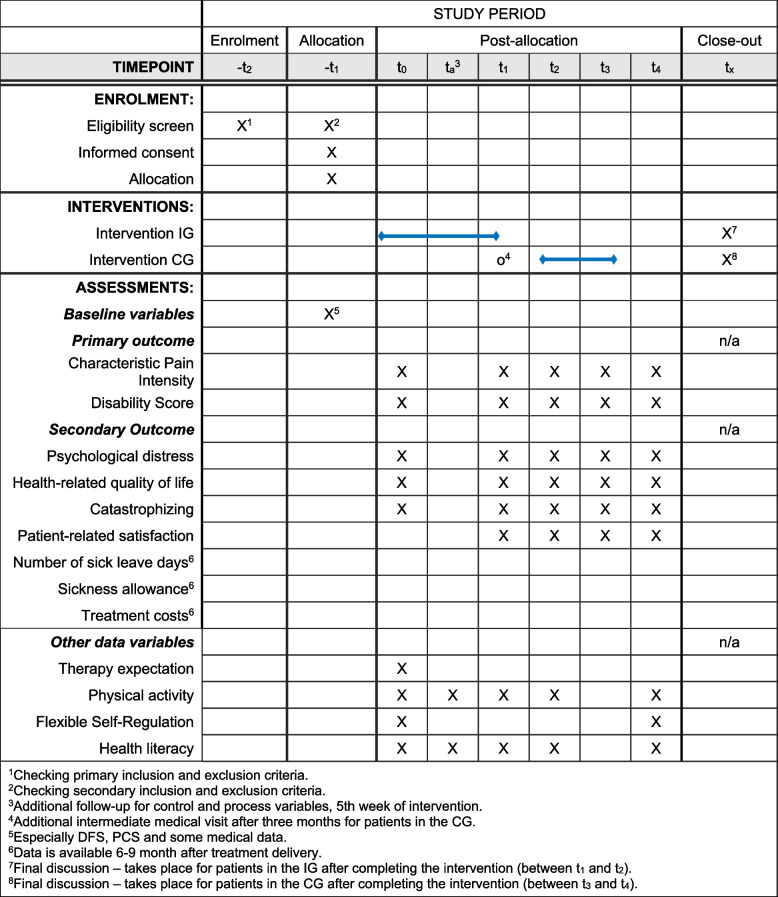 Figure 4
Figure 4- —Gemeinsamer Bundesausschuss (DE)
- —Universitätsmedizin Greifswald (8976)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Fibromyalgia and Chronic Fatigue Syndrome Research · Pain Management and Placebo Effect
Introduction
Background and rationale {6a}
‘Prevention of chronic pain’ was the theme of the International Association for the Study of Pain’s conference Global Year 2020 (IASP’s Global Year) [1]. However, activities to develop, evaluate and improve diagnostic and treatment options for prevention are still rare. Given the overall burden of chronic pain on individuals and society [2–4], the goal of preventing recurrent pain from becoming chronic should be a high priority for researchers, clinicians, and policy makers.
According to a nationwide survey of German citizens, approximately 27% experience recurrent pain in various locations, 7% experience recurrent pain with functional and somatic limitations, and 3% report recurrent pain with biological and psychosocial limitations [5]. These findings are consistent with other European studies [4].
Currently available diagnostic and treatment options commonly focus on the treatment and management of chronic pain. However, health care delivery for individuals transitioning from acute to chronic pain is often characterised by overtreatment with medications, invasive treatments (e.g. surgery) and imaging diagnostics, accompanied by undertreatment in the form of early psychosocial and interdisciplinary diagnostics and interventions [6]. These established approaches thus lead to iatrogenic effects (risk factors caused by the health care system, e.g. misinformed care givers or unimodal treatment approaches), enhancing the development of chronic pain forms in general [7]. Preventing individuals from developing impairing chronic pain conditions not only alleviates the burden on those affected but also helps save limited social and economic resources.
The perspective of prevention regarding pain management comprises three different stages [8]. Primary prevention focuses on identifying and improving maladaptive and non-functional workplaces and lifestyle habits that contribute to the occurrence of pain resulting from the over- or disuse of the body. Secondary prevention aims to maintain or improve physical and/or psychosocial functioning despite recurrent pain while preventing the development of chronic pain conditions. Tertiary prevention addresses individuals with chronic pain, thus reducing the risk of work disability, impaired social participation and the increase of psychological consequences such as depression, anxiety or loneliness. All approaches targeting pain and its management require the involvement of a multidisciplinary team in an integrated approach, ensuring the acknowledgement of the biopsychosocial nature of any kind of pain experience.
The biopsychosocial understanding of pain (either acute or chronic) [9] demands corresponding approaches covering biopsychosocial mechanisms of causing or maintaining recurrent pain experience. Biopsychosocial health care delivery (syn. also interdisciplinary, integrative pain care) includes complex interventions (multimodal), provided by a multidisciplinary team within an integrated team approach (interdisciplinary pain treatment, see IASP Homepage [10]). Key characteristics are equally contributed information and an integrated alignment on diagnoses and treatment components based on a shared understanding of the individual pain model of the patients using the same language and philosophy.
While biopsychosocial approaches have a well-established history in the treatment and management of chronic pain [11], their development in the context of prevention has been somewhat inconsistent.
Consequently, a concept of interdisciplinary group therapy was developed, piloted and adapted as outlined by Kaiser et al. in 2020 [12]. The intervention’s concept, which falls under the category of secondary prevention, draws from existing evidence regarding individuals with recurrent pain and those at risk of developing chronic pain.
The overall aim of PAIN2.0 is to improve the care of patients undergoing the transition from acute to chronic pain in an outpatient setting. The study involves the implementation of an ambulatory (outpatient) interdisciplinary multimodal pain therapy (A-IMPT) for individuals with persistent or recurrent pain, who, at the time of indication, have risk factors for the development of chronic pain and an increased physical and/or psychosocial disability.
PAIN2.0
PAIN2.0 is a consortium project of the Innovation Fund (01NVF20023) with a duration of 42 months.
The consortium leader is the German Pain Society (Deutsche Schmerzgesellschaft e.V.). The consortium partners involved in the project management (PM) are a public health insurance provider (BARMER), an external evaluation institute (Institute for Community Medicine, University Medicine Greifswald), as well as four institutions with profound experience in delivering interdisciplinary multimodal pain therapy (IMPT) (German Red Cross Pain Centre Mainz, University Hospital Carl Gustav Carus Dresden, University Hospital Schleswig-Holstein/Lübeck, University Medical Centre Göttingen).
Objectives {7}
The main objective of the project is to improve health care delivery for patients suffering from recurrent pain and present risk factors for chronification. Therefore, a therapy adapted to the needs of outpatients with pain is developed. The therapy entails delivering early information on the characteristics of pain, possible risks of chronicity, and the early identification of strategies to mitigate mechanisms that lead to chronicity. The transfer of a biopsychosocial understanding of the disease and specific knowledge about individual and contextual risk factors influences pain onset, equipping patients to develop adaptive coping strategies. The ultimate goal is to empower patients to take an active role in managing their pain. The following objectives for an outpatient interdisciplinary multimodal pain therapy are derived:
- Enhancing the sense of control and self-efficacy
- Teaching self-responsibility and building competence in the use of pain reduction techniques
- Introducing a biopsychosocial model
- Providing education about the specificity of pain
- Offering information on psychosocial risk factors
Therefore, the A-IMPT aims to (1) improve the objective and subjective performance as well as the subjective ability to control (physical activity and performance, health literacy, flexible self-regulation) and (2) prevent the development of chronic pain, especially in terms of pain intensity and pain-related impairment, compared to standard care.
The working hypotheses are:
- Over a 6-month period, participants in the intervention group are expected to report lower pain intensity than those in the control-group.
- Over a 6-month period, participants in the intervention group are expected to report less pain-related functional disability than those in the control-group.
Trial design {8}
The study is designed as a nationwide, multicentre randomised controlled trial (RCT), with two parallel groups to evaluate the efficacy of a 10-week outpatient interdisciplinary multimodal pain therapy. The duration of study participation is 12 months. Patients are enrolled consecutively from January 2023 to February 2024. Following verification of inclusion and exclusion criteria, they will be allocated to either the intervention group or the control group in a 1:1 ratio. The intervention is scheduled to occur between March 2023 and November 2024. Control group patients will receive standard care for 6 months, with the option to participate in the intervention program subsequently. Please refer to Fig. 1 for an overview of the study’s procedural timeline.Fig. 1. Timeline and analysis approach
Intervention effects will be analysed as follows:
- Essentially, the intervention effect will be evaluated by analysing the course of the primary and secondary outcomes in the intervention and control groups within the first 6 months (parallel-group comparison, t0 to t2) (Fig. 1b).
- In a secondary analysis approach, the long-term course of the new intervention is examined (t2 to t4). Further analyses of the outcome variables at these points are important for evaluating the stability of this effect over time (long-term) (Fig. 1c).
- The control group receives the intervention in the second half of the study period. The course of the primary and secondary outcomes in the control group after starting the intervention (t0 to t2 vs. t2 to t4) will be analysed (Fig. 1d). From a methodological perspective, this pre-post comparison can also help mitigating selection biases by increasing the willingness to participate in the study and reducing the drop-out rate within the control group.
Methods: participants, interventions and outcomes
Study setting {9}
Participating centres are healthcare institutions (n = 22) from all over Germany (distributed in 11 of 16 federal states): 18 centres are located in large cities, 3 centres in medium-sized cities and 1 centre in a rural region. Four centres are outpatient practices, 7 smaller hospitals and 11 larger hospital/university clinics. PAIN2.0 centres are health care institutions in Germany that already offer IMPT or that have the prerequisites for cooperation between the professions required for IMPT according to national scientific recommendations [13, 14]. The participating centres are listed in Table 1. Table 1. List of participating centres• Georg-August-Universität Göttingen, Universitätsmedizin Göttingen• DRK-Schmerz-Zentrum Mainz, gemeinnützige Trägergesellschaft Süd-West mbH• Universitätsklinikum Carl Gustav Carus and er der technischen Universität Dresden, AöR, Universitäts-Schmerz-Centrum Dresden• AMEOS Klinikum St. Elisabeth Neuburg• Universitätsklinikum Würzburg• Universitätsklinikum Freiburg• Vitos Orthopädische Klinik Kassel gGmbH• Brüderkrankenhaus St. Josef Paderborn• Schmerz- und Palliativzentrum Rhein-Main in Wiesbaden• Westmecklenburg Klinikum Helene von Bülow GmbH Hagenow• Universitätsklinikum Essen AöR• Medizinische Hochschule Hannover• Krankenhaus Bad Oeynhausen der Mühlenkreiskliniken AöR• Universitätsklinikum Schleswig-Holstein, Campus Lübeck• Krankenhaus Mörsenbroich-Rath GmbH, Düsseldorf• Praxis für ganzheitliche Schmerztherapie im Franziskus-Carré Münster• Universitätsklinikum Heidelberg• Berufsgenossenschaftliches Universitätsklinikum Bergmannsheil gGmbH Bochum• Universitätsklinikum des Saarlandes, Homburg• Asklepios Kliniken Hamburg GmbH–Asklepios Klinik Nord• Praxis für ganzheitliche Schmerztherapie Dr. Cayemitte-Rückner, Hamburg• Zentrum für ambulante Rehabilitation GmbH Münster
The centres play a crucial role in the implementation of the new intervention, undertaking vital responsibilities in patient recruitment (including patient information and securing informed consent), overseeing and documenting study-related procedures, collecting data, and transmitting data sets. Each centre receives comprehensive training on study protocols and tasks, both study-related and intervention-related. They actively participate in (online) project meetings and profession-specific intervision and undergo thorough monitoring. Additionally, these centres contribute to regional recruitment efforts, providing support and outreach within their respective areas.
Eligibility criteria {10}
Primary criteria for study inclusion comprise the following:
- New onset of pain (at least 6 weeks ago) or recurrent forms of pain or pain persisting for a longer period
- Pain-related limitations relevant to the patient (e.g. previous sick leave days, interference with daily life, family, leisure, work, and homework) and associated with reduced quality of life
- A risk of developing chronic pain (e.g. pain spread, negative mood, family and work stress factors, avoidance, and avoidance behaviour)
Patients must be at least 18 years old, have sufficient knowledge of the German language in spoken and written form, live in the vicinity of the participating health care facility, and have given their verbal and written consent to participate.
Primary criteria for study exclusion comprise the following:
- Clinical signs of a serious illness requiring urgent acute therapy or other serious illnesses (red flags; e.g. severe cardiac insufficiency, tumour)
- A manifest chronic pain condition that has already occurred (e.g. sick leave due to pain for more than 6 months, previous treatment with strong opioids for more than 3 years, previous IMPT)
- A severe and active psychiatric disorder (personality disorder, severe depression, signs of suicidal tendencies)
- An ongoing application for retirement
- A rehabilitation procedure planned for the near future
- Linguistic and/or cognitive impairments
The primary inclusion and exclusion criteria refer to the target population of PAIN2.0. However, there are additional secondary inclusion and exclusion criteria that are relevant for group participation and once again describe a subpopulation from the overall target population for inclusion in the PAIN2.0 group programme.
In addition to the general requirement of being able to participate in a 10-week group therapy and residing in close proximity to the facility, profession-specific secondary exclusion criteria were established. These secondary exclusion criteria included medical, physiotherapeutic, and psychological indicators that would limit regular participation in the therapy program and the benefits thereof. They are as follows:
Medical:
- Limited physical function for A-IMPT from a medical point of view, health check (check of exclusion criteria, medical)
- Presence of concomitant diseases that require special monitoring or limit the resilience for the A-IMPT
- Need for withdrawal treatment that requires continuous monitoring
- Existing drug dependence (e.g. opioids, benzodiazepines)
- Presence of an acute pain exacerbation that makes participation in the A-IMPT impossible
Psychological:
- Restricted psychological function
- Restricted social resources in terms of supporting constant group attendance
- Presence of a manifest, severe psychiatric/psychological diagnosis that primarily indicates psychotherapy (e.g. severe depression, personality disorder)
- Limited group capacity
- Restricted motivation to participate regularly
Physiotherapy:
- Limited self-care (i.e. daily physical activities, in the sense of managing personal affairs, personal hygiene and mobility)
- Limited mobility for participation in the A-IMPT
- Limited physical capacities
- Pronounced movement-related fear-avoidance behaviour
- Restricted movement-related competencies
- Indication for IMPT with higher intensity (‘more’ than A-IMPT)
- Need for priority, specific physiotherapy treatment.
Who will take informed consent? {26a}
Informed consent is obtained by the responsible physicians in the centres. They provide comprehensive information about the study and its schedules.
Before asking for consent, the procedure of inclusion contains two steps: primary inclusion criteria will be evaluated by the responsible physician and cover eligibility criteria as described above. Secondary inclusion criteria will be evaluated by the team (physician, physiotherapy and psychology). After fulfilling primary and secondary criteria, patients will be asked to give consent and will be consecutively included in the study.
Additional consent provisions for collection and use of participant data and biological specimens {26b}
N/a. There are no additional consent provisions.
Interventions
Explanation for the choice of comparators {6b}
The comparator is the standard healthcare as currently applied in the standard pain therapy in Germany. Patients in the intervention group will receive the new intervention at the beginning of the first 6 months, whereas participants in the control group will not receive any trial-related healthcare interventions. However, they are permitted to continue their pre-existing medical, physiotherapeutic and/or psychological (pain-related) therapies, which is often referred to as ‘treatment as usual’.
The comparator was chosen to identify the effects of the new intervention and to improve the currently applied pain therapy. Therefore, a comparison to ‘usual care’ is eligible. It is worth noting that patients in the control group also receive interventions after the initial 6 months (Fig. 2; see also Fig. 1).Fig. 2. Flow chart of participants
Intervention description {11a}
Interdisciplinary multimodal pain therapy [15] is commonly applied in chronic pain treatment. It is described as an integrative therapy approach consisting of somatic, psychotherapeutic, and physiotherapeutic interventions. Physicians, physiotherapists and psychologists collaborate equally in an integrative team approach and regularly coordinate and align on diagnosis, treatment plan and treatment progress. The primary goal of treating chronic pain by IMPT is to restore the patient’s subjective and objective functioning and self-control.
In this project, the IMPT is applied to an outpatient setting (A-IMPT) and adapted to the aims for the above-described target population.
The A-IMPT takes place once a week for 3 h in 10 sessions over 12 weeks in groups of 10 patients. It consists of 5 modules in total, each thematically grouped (Fig. 3). There are two sessions within each module, led by the respective professions. Throughout the 10 sessions, psychologists and physiotherapists are each present for a total of 30 h, while the presence of the physicians in the group sums up to 15 h. It is important to note that the content within each module is taught collaboratively by one or more professions.Fig. 3. Treatment plan and components of the A-IMPT
In the beginning, the general focus is on knowledge transfer, which is progressively expanded through practical exercises and integrated into the patient's background of experience (deepening of problem actualisation and enhancing motivational clarification). Therapeutic interventions (resource activation, problem-solving) are introduced from the beginning to support the transfer into everyday life. Each session ends with practical content (exercises, discussion, task to take home), which is taken up in the following week's session and leads into the new topic. In this way, patients experience health literacy to maintain a healthy, physically active lifestyle.
In addition to group therapy, all therapists also have the flexibility to offer 30 min of one-on-one time to each patient throughout the 10 weeks. Regular interdisciplinary team meetings are scheduled every 2 weeks to discuss each patient, lasting 30 to 60 min. A final meeting including the patient and all of the involved healthcare professionals of about 15 to 20 min completes the treatment. It serves to summarise the patient’s experiences, diagnoses, and further recommendations. As a conclusion, a collective final letter is written.
Coordination of group appointments, cancellations and provision of materials is handled by the documentation assistant or the nursing staff.
Criteria for discontinuing or modifying allocated interventions {11b}
Discontinuation of the study at the participants’ request is possible at any time during participation in treatment or the waiting period without giving reasons.
During participation and waiting period, patients continue to have full access to the health care system (i.e. primary care physicians or specialists). Changes in the participants’ medical treatment are assessed during the individual one-on-one contact with the physician as part of the A-IMPT. In the delayed treatment period of the control group, medical changes will be additionally assessed at the face-to-face interim contact (30 min) 3 months after study inclusion.
Reasons for study discontinuation also include any medical conditions that impact the participant’s ability to continue participating in the A-IMPT, whether they are related to pain or unrelated medical circumstances (e.g. need for urgent surgery or hospitalisation). Exacerbation of pain requiring intensified pain management (inpatient treatment/hospitalisation) will result in study discontinuation. However, discontinuation is not necessary if the pain exacerbation or new-onset pain can be adequately treated (including surgical intervention or short-term opioid prescription, if necessary) without compromising the ability to participate in the intervention (A-IMPT). Furthermore, physiotherapeutic and psychological reasons for study discontinuation are documented during the biweekly team meetings. The decision to discontinue the study is always made collaboratively by the treatment team.
Strategies to improve adherence to interventions {11c}
Before the start of recruitment, the centres receive training in the interventions, study documentation and data management, utilisation of assessment instruments, transmission of study documentation to the evaluating institutions, as well as the procedures and obligations regarding data validation. Training is mandatory; furthermore, written and video-based training materials are accessible through an access-restricted website.
A comprehensive monitoring concept has been developed and will be executed by the project administration (Deutsche Schmerzgesellschaft e.V.) in collaboration with consortium partners, including the German Red Cross Pain Centre Mainz, University Hospital Carl Gustav Carus Dresden, University Hospital Schleswig-Holstein/Lübeck, University Medical Centre Göttingen, and the evaluating institution (University Medicine Greifswald). The monitoring aims to oversee the implementation and adherence to the study protocol, provide direct feedback to the centres, and document any relevant deviations. It commences immediately after the recruitment and inclusion of the first patients.
For participants of the control group, an intermediate medical visit (interim contact) is scheduled after 3 months to prevent dropout. In addition to reassessing the status of the inclusion and exclusion criteria, a brief status report on the patient’s condition is given, and the patients should be motivated to attend the later intervention.
The principle of data management and monitoring has been described in a comprehensive data management plan.
Relevant concomitant care permitted or prohibited during the trial {11d}
Participants are allowed to continue pre-existing pharmacological and non-pharmacological therapies (treatment as usual; see also Sect. 6b) as long as these therapies do not interfere with the primary exclusion criteria (e.g. opioid intake > 6 month).
Provisions for post-trial care {30}
N/a. No provisions are planned.
Outcomes {12}
Primary outcomes
The primary outcomes are (1) characteristic pain intensity (PI) and (2) disability score (DS) for pain-related impairment. PI and DS are collected at baseline (t0) and at 3-, 6-, 9- and 12-month follow-up (t1 to t4). Changes in the primary outcomes between baseline (t0) and 6-month follow-up (t2) are evaluated as primary endpoints. Data are collected through a patient questionnaire, which includes the following:
(1) Characteristic pain intensity and (2) disability score are components of the Von Korff Chronic Pain Grade Scale (CPGS) [16]. The CPGS is a multidimensional measure with 7 items covering the two mentioned dimensions of overall chronic pain severity. The PI score is calculated as the average of three 0–10 ratings for ‘pain right now’, ‘average pain’ and ‘worst pain’, which is then multiplied by 10 to obtain a 0–100 score. The DS score is derived from the average of three 0–10 ratings for ‘daily activities’, ‘social activities’, and ‘work activities’, also multiplied by 10 to produce a 0–100 score. The last item covers the disability days.
Secondary outcomes
The secondary outcomes are (1) psychological distress, (2) health-related quality of life, (3) catastrophising (primary data), (4) patient-related satisfaction with the intervention, as well as (5) the number of sick leave days, (6) sickness allowance, and (7) treatment costs (secondary data). Primary data is collected through a patient questionnaire at baseline (t_0_) and on 3-, 6-, 9- and 12-month follow-up points (t1 to t4), which include the following:
- Psychological distress is evaluated using the short form of the Depression, Anxiety and Stress Scale (DASS) [17–20]. The DASS includes three subscales, each composed of 7 items: depression, anxiety, and stress.
- Health-related quality of life is measured by the Veterans RAND 12-Item Health Survey (VR-12) [19–24]. This assessment instrument comprises 12 items, which are used to calculate two separate sum scales for physical and mental health. Each sum scale includes all 12 items, with specific weightings applied to the 6 items associated with the physical sum scale and the 6 items linked to the mental sum scale. Higher values on these sum scales indicate elevated levels of either physical or mental health.
- The Pain Catastrophising Scale (PCS) [23, 25] examines catastrophising in regard to pain. The PCS consists of 13 statements covering a range of thoughts and feelings that patients may experience while in pain. The instrument comprises three subscales: rumination, magnification, and helplessness. Higher scores on these subscales indicate a more pronounced level of pain catastrophising.
- Patient-related satisfaction with the intervention is evaluated using an adapted version of the Patient Satisfaction Questionnaire (ZUF-8) [17, 18, 24, 25], which has been modified slightly to suit the outpatient context. Additionally, a global change item for assessing patient satisfaction is included in the evaluation.
Secondary data of the patients are made available by the participating health insurance BARMER (data source: BARMER scientific Datawarehouse, W-DWH) 6–9 months after treatment delivery and consists of the following:
- (5)Sick leave days: The dataset contains the number of sick leave days for each BARMER patient included in the study.
- (6)Sickness allowance: Additionally, the data set provides details about paid sickness allowance for each BARMER patient. These data, combined with sick leave days, form the basis for calculating the short- and long-term social costs related to incapacity to work.
- (7)Treatment costs: For each BARMER patient included in the data set, comprehensive cost data is available, covering expenses related to inpatient and outpatient care, medication, physiotherapy, occupational therapy, as well as assistive devices.
If these secondary data are not available, or not available to a sufficient extent, the number of sick leave days, medication, visits to specialists, inpatient facilities, and other medical service providers (e.g. rehabilitation) can be determined from the responses provided by the patient questionnaire.
In addition to the primary and secondary outcome measures, process variables and controls for confounders are also collected to examine the effects of the interventions.
- (8)Therapy expectation is evaluated using the Patient Questionnaire on Therapy Expectation and Evaluation (PATHEV) [26]. Treatment expectation encompasses the patient’s motivation and expectations regarding future treatment. Subscales assess hope for recovery, fear of change and its consequences, and the perceived alignment between treatment plan and the patient’s initial condition to be treated.
- (9)Physical activity is assessed using the European Health Interview Survey Physical Activity Questionnaire (EHIS-PAQ) [27–29]. The EHIS-PAQ is a questionnaire designed to evaluate the extent of physical activity in specific public health-related settings. It assesses physical activity related to work, transportation, and leisure in a typical week.
- (10)Flexible Self-Regulation is evaluated by the Self-Regulation-Inventory (SSI-K3) [30]. The construct of self-control describes conscious action on one’s own responsibility—i.e. the ability to set goals that fit one’s personality and to make the decisions that go with them. It also includes the ability to pursue these goals even over obstacles.
- (11)Health literacy is measured with two German specific questionnaires for assessing heath literature in this field: ‘Gesundheitskompetenzfragebogen’ (Health Literacy Questionnaire) [31] and ‘Fragebogen zur Erfassung der bewegungsbezogenen Gesundheitskompetenz’ (BGK, Questionnaire for movement-related health competence) [32]. The underlying concept of the Health Literacy Questionnaire is composed of the 3 facets of health literacy: ‘health goals’, ‘confidence to succeed’, ‘coping skills’. The BGK assesses physical activity-related health competence with individual items of a survey instrument based on the PAHCO model. The physical activity-related health competence (PAHCO) model assumes that individuals require three integrated sub-competences to lead a healthy, physically active lifestyle: movement competence, self-regulation competence and control competence. Selected subscales from each questionnaire are used.
Primary and secondary outcomes, additional variables and follow-ups are presented in Table 2. Table 2. Outcomes, additional variables, and follow-upsTimepoints/follow-upst0ta^1^t1t2t3t4Outcome variables****PrimaryCharacteristic pain intensityXXXXXDisability scoreXXXXXSecondaryPsychological distressXXXXXHealth-related quality of lifeXXXXXCatastrophisingXXXXXPatient-related satisfactionXXXXNumber of sick leave days^2^Sickness allowance^2^Treatment costs^2^Additional variablesControlTherapy expectationXProcessPhysical activityXXXXXFlexible self-regulationXXXXXHealth literacyXXXXX^1^Additional follow-up for control and process variables, 5th week of intervention^2^Data is available 6–9 month after treatment delivery
During the course of the project, the number of primary outcomes was reduced from three to two. PI and DS are the primary outcomes, while satisfaction with intervention, previously also a primary outcome, is now considered a secondary outcome. This change was necessary to ensure that the main effects of the intervention could be analysed with sufficient power, given the number of cases available.
Participant timeline {13}
The complete participant timeline is summarised in Fig. 4. Although details of the timing of enrolment, intervention, and assessments in the PAIN2.0 trial are shown in Figs. 1, and 3 and Table 2.Fig. 4. Time schedule of enrolment, interventions and assessments
Sample size {14}
During the initial phase of the project, it became clear that the originally planned sample size could not be achieved. For this reason, the required number of cases was recalculated based on the assumption that only two primary endpoints, including characteristic pain intensity (PI) and disability score (DS), would be investigated and that the primary analysis would refer to the 6-month measurement time point.
To determine the required number of cases, a simplified multilevel model was employed to examine group differences between standardised mean differences (SRMs) for the two primary outcome measures in the primary analysis approach. The SRM is calculated by dividing the pre-post differences between baseline and follow-up values (t0 to t2) by the respective standard deviation of the pre-post differences. The group differences are statistically tested using regression analyses, with the SRMs as the dependent variable and the group membership as the predictor variable.
Power calculation was performed using MLPowSim [33] in a simulation of power to detect group differences. The effect size was defined as the difference between group-specific SRMs, accounting for a residual variance of 1.0. The differences between the SRMs can therefore be interpreted directly as effect sizes. A value of 0.3 was chosen as the group difference to be detected. This corresponds to the size of a minimally significant difference in numerical rating scales in pain research [34]. Type I and type II errors were set at α = 0.05 and β = 0.20, respectively.
The results of the sample size calculation indicated a final sample size of 500 cases (statistical power of 80%, 2-sided significance level of 0.05). An expected drop-out of 20% over the 6-month comparison period leads to an increase in the required number of cases to be randomised initially to N = 782. Therefore, it is estimated that approximately N = 1029 individuals need to be screened to assess their eligibility criteria.
Recruitment {15}
Participants are recruited through:
- The participating health insurance (BARMER)
- Physicians, psychologists, and physical therapists within regional networks
- The study centres
The recruitment of insured individuals and patients, as well as their referral to the project, is carried out by the consortium partners’ project management, the PAIN2.0 centres themselves as well as by cooperating clinicians (general practitioners, specialists, company physicians and other health professionals). Recruitment measures are implemented in a systematic rotation and are repeated in conjunction with new information. The recruitment process spans a period of 5 or 6 months, with the first patient being enrolled in January 2023.
Recruitment of referring clinicians
An important factor of early patient care is the timely identification of risk factors by healthcare providers (including general practitioners, specialists, company physicians, orthopaedists, neurologists, physiotherapists, and other health professionals). With the support of the project team (e.g. collection of contact data of potential referrers), PAIN2.0 centres contact patients directly (in person, by telephone, by post), organise information events or collaborate with the regionally established general practitioner training activities and quality circles of various specialist groups (including pain conferences). This network effort is aimed at ensuring the sustainability of the new care service and thus is an important component of the project protocol.
Further, the consortium leader Deutsche Schmerzgesellschaft e.V. will contact national networks of potential referring professions and provide information about the study and intervention.
Recruitment of patients
Patient recruitment for the A-IMPT primarily relies on press releases and the websites of the participating centres. In addition, BARMER sends informative mail to insured individuals, based on healthcare data suggesting the onset of developing chronic pain. These individuals will have the option to contact BARMER’s specifically trained telephone counselling service (‘teledoctor’). The staff members of teledoctor perform a preliminary check of initial inclusion and exclusion criteria and refer the insured individual directly to the centre or provide the centre’s contact details. Other methods of patient recruitment include direct contact with PAIN2.0 centres through flyers, posters, newsletters, local advertising measures or activities on social media [35]. Patients can also reach out to the centre directly.
Recruitment via public relations work
The wider public is informed about PAIN2.0 through the homepage [36], national press releases, publications in specialised media (which not only highlight the unique aspects of the patient group but also describe the innovative A-IMPT care service), outreach to associations, medical associations and businesses as well as advertising on social media platforms. These initiatives are coordinated by the consortium partners’ project management. Interested referring clinicians and patients can contact the PAIN2.0 centres directly.
In preparation for recruitment, numerous recruitment options were presented to the centres in video conferences, and sufficient materials for implementation were handed out (including cover letters, webinars and regional press releases). During the recruitment phase, support and exchange were offered to the centres in video conferences or in the context of individual centre support. To ensure the consistency of project communications, the project team developed text modules that were tailored to different target groups, including patients, the professional public, and the general public. These modules were applied in a standardised manner.
Assignment of interventions: allocation
Sequence generation {16a}
Lists of randomised blocks of varying lengths were generated by the evaluating institute for each participating centre and implemented in the PAIN2.0 database.
Concealment mechanism {16b}
Lists of randomised blocks used in the external randomisation were not known to the recruiting centres at the time of patient enrolment.
Implementation {16c}
Patients are enrolled by physicians who verify the primary inclusion and exclusion criteria.
Those patients who fulfil both the primary and secondary inclusion criteria and have no reasons for exclusion are consecutively included in the study.
Patients providing informed consent were randomly assigned to the intervention or control group by the medical documentarians during study enrolment.
Assignment of interventions: blinding
Who will be blinded {17a}
N/a. Blinding is not possible.
Procedure for unblinding if needed {17b}
N/a. There is no blinding.
Data collection and management
Plans for assessment and collection of outcomes {18a}
Prior to the start of recruitment, the participating centres will receive training on the interventions, the utilisation of assessment instruments, handling the study documentation, forwarding the study documentation to the evaluating institutions, and the process and obligations for data validation.
At the time of enrolment (i.e. before t0), patients will be asked to complete the standard questionnaire of the German Pain Society (DSF) [37]. In addition, medical data is assessed. Further data collection is done through questionnaire surveys at baseline and at 3-, 6-, 9- and 12-month follow-ups. In addition, a process evaluation questionnaire is to be completed in the fifth week of the intervention (Fig. 4).
Data is archived in a PAIN2.0 database, which contains all documentation.
Monitoring is conducted by the central project coordinator (Deutsche Schmerzgesellschaft e.V.), the consortium partners German Red Cross Pain Centre Mainz, University Hospital Carl Gustav Carus Dresden, University Hospital Schleswig-Holstein/Lübeck, University Medical Center Göttingen, and the evaluating institution (University Medicine Greifswald).
Questionnaires are available at the German Pain Society (Deutsche Schmerzgesellschaft e.V.).
Plans to promote participant retention and complete follow-up {18b}
To promote participant retention, several procedures have been introduced. Participants in the intervention group receive one individual contact with each professional group during the 10-week therapy. These individual contacts last 30 min each and can be split into two appointments of 15 min each if necessary. Participants in the control group receive an additional intermediate medical visit after 3 months to prevent dropout. The questionnaire response is monitored through the database. If a questionnaire is not returned on time, two follow-up actions are taken. Patients who do not regularly attend the interventions will be contacted by the study centre. Reasons for discontinuation are documented.
A list of outcome data will be compiled for participants who discontinue or deviate from the intervention protocols. This will include detailed information on participants who drop out of the intervention or deviate from the study protocol.
Data management {19}
Data archiving takes place in a PAIN2.0 database that holds all documentation. The principle of data management and data protection has been described in a comprehensive data management plan.
Confidentiality {27}
The following patient data are collected and processed in the centres:
- Administrative data (e.g. name, date of birth, health insurance company, and the name of the responsible study doctor) only remain in the centres and are used for medical care according to the study conditions and for the organisation of follow-up interviews and group procedures. These data must be retained for a period of 10 years. The list remains at the centre and is the only link between pseudonymised patient ID and the health insurance data.
- All other information on patient care and evaluation is entered into the PAIN2.0 database exclusively in pseudonymised form, following the written consent of the study participants. In the PAIN2.0 database, the pseudonymised patient data for each centre are presented in separate overviews, with data from other centres being inaccessible.
Questionnaire data for evaluation is entered into the PAIN2.0 database exclusively in pseudonymised form.
Plans for collection, laboratory evaluation and storage of biological specimens for genetic or molecular analysis in this trial/future use {33}
N/a. There are no plans for collection, laboratory evaluation and storage of biological specimens for genetic or molecular analysis in the current trial and future use in ancillary studies.
Statistical methods
Statistical methods for primary and secondary outcomes {20a}
The primary analysis model for the two primary outcomes (pain intensity and disability score at 6 months adjusted for baseline values) is a linear mixed regression model with a random intercept.
The values of the primary outcomes at time t3 (6-month follow-up) serve as the dependent variables. To describe the effect of the intervention, the baseline value at time t_0_ and group membership are used as predictor variables [38, 39]. As two primary endpoints are analysed simultaneously, adjustment for multiple testing using Bonferron’s method will be applied.
When using these models, it is possible to include further predictor variables in the analysis. This can be of interest if, despite randomisation, relevant differences occur between the study arms and must be statistically controlled, or if the effects of covariates (e.g. of age or other patient characteristics) are to be analysed. Through appropriate model specification, all hypotheses of interest can be tested with these analysis methods.
The analysis of the primary endpoints will be conducted according to the intention to treat (ITT) principle.
The primary and secondary outcomes to be investigated are predominantly continuous data for which linear regression models can be used. However, the family of (generalised) mixed models also allows analogous evaluations for other types (ordinal or categorical) of dependent variables.
In the context of the analysis of days of incapacity to work or cost data, it may furthermore be necessary to use special analysis methods for data with an asymmetric distribution or with heavily populated zero cells (‘zero-inflated’).
Statistical significance tests are performed with an α-level of 0.05 (two-sided). In the confirmatory analysis of the primary outcome measures, a Bonferroni adjustment for multiple testing (3 outcome measures, 2 follow-up times) is applied. No such adjustment is used in the exploratory analyses of the secondary outcomes.
Interim analyses {21b}
N/a. Interim analyses are not planned.
Methods for additional analyses (e.g. subgroup analyses) {20b}
Level of centres
Additional investigations will evaluate existing process and structural parameters as required by the study protocol (e.g. consistency in team collaboration, availability of complete staff, aspects of coordinating treatment groups and plans, qualification of staff, perceived quality of interaction between staff members while conducting group or team meetings).
Patient level
Parameters for evaluating the delivery of intervention will be gathered during the treatment period (process parameters, see above). Satisfaction of patients with group delivery and perceived relationship and support by caregivers will be evaluated additionally.
Subgroup formation is planned primarily for the centre level. Centres will be grouped according to local parameters (size of community, local health care delivery and networks in terms of pain management), and will consider the process and structural parameters of the centre (main delivery) and delivery of the study intervention.
Subgroup analyses as described above will be conducted as exploratory analyses.
Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing data {20c}
In longitudinal analyses involving more than one follow-up time point, the family of (generalised) mixed models uses all available data, even if data at some time points are missing. If necessary (e.g. in case of high drop-out-rates > 30%), appropriate methods of (multiple) imputation of missing values will be employed. The population for primary analysis includes all patients for whom PI and DS data are available at baseline and at 6-months-follow-up.
Plans to give access to the full protocol, participant level-data and statistical code {31c}
The full protocol is available online at DRKS [1]; the statistical code will be provided at the end of the study upon reasonable request. Due to existing data protection rules, no access to the participant-level dataset is planned.
Oversight and monitoring
Composition of the coordinating centre and trial steering committee {5d}
PAIN2.0 is a consortium project; the consortium leader is the German Pain Society (Deutsche Schmerzgesellschaft e.V.) in collaboration with the health insurance company BARMER. The consortium partners involved in the project management (PM) are BARMER, an external evaluation institute (Institute for Community Medicine, University Medicine Greifswald), as well as four institutions with extensive experience in interdisciplinary multimodal pain therapy (IMPT): German Red Cross Pain Centre Main, University Hospital Carl Gustav Carus Dresden, University Hospital Schleswig-Holstein/Lübeck, University Medical Centre Göttingen, University Medicine Greifswald.
The consortium is responsible for the project conception and implementation, the organisation of centre and patient recruitment, support in local network formation as well as the monitoring of the study.
Consortium partners deliver the intervention and fulfil study related tasks (PAIN2.0-Centers, see Table 1).
An annual Advisory Board consisting of representatives of various committees of the German Pain Society is appointed to advise on the conduct of the study.
Composition of the data monitoring committee, its role and reporting structure {21a}
The consortium project management is responsible for the project monitoring of the study. It consists of the consortium partners German Pain Society (consortium leader), University Medical Centre Göttingen, German Red Cross Pain Centre Mainz, University Hospital Carl Gustav Carus Dresden, University Hospital Schleswig-Holstein/Lübeck, University Medicine Greifswald, and BARMER. All monitoring activities take place independently from the sponsor.
Adverse event reporting and harms {22}
N/a. The occurrence of adverse events is not expected in this trial.
Frequency and plans for auditing trial conduct {23}
Monitoring and auditing a multicentre study with a complex intervention presents unique challenges. The monitoring concept of PAIN2.0 encompasses two key areas:
- Monitoring of case number achievement, recruitment, and admission according to study protocol and
- Monitoring the implementation of the provided intervention and follow-up surveys according to study protocol.
One of the objectives of the monitoring is to ensure the implementation purity of the project protocol in each participating PAIN2.0 centre, considering the different local conditions and prerequisites. In addition, the monitoring also serves to ensure treatment purity as a prerequisite for the strength of the intervention, including the hypothetically assumed effects. The third objective involves the collection and evaluation of the facilities’ experiences in recruiting suitable patients as well as in implementing the new care service, which are of high importance for the subsequent possible roll-out. For each area, the following 5 levels of monitoring are currently envisaged:
- Continuous data monitoring (monthly, individually for each centre): The documentation as well as the implementation of the study (inclusion and A-IMPT) will be monitored via criteria defined in the project team for implementation purity (about the project protocol, including checking primary and secondary inclusion and exclusion criteria) and treatment purity (including implementation of the A-IMPT; reviewing data base). In the event of a relevant deviation from the project protocol, the responsible PAIN2.0 centre will be contacted and will undergo further monitoring.
- Individual audit reports (monthly to quarterly, individual for each centre): During the recruitment phase (January 2023 to November 2023), there will be a monthly individual centre report on caseload management for the PAIN2.0 centres including selected data on implementation and admission purity (retrieved from data base; including caseload, referral pathways, patient characteristics, randomisation). During treatment delivery (March 2023 to August 2024), a quarterly audit report will be provided to reflect intervention purity according to study protocol.
- Ongoing PAIN2.0 Talks/Ongoing Video Conferences (monthly, online): All centres are invited to participate in 1-h profession specific talks. The main goal of these monthly meetings is to provide information and resolve any questions or obstacles. The discussions primarily focus on admission and later in the process on the delivery of the health care intervention. A regular protocol is sent out to all members of all centres after completed talk-rounds.
- Visit audits (once for each centre after completing study enrolment and admission): A single visit to each centre is planned to prepare for data delivery after completing the recruitment phase.
- Final audit (twice; one after completed admission/enrolment, one after completing intervention delivery; individually for each centre; online): Monitoring of data entry, quality of data and the compliance of data protection law are focus of the final audits. Reports provide feedback of open or pending tasks of the centres to close data acquisition and management, allowing the start of data delivery to the evaluation institute and to the project team for further/final analyses.
Plans for communicating important protocol amendments to relevant parties (e.g. trial participants, ethical committees) {25}
Protocol modifications (e.g. changes to eligibility criteria, outcomes, analyses) to relevant parties (e.g. trial participants, ethical committees, investigators, institutional review board, trial participants, trial registry) are communicated by the study coordinating centre (Deutsche Schmerzgesellschaft e.V.) and will be published in the preregistration of this study [40].
Dissemination plans {31a}
The study protocol is available as an open access publication in agreement with SPIRIT [41, 42] and CONSORT [43] criteria. The final trial dataset will primarily be available for the data centre of the project and the independent evaluation institution (University Medicine Greifswald).
Data protection regulations restrict the use of the trial data to purposes and by institutions agreed upon by participants who have provided written informed consent. Any queries regarding data availability can be forwarded to the corresponding author. The trial results will be made available by scientific publication and reported to the funding body.
Authorship eligibility guidelines for publishing peer-review journals will be applied.
Discussion
Recurrent or persistent pain is a widespread issue in the German population, imposing significant costs on individuals and society due to physical and psychosocial impairment. PAIN2.0 is designed to improve the health of individuals with recurrent pain and associated risk factors, subsequently reducing the costs incurred.
Intensive forms of therapy or management programs for chronic pain have already been shown to be cost-effective for chronic pain [44]. Thus, long-term cost reductions can be expected by preventing the occurrence of severe physical and psychosocial impairments and avoiding chronic courses of pain. The study results of PAIN2.0, alongside the economic feasibility analyses, serve as the foundation for integrating outpatient interdisciplinary pain therapy to improve recurrent pain into standard care.
The fact that the study involves a complex intervention is a potential limitation. An equally complex monitoring concept attempts to ensure the comparability of the intervention to be carried out. In addition, regular data monitoring and monitoring of process and structural quality ensure compliance with the study protocol.
Overall, the new form of care could be included in standard practice pending convincing results and approval from the German Federal Joint Committee.
Trial status
Protocol version number: study protocol version 1.3 dating from 04/09/2022.
Start of recruitment: 01/01/2023.
End of Recruitment: 28/02/2024.
A revision of the study protocol became necessary as bottlenecks in the planned recruitment numbers arose during the recruitment process. The modification relates in particular to the reduction of the primary endpoints to two. Pain intensity and pain-related functional impairment (Von Korff Index) are defined as primary endpoints. Patient satisfaction is now only analysed as a secondary endpoint. The revision enables an appropriate and meaningful evaluation study despite a noticeable reduction in the number of cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Association for the Study of Pain. https://www.iasp-pain.org/advocacy/global-year/prevention-of-pain/#:~:text=IASP%20Dedicates%202020%20Global%20Year%20to%20the%20Prevention%20of%20Pain&text=Brona%20Fullen%20and%20Dr.,Esther%20Pogatzki%2D Zahn. Accessed 20 September 2023.
- 2Dietl M, Korczak D. Over-, under- and misuse of pain treatment in Germany. GMS Health Technol Assess. 2011;7. 10.3205/hta 000094.10.3205/hta 000094 PMC 308066121522485 · doi ↗ · pubmed ↗
- 3Nicholas MK, Linton SJ, Watson P, Main CJ, Decade of the Flags Working Group. Early identification and management of psychological risk factors ("yellow flags") in patients with low back pain: a reappraisal. Phys Ther. 2011;91:737–53.10.2522/ptj.2010022421451099 · doi ↗ · pubmed ↗
- 4IASP terminology. https://www.iasp-pain.org/resources/terminology/. Assessed 20 September 2023.
- 5Müller-Schwefe G, Nadstawek J, Toelle T, Nilges P, Überall MA, et al. Struktur der schmerzmedizinischen Versorgung in Deutschland: Klassifikation schmerzmedizinischer Einrichtungen. Schmerz. 2016;30:2018–26.10.1007/s 00482-016-0119-427221745 · doi ↗ · pubmed ↗
- 6Schmidt J, Lamprecht F, Wittmann WW. Zufriedenheit mit der stationären Versorgung. Entwicklung eines Fragebogens und erste Validitätsuntersuchungen [Satisfaction with inpatient management. Development of a questionnaire and initial validity studies]. Psychother Psychosom Med Psychol. 1989;39(7):248–55.2762479 · pubmed ↗
- 7Buchholz I, Kohlmann T, Buchholz M. Vergleichende Untersuchung der psychometrischen Eigenschaften des SF-36/SF-12 vs. VR-36/VR-12. Abschlussbericht. 2017. https://www.reha-vffr.de/images/vffrpdf/projekte/2017/VR-Abschlussbericht_vffr 205.pdf. Accessed 13 September 2023.
- 8Finger JD, Tafforeau J, Gisle L, et al. Development of the European Health Interview Survey - Physical Activity Questionnaire (EHIS-PAQ) to monitor physical activity in the European Union. Arch Public Health. 2015;73:59. 10.1186/s 13690-015-0110-z.10.1186/s 13690-015-0110-z PMC 466744826634120 · doi ↗ · pubmed ↗