Pregnancy and neonatal outcomes in women with arcuate uterus: a population-based cohort study of over 3.8 million women
Nir Kugelman, Ella M. Gangbe, Ahmad Badeghiesh, Haitham Baghlaf, Michael H. Dahan

TL;DR
Women with an arcuate uterus face higher risks of complications during pregnancy and childbirth, including cesarean sections and coagulopathy.
Contribution
This study is the first large-scale population-based analysis of pregnancy outcomes in women with an arcuate uterus.
Findings
Women with an arcuate uterus had significantly higher rates of cesarean sections and preterm delivery.
They also faced increased risks of preeclampsia, placental abruption, and neonates small for gestational age.
Compared to matched controls, they showed higher odds of postpartum hemorrhage and wound complications.
Abstract
Congenital uterine anomalies are associated with adverse reproductive outcomes, yet the impact of the arcuate uterus remains unclear due to limited sample sizes and inconsistent findings in previous studies. We utilized a large population database to assess pregnancy, delivery, and neonatal outcomes in women with an arcuate uterus. Retrospective population-based study using data from the Health Care Cost and Utilization Project-Nationwide Inpatient Sample. Cases of arcuate uterus were identified using ICD code 752.36. Pregnancies in women with an arcuate uterus were matched to 3,016 pregnancies in women without congenital uterine anomalies (1 to 4) and compared to the entire population without congenital anomalies. Multivariate logistic regression adjusted for confounding variables. Among 3,841,147 control births and 754 births in women with an arcuate uterus, more of these women were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
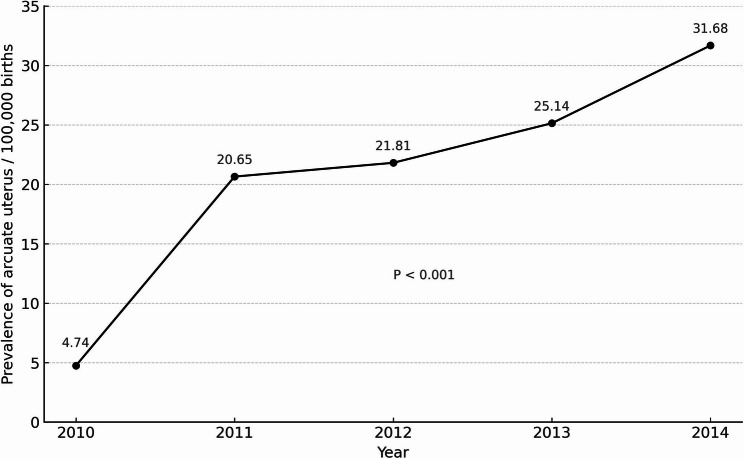 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGynecological conditions and treatments · Uterine Myomas and Treatments · Endometriosis Research and Treatment
Background
Congenital uterine anomalies (CUAs) affect about 5% of women and are linked to adverse health outcomes [1]. In non-pregnant women, CUAs can cause hematometra, hematocolpos, endometriosis, pelvic pain, abnormal uterine bleeding, and genital and urinary tract infections [2]. Additionally, 20–30% of individuals with Müllerian anomalies present with renal anomalies and other malformations, including cardiac defects [3–5].
In pregnant women, CUAs increase the risk of first and second-trimester miscarriages, preterm delivery, malpresentation, cesarean section (CS), and small for gestational age (SGA) neonates [6, 7]. Women with infertility also show higher rates of uterine malformations [8]. These adverse outcomes are primarily associated with uterus didelphys, bicornuate uterus, and septate uterus [3].
The arcuate uterus, a common CUA, is characterized by a slight indentation of less than a centimeter at the fundus with an angle above 90 degrees [9]. Most women with an arcuate uterus are asymptomatic, often diagnosed incidentally during ultrasonography [10]. Compared to other CUAs, the arcuate uterus appears to have fewer adverse effects on pregnancies. For instance, Woelfer et al. reported a slight increase in second-trimester pregnancy losses and preterm labor among women with an arcuate uterus [11], while Mucowski et al. found no significant impact on reproductive outcomes in a smaller study [12].
Most literature focuses on more significant uterine anomalies such as bicornuate or unicornuate uteri since arcuate uterus is often considered a variation of normal [12] or combines all CUAs. Studies specifically examining the effects of the arcuate uterus on pregnancy outcomes involved only a small number of participants, potentially lacking the power to detect significant differences. The largest study on this topic examined 420 cases of arcuate uterus and small septum combined [13]. Additionally, findings in the literature are conflicting. This study aims to clarify the pregnancy, delivery, and neonatal outcomes of women with an arcuate uterus using a large population database.
Methods
Data source
We conducted a retrospective population-based cohort study using data from the Health Care Cost and Utilization Project-Nationwide Inpatient Sample (HCUP-NIS) from 2010 to 2014. The HCUP-NIS database contains data on hospital inpatient stays and represents the largest publicly available all-payer inpatient database in the United States, covering over 97% of inpatient discharges from U.S. community hospitals. Data collection is managed by federal and state agencies, hospital associations, and private organizations. Data elements before 2015 are coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
Study population
In-hospital births occurring between 2010 and 2014 were included in the study. Births were identified using ICD-9-CM diagnostic codes (634x-679x, V22x, V23x, V27x) and procedural codes (72x-75x). Each pregnancy was included only once. In-hospital admissions resulting in delivery or maternal death were identified using specific ICD-9-CM codes (650x, 677x, 651x-676x) and procedural codes (72x, 73x, 74.0, 74.1, 74.2, 74.4, 74.99). Women with an arcuate uterus were identified using ICD-9-CM diagnostic code 752.36. Women without uterine anomalies served as the control group.
Data collection
Baseline characteristics recorded included age, race, type of insurance, income, body mass index (BMI) (obese BMI ≥ 30 kg/m² versus non-obese BMI < 30 kg/m²), previous CS, smoking history, pre-existing hypertension, diabetes, thyroid disease, drug use, HIV status, use of in in vitro fertilization (IVF), and presence of multiple gestation.
Pregnancy outcomes assessed included pregnancy-induced hypertension (PIH), chronic hypertension with superimposed preeclampsia, gestational hypertension, preeclampsia, eclampsia, gestational diabetes, and placenta previa. In the ICD-9-CM system, PIH was recorded as a composite category reflecting older terminology, which encompassed hypertensive disorders such as gestational hypertension, preeclampsia, and eclampsia. These outcomes were also analyzed separately when specifically coded.
Delivery outcomes included preterm premature rupture of membranes (PPROM), preterm delivery, placental abruption, chorioamnionitis, mode of delivery (operative vaginal delivery, CS, spontaneous vaginal delivery (SVD)), hysterectomy, postpartum hemorrhage (PPH), wound complications, maternal death, blood transfusion, maternal infection, venous thromboembolism (VTE), and disseminated intravascular coagulopathy (DIC). Deep vein thrombosis (DVT) and pulmonary embolism (PE) were included under VTE. Neonatal outcomes included SGA, intrauterine fetal demise, and congenital anomalies.
Statistical analysis
An unmatched and a matched analysis were performed. Each case of arcuate uterus was matched to four controls based on age, race, income, and insurance type. Statistically significant differences in baseline characteristics between women with and without an arcuate uterus were compared using Chi-Squared or Fisher’s exact tests. Maternal and neonatal outcomes were compared using univariate and multivariate logistic regression analyses adjusted for confounding variables (characteristics with p < 0.05). Analyses were conducted using SPSS 23.0 software. Statistical significance was set at p < 0.05.
Results
A total of 3,851,029 births occurred during the study period, including 754 from women with an arcuate uterus and 3,840,147 from women without CUAs (control group). Additionally, 10,128 births from women with other CUAs were excluded. The 754 births from women with an arcuate uterus were matched to 3,016 control births. The prevalence of arcuate uterus between 2010 and 2014 was 19.58 per 100,000 births, with a significant increase over time from 4.74 per 100,000 in 2010 to 31.68 per 100,000 in 2014 (p < 0.001) (Fig. 1).
Fig. 1. Prevalence of arcuate uterus among the 3,840,901 births that occurred between 2010 and 2014
Baseline characteristics
Women with an arcuate uterus were more likely to be older than 25 years, Caucasian, in a higher income quartile, and have private insurance compared to the control group (all p < 0.001) (Table 1). They were also more likely to have had a previous CS (p < 0.001), pre-gestational diabetes (p = 0.03), thyroid disease (p < 0.001), IVF pregnancies (p < 0.01), and multiple gestations (p < 0.01). In the matched group, women with an arcuate uterus were more likely to have had a previous CS (p < 0.001) and thyroid disease (p = 0.02).
Table 1. Maternal characteristics of the 3,840,901 births that occurred between 2004 to 2014CharacteristicsArcuate UterusN = 754No Arcuate UterusN = 3,840,147p-valueAge (years)< 0.001 < 25182 (24.1%)1,379,779 (35.8%) 25–34443 (58.7%)1,894,732 (49.3%) ≥ 35128 (17.0%)572,637 (14.9%)Race< 0.001 White534 (70.8%)2,036,437 (53.0%) Black29 (3.8%)560,659 (14.6%) Hispanic117 (15.5%)825,628 (21.5%) Asian and Pacific42 (5.6%)20,736 (5.4%) Native American5 (0.7%30,721 (0.8%) Other28 (3.7%)184,327 (4.8%)Income quartiles< 0.001 Less than 39,000118 (15.6%)1,063,521 (27.7%) 48,000–62,999224 (29.7%)967,705 (25.2%) $63,000 or more245 (32.5%)848,589 (22.1%)Plan type< 0.001 Medicare8 (1.1%)26,881 (0.7%) Medicaid191 (25.3%)1,686,081 (43.9%) Private including Health Maintenance Organizations511 (67.8%)1,911,655 (49.8%) Self-pay18 (2.4%)99,844 (2.6%) No charge0 (0.0%)3840 (0.1%) Other26 (3.4%)111,364 (2.9%)Obesity46 (6.1%)211,207 (5.5%)0.50Previous cesarean section194 (25.7%)656,486 (17.1%)< 0.001Smoking during pregnancy41 (5.4%)211,207 (5.5%)0.98Chronic hypertension16 (2.1%)84,483 (2.2%)0.93Pregestational diabetes13 (1.7%)38,401 (1.0%)0.03Drug use14 (1.9%)61,442 (1.6%)0.64Thyroid disease48 (6.4%)119,045 (3.1%)< 0.001HIV0 (0.0%)0 (0.0%)1.00In vitro fertilization6 (0.8%)7680 (0.2%)< 0.01Multiple gestation25 (3.3%)65,282 (1.7%)< 0.01HIV Human immunodeficiency virus
Pregnancy outcomes
Pregnancy outcomes in both matched and unmatched groups showed that women with an arcuate uterus had higher risks of PIH (adjusted odd ratio (aOR) 1.76, 95% CI 1.34–2.32 in the matched group; aOR 1.32, 95% CI 1.03–1.70 in the unmatched group) and preeclampsia (aOR 2.08, 95% CI 1.45–2.98 in the matched group; aOR 1.63, 95% CI 1.18–2.24 in the unmatched group) (Table 2). However, they were not at higher risk for gestational hypertension, eclampsia, chronic hypertension with superimposed preeclampsia, gestational diabetes, or placenta previa.
Table 2. Pregnancy, delivery and other outcomes in women with an arcuate uterus compared to matched controlsOutcomesArcuate uterusn = 754No Arcuate Uterusn = 3,840,147Crude Odds Ratio (95% Confidence Interval)Adjusted Odds Ratio (95% Confidence Interval)Adjustedp-valuePregnancy outcomes^†^ Pregnancy induced HTN82 (10.9%)307,212 (8.0%)1.40 (1.11–1.76)1.32 (1.03–1.70)0.03 Gestational HTN30 (4.0%)141,085 (3.7%)1.09 (0.76–1.58)1.02 (0.70–1.51)0.92 Preeclampsia48 (6.4%)145,925 (3.8%)1.72 (1.29–2.31)1.63 (1.18–2.24)< 0.01 Eclampsia1 (0.1%)3840 (0.1%)1.94 (0.27–13.8)2.55 (0.36–18.12)0.35 Preeclampsia and Eclampsia superimposed HTN6 (0.8%)23,041 (0.6%)1.25 (0.56–2.80)1.22 (0.51–2.96)0.66 GDM57 (7.6%)249,609 (6.5%)1.18 (0.90–1.55)1.07 (0.80–1.43)0.66 Placenta previa6 (0.8%)23,041 (0.6%)1.40 (0.63–3.12)1.11 (0.46–2.69)0.81Delivery outcomes^‡^ PPROM25 (3.3%)42,242 (1.1%)2.96 (1.99–4.41)2.86 (1.86–4.40)< 0.001 Preterm delivery90 (11.9%)253,448 (6.6%)1.92 (1.54–2.40)1.86 (1.45–2.37)< 0.001 Abruptio placenta22 (2.9%)42,242 (1.1%)2.81 (1.84–4.29)3.08 (1.99–4.77)< 0.001 Chorioamnionitis16 (2.1%)72,963 (1.9%)1.11 (0.67–1.81)1.21 (0.71–2.06)0.48 Operative vaginal delivery16 (1.2%)180,285 (4.7%)0.25 (0.13–0.47)0.26 (0.13–0.52)< 0.001 Cesarean section612 (81.2%)1,255,948 (32.7%)8.82 (7.35–10.59)10.88 (8.90–13.30)< 0.001 Spontaneous vaginal delivery133 (17.6%)2,395,092 (62.4%)0.13 (0.11–0.16)0.12 (0.10–0.14)< 0.001 Hysterectomy0 (0.0%)3840 (0.1%)--- PPH32 (4.2%)115,204 (3.0%)1.42 (0.99–2.02)1.43 (0.99–2.08)0.06 Wound complications7 (0.9%)11,520 (0.3%)2.81 (1.34–5.92)2.14 (0.95–4.78)0.07 Maternal death0 (0.0%)0 (0.0%)--- Transfusion14 (1.9%)46,082 (1.2%)1.56 (0.92–2.65)1.50 (0.84–2.66)0.17Others Maternal infection18 (2.4%)88,323 (2.3%)1.05 (0.66–1.68)1.18 (0.72–1.94)0.52 DVT0 (0.0%)0 (0.0%)--- Pulmonary embolism2 (0.3%)0 (0.0%)13.58 (3.38–54.49)15.14 (3.76–60.91)< 0.001 VTE2 (0.3%)3840 (0.1%)4.61 (1.15–18.50)4.81 (1.20–19.30)0.03 DIC4 (0.5%)7680 (0.2%)2.17 (0.81–5.80)2.19 (0.82–5.88)0.12HTN hypertension, GDM gestational diabetes mellitus, PPROM premature rupture of membranes, PPH post-partum hemorrhage, DVT deep vein thrombosis, VTE venous thromboembolism, DIC disseminated intravascular coagulation^†^ Pregnancy outcomes: Adjusted for Age, Race, Plan types, Income quartiles, Previous cesarean section, Thyroid disease, Multiple gestation, Pregestational diabetes and IVF^‡^ Delivery outcomes: Adjusted for Age, Race, Plan types, Income quartiles, Previous cesarean section, Thyroid disease, Multiple gestation, Pregestational diabetes, IVF, Pregnancy induce hypertension and Preeclampsia
Delivery outcomes
Women with an arcuate uterus were more likely to experience PPROM (aOR 2.46, 95% CI 1.48–4.09 in the matched group; aOR 2.86, 95% CI 1.86–4.40 in the unmatched group), preterm delivery (aOR 2.74, 95% CI 2.06–3.65 in the matched group; aOR 1.86, 95% CI 1.45–2.37 in the unmatched group), and placental abruption (aOR 2.11, 95% CI 1.23–3.63 in the matched group; aOR 3.08, 95% CI 1.99–4.77 in the unmatched group) (Table 2). They also had significantly higher odds of delivering via CS (aOR 30.04, 95% CI 23.99–37.63 in the matched group; aOR 10.88, 95% CI 8.90–13.30 in the unmatched group) and were much less likely to have a spontaneous vaginal delivery (SVD) (aOR 0.04, 95% CI 0.03–0.05 in the matched group; aOR 0.12, 95% CI 0.10–0.14 in the unmatched group).
In the matched cohort, women with an arcuate uterus had higher odds of PPH (aOR 1.67, 95% CI 1.09–2.56), wound complications (aOR 3.42, 95% CI 1.18–9.96), and DIC (aOR 5.58, 95% CI 1.21–25.60). In the unmatched group, they had higher odds of VTE (aOR 4.81, 95% CI 1.20–19.30) PE (aOR 15.14, 95% CI 3.76–60.91). No maternal deaths were reported in either group, and no significant differences were found in other reported outcomes.
Neonatal outcomes
Deliveries from women with an arcuate uterus had a 5.7% rate of SGA neonates compared to 3.2% in the matched control group (aOR 1.76, 95% CI 1.21–2.56) and 2.6% in the unmatched control group (aOR 2.21, 95% CI 1.58–3.10) (Table 3). Rates of intrauterine fetal demise and congenital anomalies were similar between the groups in both the matched and unmatched cohorts.
Table 3. Neonatal outcomes in women with an arcuate uterus compared to matched controlsOutcomes^†^Arcuate uterus N = 754No Arcuate Uterus N = 3,840,147Crude Odds Ratio (95% Confidence Interval)Adjusted Odds Ratio (95% Confidence Interval)Adjusted p-valueSmall for gestational age43 (5.7%)99,844 (2.6%)2.30 (1.69–3.13)2.21 (1.58–3.10)< 0.001Intra uterine fetal demise5 (0.7%)15,361 (0.4%)1.59 (0.66–3.83)1.97 (0.82–4.75)0.13Congenital anomalies0 (0.0%)11,520 (0.3%)---^†^Neonatal outcomes: Adjusted for Age, Race, Plan type, Income quartiles, Previous cesarean section, Thyroid Disease, Multiple gestation, Pregestational diabetes, IVF, Pregnancy induced hypertension and Preeclampsia
Discussion
This large-scale, population-based study is the first to evaluate the impact of an arcuate uterus on obstetrical and neonatal outcomes using a substantial cohort. Our findings indicate that women with an arcuate uterus have higher risks of several complications, including PIH, preeclampsia, preterm delivery, PPROM, placental abruption, CS, PPH, and wound complications. Despite these increased risks, rates of intrauterine fetal demise and congenital anomalies were similar between women with and without an arcuate uterus. Additionally, deliveries in women with an arcuate uterus showed higher odds of SGA neonates.
The arcuate uterus is one of the most common CUAs. The reported prevalence varies depending on the population studied and the mode of diagnosis. In a systematic review, Chan et al. demonstrated a prevalence of 3.9% of arcuate uterus in an unselected population [1]. In studies estimating the prevalence of CUAs in women with fertility issues, the arcuate uterus was found in 12–16% of that specific population [14–16]. Our results demonstrate a prevalence of an arcuate uterus of 19.58 per 100,000 births between 2010 and 2014. This prevalence is substantially lower than that reported in clinical studies, which likely reflects the limited sensitivity of ICD-9-CM coding in capturing this anomaly. Because coding is applied only when a definitive diagnosis is documented, the specificity is high, but many cases are likely missed, resulting in underestimation. Importantly, the dramatic six-fold increase in prevalence observed over the study years cannot be attributed to any change in ICD-9-CM diagnostic coding, which remained constant during this period. Instead, this rise most likely reflects improved recognition, documentation, and diagnostic imaging practices. Taken together, these factors suggest that our estimates may underestimate the true prevalence and risks associated with arcuate uterus in pregnancy.
Women with an arcuate uterus had a higher incidence of hypertensive disorders of pregnancy (including pregnancy-induced hypertension and preeclampsia). Not many studies have specifically looked at this outcome in CUAs. Fox et al. described the possibility of unilateral placental implantation and functional exclusion of one of the uterine arteries as potential causes for increased rates of intrauterine growth restriction and preeclampsia in women with major uterine anomalies. In their study, the arcuate uterus did not seem to be associated with increased preeclampsia; however, they had only 14 cases with the malformation, which might not have provided enough power to detect the risk of preeclampsia [6]. It is thus unclear if the arcuate uterus could also lead to abnormal placentation and possible hypertensive disorders during pregnancy.
As demonstrated by others, the arcuate uterus was also associated with thirty times the rates of CS delivery and lower rates of spontaneous vaginal delivery. This could be explained by the fact that malpresentations and placental abruption are more common [17, 18]. Thus, it is not surprising that these women were more likely to have had CS in the past. Higher rates of CS and the associated coagulopathy, as well as the possible higher risk of hypertensive disorders in pregnancy, could directly explain why women with an arcuate uterus had a higher risk of postpartum hemorrhage and five times more DIC. This increase in the risk of postpartum hemorrhage and DIC was only found in the matched cohort. In the unmatched cohort, women with an arcuate uterus had twelve times more PE and five times more deep vein thrombosis events. This difference was not found once the cases were matched to controls. The increased risk of DIC noted in our results might not, however, be significant, as only a very small number of women suffered from these outcomes. It is unlikely that the arcuate uterus itself would cause an increased risk of coagulability.
In our study, women with an arcuate uterus demonstrated about twice the risk for PPROM, preterm delivery, and SGA. Most of the published literature recognizes these risks with CUAs as a whole but not necessarily with the arcuate uterus [13, 19, 20]. Lekovich et al. suggested placental malperfusion as a possible cause of preterm delivery in women with uterine anomalies. Placental malperfusion is also a recognized cause of small neonates [18]. Woelfer et al. and Fox et al. found that women with an arcuate uterus had higher rates of second-trimester miscarriage and preterm delivery compared to those with a normal uterus. Their respective study populations included 72 and 14 women with the anomaly [6, 11]. However, a systematic review of 12 articles looking partly at the outcomes of the arcuate uterus did not find any of these differences, although the relative risk was marginally insignificant at 2.04 (95% CI 0.99 to 4.1) [21]. Our larger cohort might have provided sufficient power to confirm that the arcuate uterus is indeed associated with risks of PPROM, preterm delivery, and SGA.
Whether metroplasty of the arcuate uterus improves pregnancy outcomes is controversial. One prospective study of 96 women with arcuate and septate uteri found no difference in outcomes [22]. Conversely, a larger retrospective study of 420 small septums and arcuate uteri reported a decrease in the rate of preterm birth from 34% before hysteroscopic resection to 7% after, and a decrease in the rate of extreme preterm birth from 13 to 3% [13].
A recent case-control study also looked at the pregnancy outcomes of 37 women with an arcuate uterus compared to 165 women with similar baseline characteristics and no congenital uterine anomalies. Similar to our study, their results showed that women with an arcuate uterus were at increased risk of spontaneous preterm birth and had lower mean birthweight. However, there were no differences in the risks of preeclampsia or CS [23].
The study has several limitations. First, its retrospective design and reliance on ICD-9-CM coding for identifying cases may have introduced classification bias. In particular, some women with a low-level septate uterus may have been misclassified as having an arcuate uterus. Second, the database lacks detailed clinical data on the method of diagnosis, parity, fertility history, previous pregnancy losses, indications for CS, history of coagulopathies, and prior adverse outcomes. The absence of these variables may confound our findings and limits our ability to determine causality. Third, the relatively low prevalence of arcuate uterus identified in the database likely reflects under-detection, which would tend to underestimate rather than exaggerate the risks associated with this anomaly. Taken together, these factors highlight that our results should be interpreted with caution and viewed as hypothesis-generating rather than definitive.
The strengths of this study include its large cohort size, making it the most extensive study to date examining pregnancy, delivery, and neonatal outcomes associated with the arcuate uterus. The study design involved matching cases of arcuate uterus to controls, and we adjusted for confounding variables using multivariate logistic regression analysis. This robust methodology enhances confidence in our findings despite the heterogeneity in the existing literature.
Additionally, even if some subjects had low-level septate uteri rather than truly arcuate uteri, the results likely reflect the complications in the population diagnosed with arcuate uteri. We expect the rate of misdiagnosis to be consistent between our study and the general population, thereby supporting the generalizability of our findings. Consequently, our results provide valuable insights that can guide practitioners in understanding and managing the pregnancy risks associated with an arcuate uterus.
Conclusions
Women with an arcuate uterus appear to be at increased risk for several adverse pregnancy outcomes, including hypertensive disorders of pregnancy (pregnancy-induced hypertension and preeclampsia), PPROM, preterm delivery, placental abruption, CS, PPH, DIC, SGA neonates, and wound complications. These findings highlight the need for careful monitoring of this population. However, given the limitations of our data, the associations we observed should be interpreted with caution. Further large-scale prospective studies are warranted to confirm these findings and to guide evidence-based interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.