Delayed Diagnosis of Non-Bacterial Thrombotic Endocarditis in a Patient With Metastatic Lung Cancer
Efe Opone, Reza Aghamohammadzadeh

TL;DR
A patient with metastatic lung cancer was diagnosed with non-bacterial thrombotic endocarditis after experiencing embolic events, highlighting the need for early recognition in cancer patients.
Contribution
This case emphasizes the diagnostic challenges and clinical importance of NBTE in cancer patients with embolic events.
Findings
NBTE was diagnosed in a patient with metastatic lung cancer following embolic events and sterile vegetations.
The patient's poor prognosis was attributed to advanced malignancy and systemic embolization.
Prompt recognition of NBTE may reduce embolic risks, but outcomes remain poor in cancer-associated cases.
Abstract
Non-bacterial thrombotic endocarditis (NBTE) is characterised by sterile vegetations on cardiac valves and is most frequently associated with malignancy or chronic inflammatory disorders. Diagnosis is challenging, as clinical signs typically manifest after embolic complications. We report the case of a 42-year-old man with a history of myocardial infarction and lacunar stroke earlier in the year, who presented with chronic cough, progressive dyspnoea, and fatigue. On admission, he was tachycardic and tachypneic, with a diastolic murmur and bibasal crackles. Laboratory tests revealed normocytic anaemia and thrombocytopenia. Computed tomography pulmonary angiogram (CTPA) excluded pulmonary embolism but demonstrated a large pericardial effusion, confirmed on transthoracic echocardiography, along with severe aortic regurgitation and a mobile echodensity on the aortic valve suspicious for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
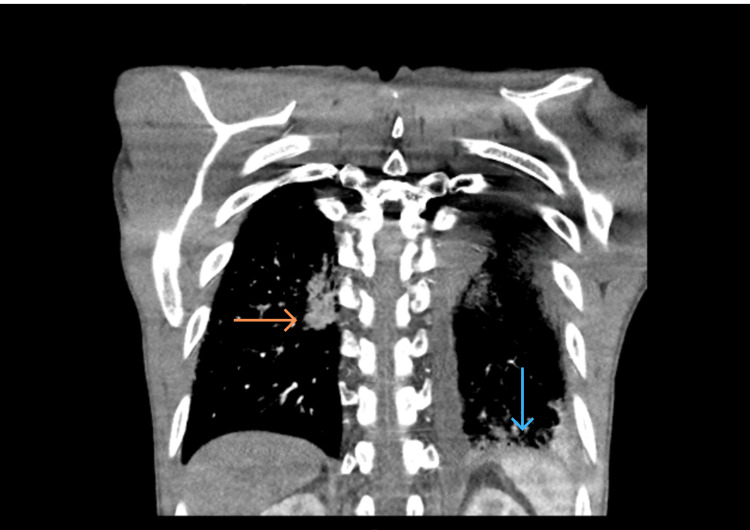 Figure 1
Figure 1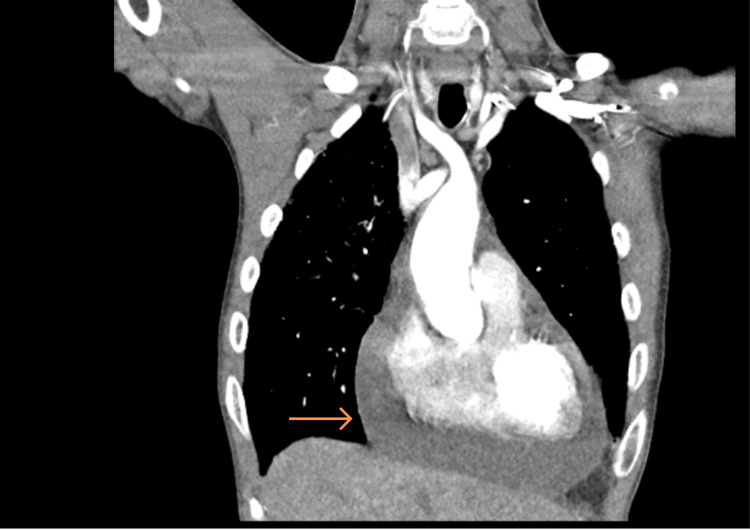 Figure 2
Figure 2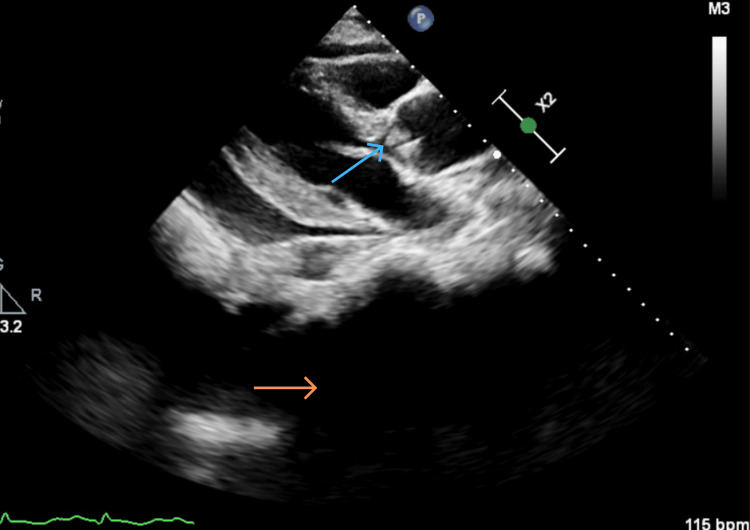 Figure 3
Figure 3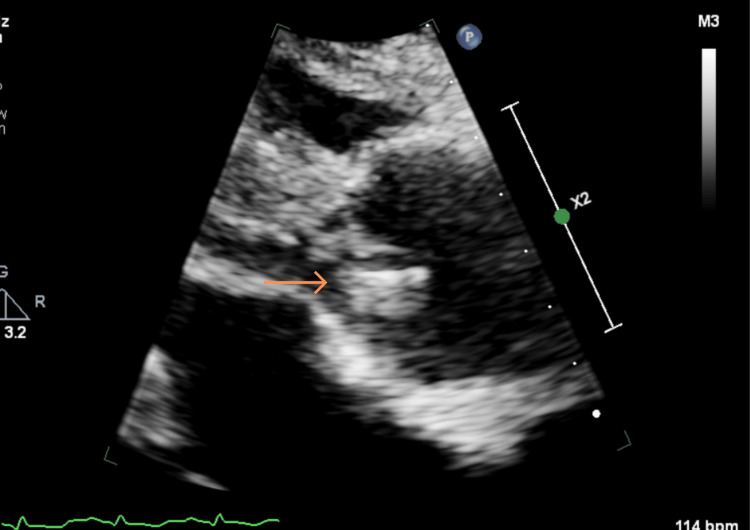 Figure 4
Figure 4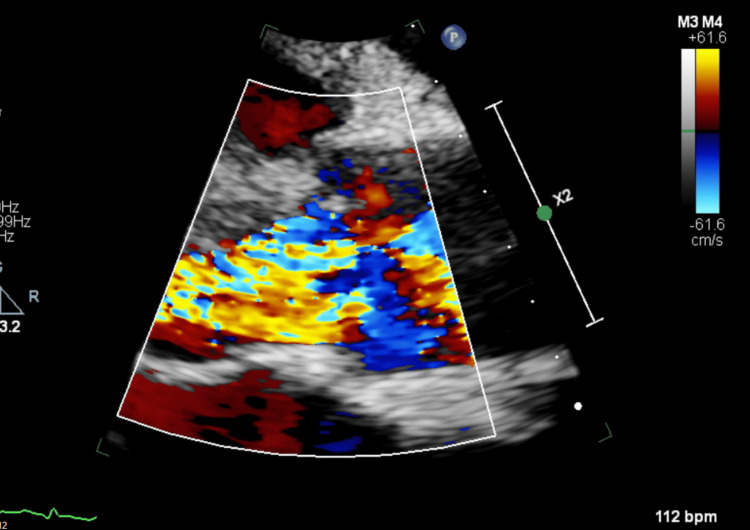 Figure 5
Figure 5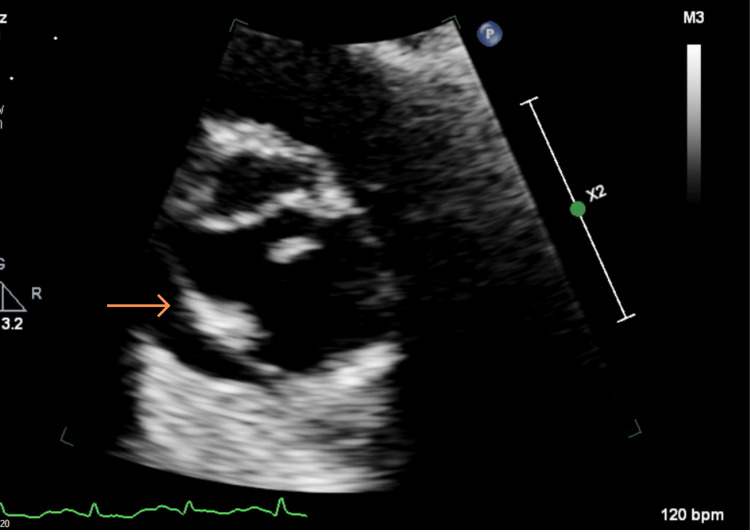 Figure 6
Figure 6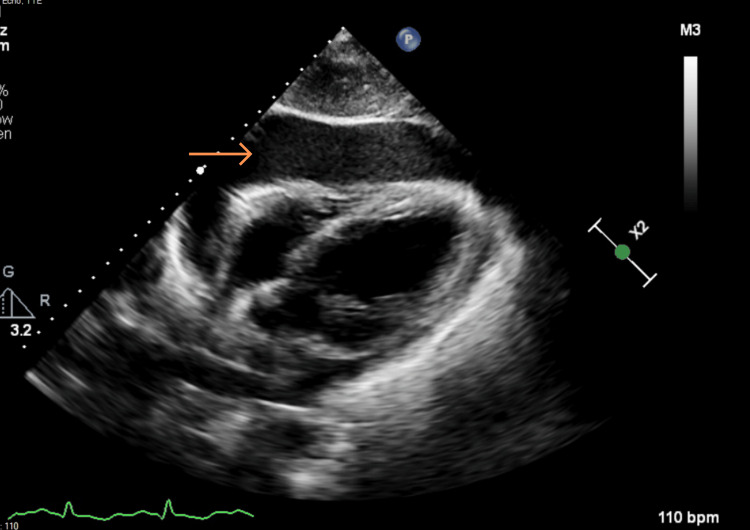 Figure 7
Figure 7| Day 1 | Day 2 | Reference range | Units | |
| Hb | 56 | 64 | 130-180 | g/L |
| WCC | 10.4 | 9.9 | 3.6 - 11.0 | x10^9/L |
| Platelets | 76 | 70 | 140 - 400 | x10^9/L |
| MCV | 94 | 95 | 80 - 100 | fL |
| Neutrophils | 8 | 6.4 | 1.8 - 7.5 | x10^9/L |
| INR | 1.5 | 1.3 | 0.8-1.2 | - |
| Fibrinogen | 0.9 | - | 1.5-4.5 | g/L |
| Sodium | 136 | 134 | 133 - 146 | mmol/L |
| Potassium | 4.4 | 4.1 | 3.5-5 | mmol/L |
| eGFR | >90 | >90 | >90 | mL/min/1.73m² |
| CRP | 8 | 45 | 5 | mg/L |
| Troponin I | 306 | - | 0-34 | ng/L |
| D dimer | 3048 | - | 0-229 | Ng/mL |
| C3 | 1.5 | - | 0.8-1.9 | g/L |
| C4 | 0.36 | - | 0.2-0.5 | g/L |
| IgG Anticardiolipin Ab | 1.5 | - | 0-10 | GPL U/mL |
| IgM Anticardiolipin Ab | 3.1 | - | 0-10 | GPL U/mL |
| IgG B-2-glycoprotein-1 Ab | <0.8 | - | 0-10 | GPL U/mL |
| IgM B-2 glycoprotein-1 Ab | 8.1 | - | 0-10 | GPL U/mL |
| CTD screen | 0.1 | - | 0-1 | - |
| MPO Ab | <0.2 | - | 0-5 | IU/mL |
| PR3 Ab | <0.6 | - | 0-3 | IU/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Actinomycetales infections and treatment · Transplantation: Methods and Outcomes
Introduction
First described in 1888 by Zeigler and later named “marantic endocarditis” by Libman in 1923, non-bacterial thrombotic endocarditis (NBTE) is a form of non-infective thrombotic endocarditis characterised by sterile fibrin-platelet vegetations on cardiac valve leaflets [1]. It most commonly affects the mitral and aortic valves and is strongly associated with malignancy, particularly mucin-producing adenocarcinomas, and chronic inflammatory conditions such as systemic lupus erythematosus and antiphospholipid syndrome [2].
Although uncommon, NBTE is clinically important because it frequently presents with systemic embolic events rather than cardiac symptoms, often delaying diagnosis [3]. In a contemporary Cleveland Clinic registry spanning 20 years, stroke accounted for ≈60% of presentations, while acute coronary syndrome represented 7% [4]. A recent systematic review and meta-analysis of 450 patients reported that approximately 70% had embolic phenomena and that malignancy was associated with a sixfold increase in embolic risk and a significantly higher in-hospital mortality [5].
Antemortem diagnosis remains challenging despite advances in echocardiographic imaging, and there are currently no formal guidelines for investigation or management [6].
We report the case of a 42-year-old man with recurrent embolic events, pericardial effusion, and valvular regurgitation, ultimately diagnosed with NBTE secondary to metastatic lung adenocarcinoma. This case highlights the importance of maintaining a high index of suspicion for NBTE in patients with unexplained systemic embolisation and the value of multimodal imaging in establishing the diagnosis.
Case presentation
A 42-year-old man presented with chronic cough, progressive shortness of breath, and fatigue. He denied chest pain, weight loss, rashes, joint pain, or gastrointestinal/genitourinary symptoms but reported occasional night sweats. His history was significant for two vascular events earlier in the year, a lacunar stroke and a non-ST elevation myocardial infarction, raising concern for an underlying prothrombotic state. He had a family history of ischaemic heart disease and reported cannabis use and alcohol excess.
On admission, he was tachypneic with a respiratory rate of 24 breaths per minute, oxygen saturation 99% on air, blood pressure 131/90 mmHg, heart rate 127 beats/min, and temperature 35.6°C. He appeared pale, with digital clubbing. Cardiovascular examination revealed a grade 3 diastolic murmur along the left sternal border, and bilateral crackles were heard on chest auscultation. Laboratory investigations demonstrated normocytic anaemia, thrombocytopenia, and elevated urea (Table 1).
Given the anaemia, an oesophagogastroduodenoscopy was performed but revealed no evidence of upper gastrointestinal bleeding. In view of his marked tachypnoea, persistent sinus tachycardia, and previous thromboembolic events, a computed tomography pulmonary angiogram (CTPA) was requested to exclude pulmonary embolism as a potentially reversible cause of his acute deterioration. The study demonstrated no filling defects within the pulmonary arteries but revealed a moderate-to-large pericardial effusion, a small left pleural effusion, and interstitial thickening in the right lung lobes (Figures 1, 2). Transthoracic echocardiography confirmed a large pericardial effusion (2.8 cm anteriorly), severe aortic regurgitation, and a mobile echodensity attached to the left coronary cusp of the aortic valve, suspicious for vegetation (Figures 3-7).
CTPA coronal view – right subpleural nodular consolidation (orange arrow) and consolidative changes in the left lower lobe (blue arrow)CTPA: Computed tomography pulmonary angiogram
CTPA coronal view – moderate to gross volume pericardial effusion (orange arrow)CTPA: Computed tomography pulmonary angiogram
TTE PLAX view – pericardial effusion (orange arrow) and thick aortic valve (blue arrow)TTE: Transthoracic echocardiogram, PLAX: Parasternal long axis
TTE PLAX view – zoom in on the aortic valve (orange arrow)TTE: Transthoracic echocardiogram, PLAX: Parasternal long axis
TTE PLAX view - zoom in on the aortic valve with colour flow mapping showing the aortic regurgitationTTE: Transthoracic echocardiogram, PLAX: Parasternal long axis
TTE PSAX view - aortic valve and the possible vegetation structure (orange arrow)TTE: Transthoracic echocardiogram, PSAX: Parasternal short axis
TTE subcostal window - pericardial effusion (orange arrow)TTE: Transthoracic echocardiogram
Pericardiocentesis drained 940 mL of haemoserous fluid for cytology and culture. Additional CT imaging demonstrated peripheral wedge-shaped infarcts in both kidneys and two large splenic infarcts, consistent with systemic embolisation. Serial blood cultures remained negative, and serology for Brucella and Coxiella burnetii was also negative.
The case was discussed at a multidisciplinary cardiology meeting, and the patient was considered for aortic valve replacement pending transoesophageal echocardiography and preoperative assessment. Despite empirical antibiotic therapy, follow-up imaging demonstrated worsening interstitial lung changes and new infrarenal aortic stenosis.
Cytological analysis of the pericardial fluid subsequently confirmed metastatic adenocarcinoma of probable pulmonary origin. In view of the diagnosis of advanced malignancy, sterile vegetations on echocardiography, persistently negative blood cultures, and recurrent systemic emboli, a diagnosis of non-bacterial thrombotic endocarditis (NBTE) was favoured. In light of the poor overall prognosis, surgical intervention was deferred, and a palliative approach was adopted. The patient’s condition deteriorated rapidly, and he died several days after discharge.
Discussion
This case highlights the diagnostic challenge of NBTE when the presenting feature is recurrent systemic embolisation rather than cardiac symptoms. NBTE is an uncommon but clinically significant entity that most often affects the mitral and aortic valves [2,4-9]. Diagnosis is frequently delayed, and embolic events, particularly stroke, are the most common presenting manifestation [7]. A Cleveland Clinic registry reported that stroke accounted for approximately 60% of initial presentations, with acute coronary syndrome occurring in 7% [4].
The most comprehensive epidemiological summary to date comes from a recent systematic review and meta-analysis of 416 reports comprising 450 patients [5]. The median age at diagnosis was 48 years, closely mirroring the age of our patient. The female-to-male ratio was approximately 2:1. Embolic phenomena were observed in around 70% of cases, with stroke being the most frequent manifestation. Malignancy was the leading associated condition and was strongly linked to an increased risk of embolic complications (adjusted odds ratio ≈ 6.4 compared with non-malignant causes). In-hospital mortality was high overall (36%), rising to more than 50% in cancer-associated NBTE, again consistent with the poor prognosis seen in our case, where the patient deteriorated rapidly despite supportive management.
Rogers et al. conducted a seminal clinical and pathological study of 115 patients with cancer and NBTE identified at autopsy [8]. Forty-two of these patients had cerebral infarcts attributable to NBTE rather than to other vascular pathology. Carcinoma of the lung was the most common malignancy, accounting for 33% of cases, followed by tumours of the gastrointestinal tract and haematopoietic system, findings which closely align with the primary lung adenocarcinoma identified in our patient. Importantly, Rogers et al. also investigated the effects of anticoagulation and demonstrated a reduction in the number and size of cerebral infarcts in anticoagulated patients, supporting the use of anticoagulation as a key component of management where not contraindicated.
The pathophysiology of NBTE is rooted in a hypercoagulable state. Malignancy contributes through tumour cell expression of procoagulant factors (e.g., tissue factor), vascular compression by tumour masses, and a systemic pro-inflammatory response [2]. Chronic inflammatory conditions, including systemic lupus erythematosus, rheumatoid arthritis, and antiphospholipid syndrome, are also recognised triggers; in one surgical series, 60% of patients with NBTE had an immune-mediated disorder [9].
Historically, NBTE was diagnosed almost exclusively at post-mortem, but advances in cardiac imaging, particularly transoesophageal echocardiography, have facilitated antemortem recognition [6]. Despite this, diagnosis remains challenging, and there is no widely accepted guidance for investigation or treatment. Several authors have recently proposed diagnostic algorithms, but maintaining a high index of suspicion remains crucial. NBTE should be strongly considered in patients presenting with unexplained systemic embolisation, especially in the setting of malignancy or inflammatory disease. Our case exemplifies these principles: the combination of recurrent embolic events, sterile vegetations on echocardiography, negative blood cultures, and the subsequent discovery of metastatic adenocarcinoma was highly suggestive of NBTE and directed management towards palliative care rather than surgical intervention.
Conclusions
Nonbacterial thrombotic endocarditis (NBTE) remains a challenging and frequently under-recognised diagnosis because of its non-specific presentation and tendency to manifest only after systemic embolisation. Our case is noteworthy for several reasons: it involved a young man with no known cancer diagnosis at presentation, whose first two clinical manifestations were myocardial infarction and lacunar stroke, both unusual sentinel events for NBTE. In addition, the coexistence of severe aortic regurgitation, a large haemorrhagic pericardial effusion, and sterile vegetations is rarely reported together in the context of NBTE.
This case demonstrates that malignancy can present with multisystem thromboembolic disease mimicking infective endocarditis or autoimmune disorders and highlights the need for clinicians to maintain a high index of suspicion for NBTE when faced with unexplained embolic events, valve abnormalities, or recurrent vascular occlusion, even in the absence of confirmed infection. Early recognition, prompt echocardiography, and consideration of anticoagulation may reduce further embolic complications. Despite advances in imaging, there remains a paucity of formal diagnostic and management guidelines for NBTE, particularly in cancer-associated cases. Reporting rare presentations such as this contributes to a growing body of evidence that may ultimately inform future algorithms for earlier detection and treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Non-bacterial thrombotic endocarditis manifested by ventricular fibrillation in a patient with low grade ovarian carcinoma: case report and literature review Eur Heart J Case Rep Kuipers RS Berghuis MA Ogilvie AC 05202110.1093/ehjcr/ytab 120PMC 818366034109290 · doi ↗ · pubmed ↗
- 2Nonbacterial thrombotic endocarditis in cancer patients: pathogenesis, diagnosis, and treatment Oncologist el-Shami K Griffiths E Streiff M 5185231220071752223910.1634/theoncologist.12-5-518 · doi ↗ · pubmed ↗
- 3Systemic embolization due to non-bacterial thrombotic endocarditis: An autopsy case report and mini review of the literature SAGE Open Med Case Rep Tisch C Ernst D Falke M 205031312202410.1177/2050313 X 241229576 PMC 1082637438292877 · doi ↗ · pubmed ↗
- 4A contemporary 20-year Cleveland Clinic experience of nonbacterial thrombotic endocarditis: etiology, echocardiographic imaging, management, and outcomes Am J Med Zmaili MA Alzubi JM Kocyigit D 3613691342021 https://pubmed.ncbi.nlm.nih.gov/32827467/3282746710.1016/j.amjmed.2020.06.047 · doi ↗ · pubmed ↗
- 5Epidemiologic and clinical characteristics of marantic endocarditis: a systematic review and meta-analysis of 416 reports Curr Probl Cardiol Alhuarrat MA Garg V Borkowski P 1020274920243755794110.1016/j.cpcardiol.2023.102027 · doi ↗ · pubmed ↗
- 6Diagnostic work-up in patients with nonbacterial thrombotic endocarditis J Clin Med Tonutti A ScarfòI La Canna G 122023 https://doi.org/10.3390/jcm 1218581910.3390/jcm 12185819 PMC 1053202337762758 · doi ↗ · pubmed ↗
- 7Nonbacterial thrombotic endocarditis with bivalvular regurgitation CASE (Phila) Assaf SN Taylor J Assaf AN 168174720233732546010.1016/j.case.2023.02.004PMC 10264202 · doi ↗ · pubmed ↗
- 8Cerebral infarction from non-bacterial thrombotic endocarditis: clinical and pathological study including the effects of anticoagulation Am J Med Rogers LR Cho ES Kempin S Posner JB 198783 https://doi.org/10.1016/0002-9343(87)90908-910.1016/0002-9343(87)90908-93674060 · doi ↗ · pubmed ↗