Non-ketotic Hyperglycemic Hemichorea as a Clue to Undiagnosed Type 2 Diabetes Mellitus in an Elderly Man: A Case Report
Rafael Machado, Rita Marçal

TL;DR
An elderly man with undiagnosed type 2 diabetes showed rare neurological symptoms, highlighting the need for metabolic screening in primary care.
Contribution
This case report presents non-ketotic hyperglycemic hemichorea as an initial sign of undiagnosed diabetes in an elderly patient.
Findings
Non-ketotic hyperglycemic hemichorea was diagnosed in a 76-year-old man with severe hyperglycemia.
Neurological symptoms resolved after insulin treatment and glycemic optimization.
The case emphasizes the importance of metabolic screening for early diabetes detection.
Abstract
Non‑ketotic hyperglycemic hemichorea is a rare neurologic complication associated with poorly controlled and, in exceptional cases, previously undiagnosed type 2 diabetes, characterized by sudden unilateral choreiform movements and basal ganglia hyperdensity on CT or T1-hyperintensity on MRI. We report the case of a 76‑year‑old male without routine primary-care follow-up who presented to the emergency department after one week of left-arm choreo‑dystonic movements, accompanied by mild left-sided hemiparesis and hypoesthesia. Laboratory evaluation revealed severe hyperglycemia (381 mg/dl) and glycosuria but no ketonuria. Non-contrast brain CT identified a discrete hyperdensity in the right caudate and lentiform nucleus, with no additional findings to suggest hemorrhagic or ischemic stroke. A 6-unit intravenous bolus of regular human insulin normalized serum glucose and markedly reduced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
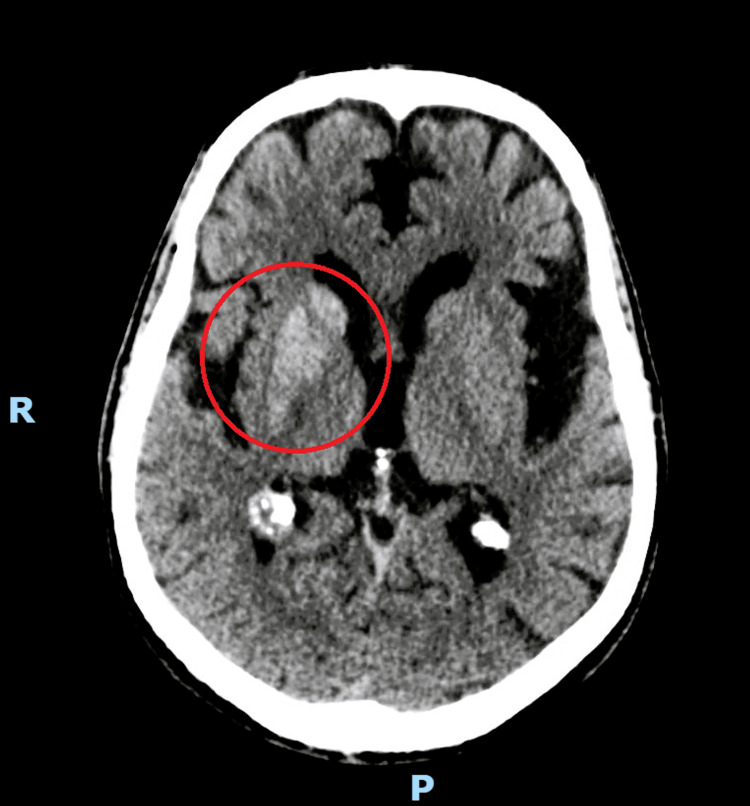 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Neurological disorders and treatments · Genetic Neurodegenerative Diseases
Introduction
Hemichorea is a hyperkinetic movement syndrome characterized by abrupt, involuntary, non-patterned, and purposeless movements affecting one side of the body [1,2]. This condition results from dysfunction of the contralateral basal ganglia, often caused by underlying structural lesions such as vascular insults, neoplasms, drug effects, autoimmune diseases, or metabolic disturbances [1,2].
Non-ketotic hyperglycemic hemichorea (NKH-HC) is a rare neurological complication of longstanding, poorly controlled, and, in exceptional cases, previously undiagnosed type 2 diabetes mellitus [3], with a reported prevalence of approximately one case per 100,000 individuals [4], affecting most commonly elderly women [2,5].
Clinically, NKH-HC is marked by an acute onset of unilateral involuntary choreiform movements of the limbs. Neuroimaging typically reveals distinctive findings in the contralateral basal ganglia, such as hyperdensity on CT or hyperintense signals on T1-weighted MRI, reflecting perfusion changes in these regions that have recently been termed “diabetic striatopathy” [1,6]. The most accepted pathogenic hypothesis suggests a shift toward anaerobic cerebral metabolism, leading to rapid depletion of gamma‑aminobutyric acid (GABA) and subsequent disinhibition of the subthalamic nucleus and basal ganglia. In non-ketotic states, the lack of ketone bodies prevents GABA resynthesis, worsening this imbalance [2,4,5]. Other pathological findings, such as microvascular hemorrhage and reactive astrocytosis, further suggest that vascular injury and gliosis may also contribute to the clinical and imaging features of the condition [2,4,5].
Recognizing these clinical and radiological hallmarks is essential because prompt correction of hyperglycemia typically leads to a rapid, often complete, symptom resolution, although recurrence has been reported in approximately 18 % of cases [4].
Case presentation
A 76-year-old man presented to the emergency department with continuous, abnormal, involuntary movements of the left arm that had persisted for one week. He denied headaches, dizziness, loss of consciousness, or dysarthria. Past medical history included hypertension and surgical drainage of a left traumatic subdural hematoma four years earlier, with no medical follow-up thereafter. He reported no regular primary care visits for the past five years, with medication non-adherence during that period. He also reported no recent head trauma.
On examination, the patient was awake, alert, and fully oriented. Vital signs were within normal limits. Neurologic assessment revealed non-stereotyped choreic-dystonic movements of the left upper and lower limbs, accompanied by mild left-sided hemiparesis and hypoesthesia.
Initial blood and urinary tests revealed a serum glucose level of 381 mg/dL, glycosuria, and negative urinary ketone bodies. Complete blood count, corrected sodium, arterial blood gas test, electrolytes, and renal and hepatic panels were all within normal limits. Thyroid tests and HbA1c were not available in the emergency setting.
Non-contrast head CT showed a discrete focal hyperdensity involving the right caudate and lentiform nucleus (Figure 1), together with incipient signs of microangiopathic subcortical leukoencephalopathy and postoperative sequelae from the prior left frontal-parietal trepanation. There was no evidence of mass effect, midline shift, or extra-axial collections. The ventriculocisternal system was patent. MRI was not available in the emergency department. These findings were consistent with a probable diagnosis of non-ketotic hyperglycemic hemichorea.
Single axial non-contrast head CT shows a discrete hyperdensity involving the right caudate and lentiform nucleus, circled in redThis non-contrast head CT scan was performed with 3 mm slices parallel to the orbitomeatal plane.
The patient received a 6-unit bolus of human insulin (100 U/mL) followed by an isotonic saline infusion, guided by hydration status. Glucose levels were monitored every two hours. Six hours later, his serum glucose had reduced to 196 mg/dL, and the intensity of his neurological symptoms had markedly diminished. By the time of discharge from the emergency department, hemichorea had resolved completely. The patient was prescribed metformin 500 mg twice daily, and he was referred for outpatient endocrinology follow‑up.
Three days after discharge, at the endocrinology appointment, HbA1c was 14.2%, fasting plasma glucose 381 mg/dL, and thyroid panel within normal range. Insulin glargine was started at 18 units nightly. After one month, HbA1c decreased to 11.8%, insulin was maintained, and metformin was replaced with a fixed-dose combination of metformin/sitagliptin 850/50 mg twice daily. At seven months, HbA1c had normalized to 5.6% and no hypoglycemic episodes were reported. Insulin was discontinued, and the oral antidiabetic was increased to 1000/50 mg twice daily. The patient was discharged from the endocrinology care and enrolled for ongoing surveillance at his primary‑care health center. There was no report of neurologic signs.
Discussion
This case highlights NKH‑HC as an uncommon initial manifestation of undiagnosed diabetes, particularly in an elderly individual lacking regular medical care. The presentation in this patient is atypical, as most reported cases occur in elderly women with long-standing type 2 diabetes mellitus [2,5]. However, recent meta-analyses and case series suggest that the gender distribution may be more balanced than previously thought, and that NKH-HC can also be the first clinical sign of diabetes in previously undiagnosed individuals [4].
The main differential diagnoses for hemichorea include acute ischemic stroke, intracerebral hemorrhage, basal ganglia tumors, or metastases. In this patient, the characteristic CT hyperdensity localized to the basal ganglia, without mass effect, midline shift, or extra-axial collections, correlated with marked hyperglycemia, strongly supports NKH‑HC. Unlike structural lesions such as neoplastic or hemorrhagic processes, this imaging pattern is consistent with previous reports, which lack mass effect and often spares the internal capsule [2,7].
Most patients experience rapid symptom resolution following normalization of blood glucose levels, as seen in this case. However, recurrence is not uncommon, with rates reported up to 18% [4]. Factors contributing to recurrence may include poor glycemic control, delayed initial treatment, and underlying striatal atrophy in imaging, which may predispose the basal ganglia to dysfunction [7].
Treatment typically involves glycemic control, often with insulin, and recovery time was significantly shorter in patients treated with glucose control alone, suggesting that early intervention may prevent progression to more severe or persistent symptoms [4].
From a primary care perspective, this case underscores the importance of opportunistic diabetes screening, especially in elderly patients with limited healthcare access. Early detection and management of diabetes can substantially reduce complications such as NKH-HC and reduce the burden of disease. Strengthening primary care infrastructure, therefore, remains pivotal for routine monitoring, patient education, and early identification of medication non‑adherence or disease decompensation, ultimately improving long-term outcomes.
Conclusions
Hemichorea should prompt clinicians to assess hyperglycemia, especially in elderly patients without an established diagnosis of diabetes. Contralateral basal ganglia hyperdensity on CT together with hyperglycemia suggests NKH-HC. Timely glycemic correction usually resolves the movement disorder. This case also emphasizes the critical role of continuous healthcare engagement, as systematic diabetes screening in primary care is essential for early diagnosis and complication prevention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Seminar on choreas Lancet Neurol Cardoso F Seppi K Mair KJ Wenning GK Poewe W 589602520061678198910.1016/S 1474-4422(06)70494-X · doi ↗ · pubmed ↗
- 2Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T 1-weighted brain MRI study J Neurol Sci Oh S Lee K Im J Lee MS 576220020021212767710.1016/s 0022-510x(02)00133-8 · doi ↗ · pubmed ↗
- 3Hemiballism-hemichorea. Clinical and pharmacologic findings in 21 patients Arch Neurol Dewey RB Jr Jankovic J 862867461989275752610.1001/archneur.1989.00520440044020 · doi ↗ · pubmed ↗
- 4"Diabetic striatopathy": clinical presentations, controversy, pathogenesis, treatments, and outcomes Sci Rep Chua CB Sun CK Hsu CW Tai YC Liang CY Tsai IT 15941020203200590510.1038/s 41598-020-58555-w PMC 6994507 · doi ↗ · pubmed ↗
- 5Diabetic striatal disease: clinical presentation, neuroimaging, and pathology Intern Med Abe Y Yamamoto T Soeda T 113511414820091957144610.2169/internalmedicine.48.1996 · doi ↗ · pubmed ↗
- 6Hemiballism: revisiting a classic disorder Lancet Neurol Postuma RB Lang AE 661668220031457273410.1016/s 1474-4422(03)00554-4 · doi ↗ · pubmed ↗
- 7Recurrent hemichorea-hemiballism with non-ketotic hyperglycemia Neurol Sci Shin HW Park KY Youn YC 9339343520142456315010.1007/s 10072-014-1673-0 · doi ↗ · pubmed ↗