Renal Cortical Necrosis Secondary to Idiopathic Acute Pancreatitis in a Young Adult: A Case Report
Ram Prabahar M, Raniya Palliyedath, Jayanivash Jayam, Sathiyan Sivanandam, Uma Sirisha Pusapati

TL;DR
A young man with severe acute pancreatitis developed kidney failure due to renal cortical necrosis and now requires dialysis and a kidney transplant.
Contribution
This case report documents a rare instance of renal cortical necrosis caused by idiopathic acute pancreatitis in a young adult.
Findings
The patient developed dialysis-requiring acute kidney injury due to renal cortical necrosis following acute pancreatitis.
Despite interventions, the patient experienced repeated pancreatitis episodes and progressed to end-stage kidney disease.
Genetic testing did not identify a cause, and the pancreatitis was classified as idiopathic.
Abstract
Renal cortical necrosis (RCN) is a rare and severe form of acute kidney injury (AKI), often resulting in irreversible kidney failure. We present the case of a 25-year-old male who developed severe acute pancreatitis (AP), leading to dialysis-requiring AKI. Despite remission of the initial AP episode, he remained anuric and dialysis-dependent for four weeks. A renal biopsy revealed diffuse cortical necrosis. He was continued on maintenance hemodialysis via a right internal jugular vein (IJV) tunneled venous catheter. Eight weeks after the initial episode, he presented with acute abdominal pain. Follow-up imaging studies showed gallbladder sludge and signs of walled-off pancreatic necrosis; endoscopic and surgical procedures (endoscopic ultrasound (EUS)-guided cystogastrostomy and laparoscopic cholecystectomy) were performed. However, he experienced repeated episodes of AP over the next…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
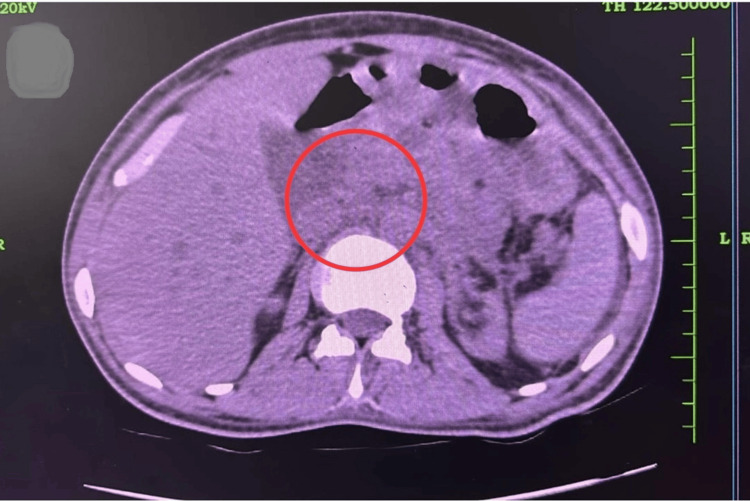 Figure 1
Figure 1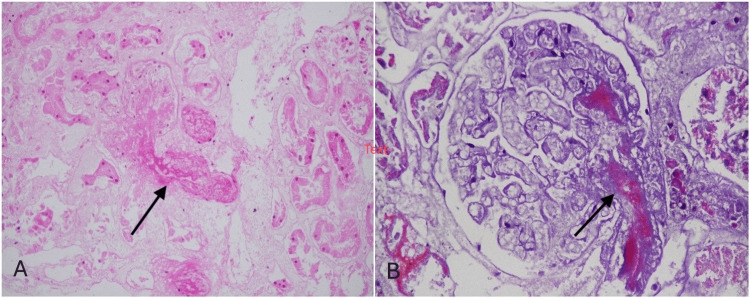 Figure 2
Figure 2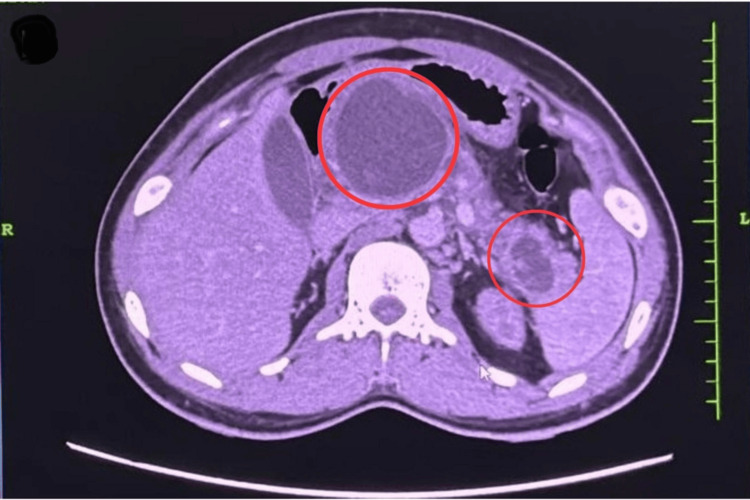 Figure 3
Figure 3| Parameter | Patient value | Reference range |
| Hemoglobin | 8.3 g/dL | 13-17 g/dL |
| PCV (Hematocrit) | 20.9% | 40%-50% |
| RBC count | 2.07 × 10⁶/µL | 4.5-5.9 × 10⁶/µL |
| MCV | 101 fL | 80-100 fL |
| Total WBC count | 17,090 /µL | 4,000-11,000 /µL |
| Neutrophils | 89% | 40%-75% |
| Lymphocytes | 16% | 20%-45% |
| Eosinophils | 3% | <6% |
| Absolute neutrophil count | 15,120/µL | 1,500-8,000/µL |
| Platelet count | 428,000/µL | 150,000-450,000/µL |
| Peripheral smear | No evidence of hemolysis; neutrophilia noted | - |
| Serum amylase | 1,200 U/L | 30-110 U/L |
| Serum lipase | 2,500 U/L | 0-160 U/L |
| C-reactive protein (CRP) | 160 mg/L | <10 mg/L |
| LDH | 220 U/L | 140-280 U/L |
| Total bilirubin | 4.03 mg/dL | 0.2-1.2 mg/dL |
| SGOT (AST) | 348 U/L | <40 U/L |
| SGPT (ALT) | 186 U/L | <40 U/L |
| Alkaline phosphatase | 135 U/L | 45-120 U/L |
| Serum creatinine | 14.49 mg/dL | 0.7-1.3 mg/dL |
| Blood urea | 129 mg/dL | 7-20 mg/dL |
| Sodium (Na⁺) | 139 mmol/L | 135-145 mmol/L |
| Potassium (K⁺) | 4.3 mmol/L | 3.5-5.0 mmol/L |
| Chloride (Cl⁻) | 104 mmol/L | 98-106 mmol/L |
| Calcium | 8.7 mg/dL | 8.5-10.5 mg/dL |
| Urine routine/microscopy | Clear, specific gravity 1.020, no protein, no RBCs, no casts | - |
| Complement levels | C3: 125 mg/dL; C4: 32 mg/dL | C3: 90-180; C4: 10-40 mg/dL |
| Serologies/immune markers | ANA, ANCA, dsDNA - Negative | - |
| ANA profile (Immunoblot) | Negative | - |
| Paraprotein workup | SPEP/UPEP - No M band | - |
| ADAMTS13 activity | 65% | >50% |
| Triglycerides | 175 mg/dL | 150-199 mg/dL |
| Total cholesterol | 79 mg/dL | <200 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Gallbladder and Bile Duct Disorders · Amoebic Infections and Treatments
Introduction
Acute pancreatitis (AP) is an inflammatory condition of the pancreas, typically presenting with acute abdominal pain. Disease severity is variable: mild AP is characterized by the absence of organ failure and local complications, moderate AP by transient organ failure resolving in less than 48 hours, and severe AP by persistent multi-organ failure [1]. Organ failure is commonly assessed using the modified Marshall scoring system, which evaluates the cardiovascular, respiratory, and renal systems. Acute kidney injury (AKI) complicates 9% to 12% of severe AP cases and is strongly associated with poor prognosis, particularly when kidney replacement therapy (KRT) is required. The need for KRT in AKI secondary to AP is variable, ranging from 26% to 63% in several series [2]. The pathophysiology is multifactorial, ranging from initial volume depletion to complex vascular and humoral factors. RCN is a rare subset of AKI, with a prevalence of 1.9% to 2% in developed countries compared with 6% to 7% in developing regions [3]. Although RCN is usually associated with obstetric catastrophes or sepsis, its occurrence in idiopathic AP is rarely documented, underscoring the clinical significance of this case.
Case presentation
A 25-year-old man with no prior comorbidities presented with severe epigastric pain radiating to the back, persistent vomiting, and oliguria. He denied smoking, alcohol, or substance use. He was hypovolemic with low-normal blood pressure on admission. Laboratory investigations revealed azotemia, anemia, markedly elevated amylase and lipase, and elevated C-reactive protein (CRP) (Table 1). Imaging showed an edematous pancreas with peri-pancreatic inflammation and normal-sized kidneys bilaterally, with minimal perinephric stranding (Figure 1). He developed severe third-space fluid collections, including ascites, bilateral pleural effusion, and pericardial effusion. He was admitted to the intensive care unit and managed conservatively with bowel rest, intravenous fluids, and total parenteral nutrition. Hemodialysis was initiated for AKI.
Computed tomography (CT) scan of the abdomen showing an edematous uncinate process and proximal pancreas with fat stranding.
Although the initial AP episode resolved, the patient remained anuric. He remained dialysis-dependent at three weeks, after which a renal biopsy was performed. The biopsy revealed diffuse cortical necrosis characterized by complete loss of viable cortical tissue, necrotic glomeruli, and fibrin thrombi occluding efferent arterioles and interlobular arteries (Figure 2). The first AP episode had a severe impact on the cardiovascular system, with the patient developing dilated cardiomyopathy and global hypokinesia. Due to a low ejection fraction (30%), he was continued on maintenance hemodialysis via a right internal jugular vein (IJV) tunneled venous catheter.
(A) Diffuse coagulative necrosis of renal cortical tissue with ghost-like glomeruli and tubules (hematoxylin and eosin (H&E) stain, 100×), and (B) glomerulus with fibrin thrombus occluding the efferent arteriole alongside necrotic surrounding tubules (H&E stain, 400×).
He was hospitalized with a second episode of AP eight weeks after the first. Follow-up imaging revealed gallbladder sludge and walled-off pancreatic necrosis (Figure 3). He underwent EUS-guided cystogastrostomy with placement of a 15-mm lumen-apposing metallic stent, followed by laparoscopic cholecystectomy. Both procedures were completed without complications. The biopsy specimen did not show gallstones or cholecystitis.
CT abdomen showing a well-defined, encapsulated fluid collection with heterogeneous internal contents, consistent with walled-off pancreatic necrosis (WOPN).
Over the subsequent 18 months, he experienced recurrent episodes of AP. During this period, he developed endocrine pancreatic insufficiency and type 3c diabetes mellitus (T3cDM). There were no clinical or laboratory features suggestive of thrombotic microangiopathy. Evaluation for recurrent AP, including serum triglycerides, calcium, IgG4, abdominal CT, and EUS-guided analysis, was unremarkable. Comprehensive genetic testing, including PRSS1 (serine protease 1, cationic trypsinogen), SPINK1 (serine peptidase inhibitor Kazal type 1), CFTR (cystic fibrosis transmembrane conductance regulator), and CTRC (chymotrypsin C), was negative, supporting the classification of AP as idiopathic. He remains dialysis-dependent and is currently awaiting deceased donor renal transplantation.
Discussion
Severe AP often leads to multi-organ failure and poor outcomes, with AKI being a well-recognized complication. AKI complicates 9% to 12% of AP cases and is associated with significantly increased mortality, with rates as high as 30% reported in one series [1,4]. The etiology of AKI is multifactorial, including hypovolemia, systemic inflammation, toxins from the necrotic pancreas, and abdominal compartment syndrome [5]. Renal recovery usually parallels the resolution of pancreatic inflammation, though 15% to 20% of patients progress to chronic kidney disease. Treatment is essentially supportive, with KRT required in severe cases. Our patient developed AKI during the first AP episode and progressed to end-stage kidney disease (ESKD).
RCN is a severe form of AKI, often resulting in irreversible renal failure. It is defined by total ischemic necrosis of all nephron elements. Diffuse forms lead to irreversible failure, while patchy forms may allow partial recovery. It typically results from ischemia due to reduced perfusion, intravascular coagulation, microvascular injury, or severe vasospasm. Etiologies are classified as obstetric or non-obstetric, with septic abortion and hemolytic uremic syndrome being the most common causes in each group. In developing countries, such as India, the incidence of RCN has declined over recent decades, largely due to reduced rates of unsafe abortions [6,7].
The pathogenic mechanism remains incompletely understood, though small-vessel vasospasm and toxin-induced endothelial injury are considered initiating events. While obstetric complications and sepsis are the predominant causes of RCN, its occurrence as a complication of AP remains exceptionally rare, with fewer than a dozen cases described. Most cases resulted in irreversible renal injury progressing to ESKD [8-10]. In addition to the usual pathogenic factors, vasoactive and cytotoxic substances released during AP are thought to contribute. In line with the systemic impact of severe AP, our patient also developed walled-off pancreatic necrosis requiring drainage and later developed chronic dilated cardiomyopathy with reduced ejection fraction.
Conclusions
Severe AP can cause significant multi-organ damage. This case highlights the rare occurrence of RCN secondary to AP in a young patient, leading to irreversible, dialysis-dependent ESKD. It underscores the importance of early recognition and vigilant management of renal complications in AP, as well as the need for long-term follow-up given the potential for recurrent episodes, chronic morbidity, and eventual renal transplantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Classification of acute pancreatitis: 2012 revision of the Atlanta classification and definitions by international consensus Gut Banks PA Bollen TL Dervenis C 1021116220132310021610.1136/gutjnl-2012-302779 · doi ↗ · pubmed ↗
- 2Acute kidney injury associated with acute pancreatitis Clin J Am Soc Nephrol Nassar TI Qunibi WY 11061115142019 https://doi.org/10.2215/CJN.131911183111820910.2215/CJN.13191118 PMC 6625613 · doi ↗ · pubmed ↗
- 3Changing picture of renal cortical necrosis in acute kidney injury in developing country World J Nephrol Prakash J Singh VP 48048642015 https://doi.org/10.5527/wjn.v 4.i 5.4802655818410.5527/wjn.v 4.i 5.480PMC 4635367 · doi ↗ · pubmed ↗
- 4Acute pancreatitis-related acute kidney injury: a southern Indian single center experience Kidney Int Rep Selvanathan D Nandhakumar A Jeswanth S 2152020
- 5The pathogenic mechanism of severe acute pancreatitis complicated with renal injury: a review of current knowledge Dig Dis Sci Zhang XP Wang L Zhou YF 297306532008 https://doi.org/10.1007/s 10620-007-9866-51759741110.1007/s 10620-007-9866-5 · doi ↗ · pubmed ↗
- 6Acute renal cortical necrosis--a study of 113 patients Ren Fail Chugh KS Jha V Sakhuja V Joshi K 3747161994 https://doi.org/10.3109/08860229409044846818414510.3109/08860229409044846 · doi ↗ · pubmed ↗
- 7Decreasing incidence of renal cortical necrosis in patients with acute renal failure in developing countries: a single-centre experience of 22 years from Eastern India Nephrol Dial Transplant Prakash J Vohra R Wani IA 12131217222007 https://doi.org/10.1093/ndt/gfl 7611726753910.1093/ndt/gfl 761 · doi ↗ · pubmed ↗
- 8Acute renal cortical necrosis in a series of young men with severe acute pancreatitis Clin Nephrol Alfonzo AV Fox JG Imrie CW Roditi G Young B 223231662006 https://doi.org/10.5414/cnp 662231706398810.5414/cnp 66223 · doi ↗ · pubmed ↗