Left Upper Lobe Lung Cancer With Swyer-James-MacLeod Syndrome
Motoka Omata, Shota Mitsuboshi, Hiroaki Shidei, Akira Ogihara, Hiroe Aoshima, Tamami Isaka, Takako Matsumoto, Masato Kanzaki

TL;DR
This paper reports a rare case of lung cancer in a patient with Swyer-James-MacLeod syndrome, a condition affecting lung development.
Contribution
The novelty lies in presenting a rare co-occurrence of lung cancer and SJMS in an adult, with a detailed surgical approach.
Findings
SJMS is extremely rare in adults and even rarer when associated with lung cancer.
A robot-assisted thoracoscopic left pneumonectomy was successfully performed for the case.
This case highlights the importance of considering SJMS in lung cancer diagnosis.
Abstract
Swyer-James-MacLeod syndrome (SJMS) is characterized by unilateral hyperlucency of the lung on chest roentgenogram, unilateral reduction in vascularity on chest computed tomography, and unilateral loss of perfusion on pulmonary ventilation/perfusion scan. The prevalence of SJMS is reported to be 0.01%, with most cases occurring in children and only a few cases in adults. Therefore, SJMS associated with primary lung cancer is extremely rare. We present a case of left upper lobe lung cancer with SJMS by performing robot-assisted thoracoscopic left pneumonectomy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
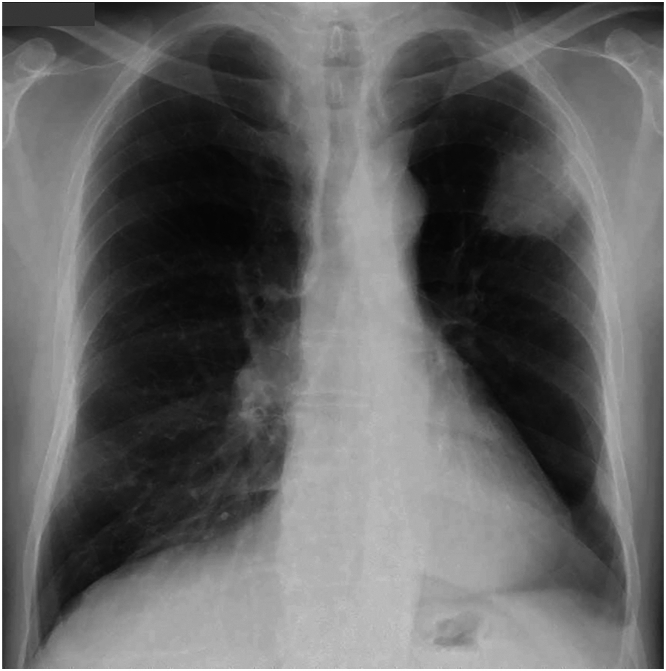 Figure 1
Figure 1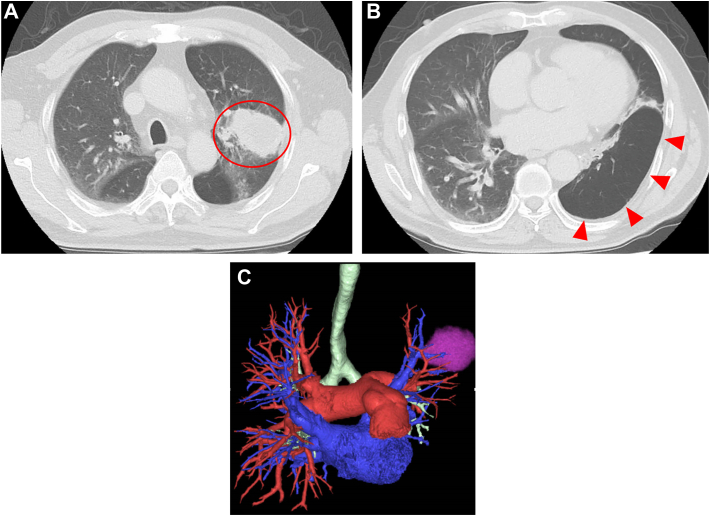 Figure 2
Figure 2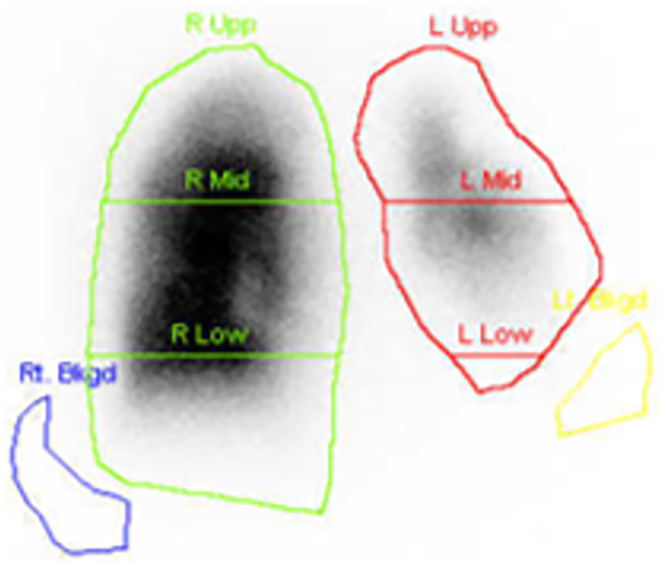 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Cancer-related molecular mechanisms research
Swyer-James-MacLeod syndrome (SJMS) is a rare disease, in 1953 first reported by Swyer and James1 in cases in children, and in 1954 by MacLeod2 in adults. It is characterized by unilateral hyperlucency of the lung on chest roentgenogram, unilateral reduction in vascularity on chest computed tomography (CT), and unilateral loss of perfusion on pulmonary ventilation/perfusion scan.3
SJMS associated with primary lung cancer is extremely rare, with only a few cases reported.4 Here, we report a case of left upper lobe lung cancer associated with SJMS in which left pneumonectomy was performed using robotic surgical system.
A man in his 70s visited the hospital complaining of chest pain. A chest CT showed a 50-mm mass in the left upper lobe. The specimen from a transbronchial lung biopsy of the tumor yielded a diagnosis of squamous cell carcinoma. He was then referred to our hospital for surgery.
Physical examination revealed no abnormalities. Tumor markers were detected as the following: squamous cell carcinoma antigen, 4.8 ng/mL (normal range, ≤1.5 ng/mL); and cytokeratin-19 fragment, 5.1 ng/mL (normal range, <3.3 ng/mL). Pulmonary function test result demonstrated forced expiratory volume in 1 second of 1.57 liters (52.5% predicted) and forced expiratory volume in 1 second/forced vital capacity ratio of 54.5%. Echocardiography showed fractional shortening of 0.43, ejection fraction of 0.60, and no abnormal findings.
Chest roentgenogram revealed a mass shadow in the left upper lung field (Figure 1), chest CT showed an irregular mass, 53 mm in diameter, in the left upper lobe, and both hyperlucency and diminished vascularity in the left lower lobe (Figures 2A, 2B). A 3-dimensional CT also showed hypoplasia of the left pulmonary artery (A6-10) and an inferior pulmonary vein (Figure 2C)Figure 1. Chest roentgenogram revealed a mass shadow in the left upper lung field.Figure 2(A) Chest computed tomographic image shows an irregular mass (red circle) measuring 53 mm in diameter in the left upper lobe. (B) Hyperlucency and diminished vascularity in the left lower lobe (red triangles). (C) Three-dimensional computed tomographic image shows hypoplasia of the left pulmonary artery (A6-10) and inferior pulmonary vein.
A fluorine-18 fluorodeoxyglucose–positron emission tomography scan showed abnormal accumulation of fluorodeoxyglucose (maximum standardized uptake value of 19.54) in the tumor.
A pulmonary ventilation/perfusion scan revealed markedly decreased pulmonary blood flow in both the left upper lobe with the tumor and the left lower lobe with both hyperlucency and diminished vascularity. The right-to-left ratio of blood flow was 86.18% on the right and 13.28% on the left (Figure 3).Figure 3. Pulmonary ventilation/perfusion scan shows markedly decreased pulmonary blood flow in both the left upper lobe with a tumor and in the left lower lobe with hyperlucency and diminished vascularity. (L, left; Low, lower; Mid, middle; R, right; Upp, upper.)
The clinical stage was cT3 N0 M0, stage IIB squamous cell lung carcinoma. In addition, SJMS was diagnosed for the left lower lobe. Robot-assisted thoracoscopic left pneumonectomy was performed. He had an uneventful course after the operation and was discharged home.
The postoperative pathology was squamous cell carcinoma with an invasion diameter of 45 × 45 × 30 mm. No lymph node metastasis was observed. The pathologic stage was pT2b N0 M0, stage IIA.
Comment
The prevalence of SJMS is reported to be 0.01%, with most cases occurring in children and only a few cases in adults.5 Bronchiectasis is not a finding in all SJMS patients, but it is present in 30% of patients and affects clinical presentation and prognosis.6
SJMS as assessed radiologically is predominantly unilateral, and pathologic criteria to diagnose it have not yet established, so other causes of a hyperlucent lung, such as pneumothorax, asymmetric emphysema, congenital lobar emphysema, pulmonary artery hypoplasia, pulmonary embolism, and bronchial obstruction due to foreign body or mucus plugs, should be ruled out.7
Even though the pathogenesis of SJMS has not yet been completely understood, the syndrome has been reported to usually occur after lung infection early in childhood, possibly due to infective agents that damage the bronchioles and prevent normal development of the alveolar ducts. Bronchiolitis obliterans results in inflammation and fibrosis in the walls and contiguous tissues of the membranous and respiratory bronchioles, with narrowing of their lumens. Fibrosis of the alveolar septum leads to obstruction of the pulmonary capillary bed, reducing blood flow to the major pulmonary arterial segments, leading to secondary pulmonary vascular hypoplasia and bronchial dysplasia, and causing air trapping due to peripheral airway obstruction, peripheral lung hyperinflation, and emphysematous changes.7 This case of SJMS was concomitant with ipsilateral lung cancer. Although, concomitant SJMS and lung cancer is rare, we think that this may be because SJMS itself is a rare disease.
Preoperative CT showed hyperlucency of the left lower lobe with hypoplasia of the pulmonary vasculature, consistent with imaging findings characteristic of the syndrome. There were also repeated episodes of respiratory infections in childhood, although details are unknown, which may have been related to the onset of the disease.
Although the patient had already been receiving inhalation therapy for chronic obstructive pulmonary disease, he had been asymptomatic without respiratory distress or oxygen demand until he was diagnosed with SJMS by preoperative CT. Surgical intervention is considered in cases involving repeated infections or progressive dyspnea, but treatment of SJMS is typically conservative and supportive, including inhaled bronchodilators, low-dose inhaled steroid, respiratory physiotherapy, and infection control.3^,^7 There are hardly any reports of surgical intervention for SJMS; however, a few reports have suggested that resection of lesions is effective in improving pulmonary function and relieving symptoms of respiratory distress due to decrease in ventilation/perfusion mismatch in the affected lobe.8
In this case, CT showed pulmonary vascular hypoplasia in the left lower lobe, and respiratory function tests and pulmonary ventilation/perfusion scan showed significant pulmonary hypofunction in the left lung due to tumor in the upper lobe and SJMS in the lower lobe, so left pneumonectomy was planned for this patient.
Although intraoperative adhesions was anticipated, robot-assisted thoracoscopic surgery was selected because we thought minimally invasive surgery was best, considering pulmonary hypofunction and complications such as diabetes mellitus. Preoperative imaging showed that the pulmonary artery might be friable, but intraoperative findings showed that the pulmonary artery and other tissues were not friable. The left lower lobe was emphysematous, and the inferior pulmonary vessels were hypoplastic, but the left pneumonectomy was successful without any problems. The patient's postoperative course was uneventful, and he is still alive 8 months after surgery, after undergoing postoperative adjuvant chemotherapy, without recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Swyer P.R.James G.C.W.A case of unilateral pulmonary emphysema Thorax 819531331307750810.1136/thx.8.2.133PMC 1019253 · doi ↗ · pubmed ↗
- 2Macleod W.M.Abnormal transradiancy of one lung Thorax 919541471317912710.1136/thx.9.2.147PMC 1019360 · doi ↗ · pubmed ↗
- 3Singal K.K.Bhatti K.P.Gupta A.Gupta N.Samra R.Gautam S.Swyer-James-Mac Leod syndrome: a rare case Bangladesh J Med Sci 142017402404
- 4Yoshida K.Koba H.Igarashi T.A case of Swyer-James syndrome—a morphological study with inflated fixed lung. Article in Japanese Nihon Kyobu Shikkan Gakkai Zasshi 3219948568607799555 · pubmed ↗
- 5Gaensler E.A.Unilateral hyperlucent lung Simon M.Potchen E.J.Le May M.Frontiers of Pulmonary Radiology 1969 Grune & Stratton 312359
- 6Abba A.A.Al-Mobeireek A.F.Clinical spectrum of Swyer-James Macleod syndrome in adults Saudi Med J 24200319519812682687 · pubmed ↗
- 7Sulaiman A.Cavaille A.Vaunois B.Tiffet O.Case report—thoracic non oncologic Swyer-James-Mac Leod syndrome; repeated chest drainages in patient misdiagnosed with pneumothorax Interact Cardiovasc Thorac Surg 820094824841916430910.1510/icvts.2008.197566 · doi ↗ · pubmed ↗
- 8Miyakoshi J.Makino T.Shiono S.Anami Y.Tojima H.Swyer-James Macleod syndrome with progressive hyperinflation Ann Thorac Surg 1142022 e 101e 1043490230010.1016/j.athoracsur.2021.10.059 · doi ↗ · pubmed ↗