Trauma nurses' experience of repositioning practice for trauma patients: a qualitative descriptive study
Abdulkareem S. Iblasi, Yupin Aungsuroch, I Gede Juanamasta, Ghassan Watffa, Yousef Al Omran, Batla Al Shammari

TL;DR
This study explores how trauma nurses in Saudi Arabia decide to reposition patients, finding that clear policies, teamwork, and resources are key to preventing pressure ulcers.
Contribution
The study provides new insights into the factors influencing trauma nurses' repositioning practices in emergency and ICU settings in Saudi Arabia.
Findings
Clear policies, teamwork, and managerial follow-up influence nurses' repositioning decisions.
Delays in medical decisions and heavy workloads often lead to repositioning being omitted.
Skill gaps and lack of equipment hinder nurses from completing repositioning even when intended.
Abstract
Clinical evidence indicates that the low frequency of repositioning among trauma nurses contributes to pressure ulcers during hospitalization. This study aimed to understand how trauma nurses address the need for repositioning patients in an emergency room and intensive care unit in Saudi Arabia. A qualitative descriptive design was employed, and the study was reported in accordance with COREQ guidelines and checklist. Semi-structured interviews were conducted with nurses to explore how they interact with the need for repositioning patients. Rigor was ensured using the criteria established by Lincoln and Guba. Fifteen nurses from a large government hospital in Saudi Arabia participated in the study. The findings revealed that the policy's clarity, the presence of teamwork, and the level of managerial follow-up influenced nurses' decisions to proceed and perform repositioning. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
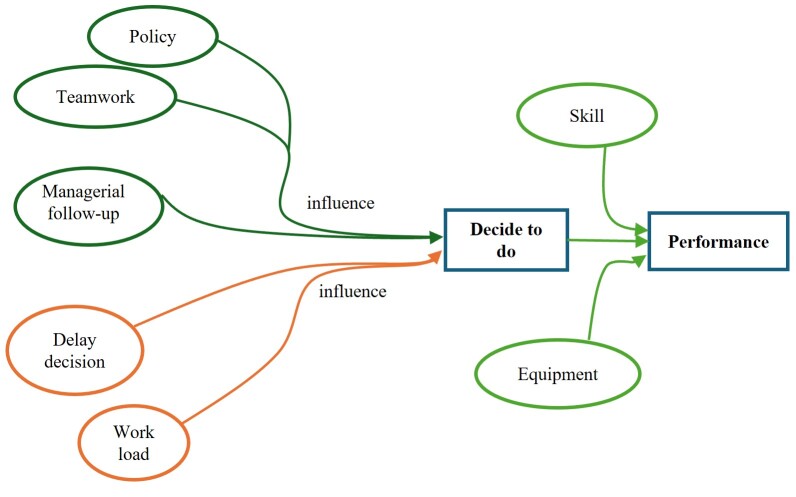 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmergency and Acute Care Studies · Trauma and Emergency Care Studies
Introduction
The World Health Organization (WHO) has reported that Saudi Arabia has one of the highest prevalence of motor vehicle accidents (MVAs), with around 27 deaths per 100,000 people annually1. Combined with a high number of construction- and labor-related injuries,2 this result makes the Saudi Arabian healthcare system deal with a high prevalence of trauma patients on a daily basis3. The majority of these injuries require hospitalization4.
Although most trauma patients are young and healthy, they are more likely to develop pressure ulcers during their hospitalization due to conditions or therapies that limit mobility3,5. However, research shows that not all immobile patients develop pressure ulcers. For instance, following hip replacement or spinal surgery, patients often require restricted mobility, but they are less likely to develop pressure ulcers6-8. According to internal statistics, 15 to 17 patients in trauma units develop new pressure ulcers each month, with a reported prevalence rate of at least 15% in 20189.
Terms such as pressure ulcer, pressure injury, bedsore are all expressions that refer to tissue damage caused by gravitational pressure over bony prominences or from medical devices10-12. Experts have published several protocols and guidelines to prevent pressure ulcer development, including the use of pressure-relieving mattresses, prophylactic dressings13, improved nutritional levels, and regular repositioning14-17. These aspects are mandatory for immobilized trauma patients.
Repositioning is essential in preventing pressure ulcers12. It is the most commonly used intervention among all others and demands physical and mental focus from nurses to conduct it18. Stabilizing the patient in the new position is part of repositioning19,20. It is important to avoid muscular injuries and physical strain during patient handling. Several approaches have been researched to ensure the safety of both nurses and patients during repositioning21. Improper techniques may put nurses and patients at risk22. However, inadequate repositioning procedures are common among this patient group, with hospital compliance indicators falling below 60.00%9.
This study aims to understand how trauma nurses perceive and implement repositioning practices among trauma patients in the emergency room and intensive care units at one of the largest trauma centers in Saudi Arabia. Currently, there are no studies available that examine nurses' actual behaviors and approaches to repositioning in trauma care, and how these may differ from those used in non-trauma conditions.
Materials and Methods
Study design
The study employed a qualitative descriptive design, using semi-structured interviews, and was reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ)23,24. The study aims to describe how nurses address the need for repositioning practices among immobilized trauma patients.
Setting
The study was conducted at the largest government hospital in Saudi Arabia. The hospital employs approximately 5,000 nurses distributed across all categories of healthcare services. Approximately 450 nurses regularly work with trauma patients in this hospital, which has around 120 beds with an occupancy rate exceeding 90% throughout the year, all due to trauma injuries9. The hospital's official language is English, which was used for the interviews, as well as for the data analysis and interpretation in this study.
According to hospital policy, when a pressure ulcer (or any skin injury) is identified, nurses must report the case to the wound care unit for assessment and treatment. If the injury is confirmed as a pressure ulcer, the wound care unit notifies the nursing quality team for documentation. For each case, the wound care unit registers the patient’s demographic information and the identity of the reporting nurse. In the current setting, several policies are in place to encourage nurses to report skin injuries observed in patients, and no blame is assigned for such reports.
Participants and Sampling
Inclusion Criteria. Eligible participants were clinical nurses currently working in the trauma emergency unit or the trauma intensive care unit who had reported at least one case of hospital-acquired pressure ulcer, based on wound care records, during the past 90-day period preceding the study's initiation (July 1–September 29, 2019). The rationale was that nurses who had reported pressure ulcer cases were likely more aware of the issue and committed to its prevention. Since repositioning is part of pressure ulcer prevention, these nurses were expected to provide insights into how such practice is implemented. Frontline nurse managers were excluded from the study as they are less likely to be directly involved in decision-making regarding repositioning practices, even though they may occasionally file reports on pressure ulcers.
Research team. It comprised seven members, four of whom were affiliated with the hospital. The lead researcher is the hospital's wound care manager and lead author of the study. Two team members are also family medicine consultants (at a community center) and work together. The fourth research member is a nurse recruiter. None of the team members holds administrative or managerial roles in the trauma units or supervises nurses working in trauma units. Their positions are known among trauma nurses at the same institution. The remaining three researchers are affiliated with an institution in Thailand and have no direct or indirect ties to the study institution. The research team held online meetings to monitor the study's progress and conclusions. The research team agreed that data saturation would be defined as three consecutive interviews yielding no new information24.
**Sampling. **Researchers sent an email to all eligible nurses based on wound care records, which showed 42 nurses. The email explained the purpose of the study and confirmed that ethical approval had been obtained from the hospital. The email also requested a reply if they agree to participate25. Twenty-three nurses responded affirmatively. Participants were selected in the order of their responses, and interviews were conducted until fifteen nurses had been interviewed, at which point data saturation was reached, based on the study assumptions.
Data collection
The research team developed a semi-structured interview guide based on Moerman's26 recommendations. All team members approved the interview items, which are presented in Table 1. The interview guide was validated by two experts in qualitative studies, and a pilot interview was conducted with the trauma nurse educator. This pilot interview was excluded from the analysis because the educator did not meet the inclusion criteria, and the purpose of the interview was solely to assess clarity and flow. No significant changes were made to the interview guide following the pilot test.
Table 1 Semi-structured interview guidePhase Items Tips and notes Introduction We want to ensure that we accurately capture everything you say, so we are going to record this interview. The recording will help us remember everything you have said without any mistakes. Every word you say is important for us to understand the topic of the study. Be sure that only the research team will listen to this recording, and all recordings will be deleted upon completion of the study. We would like to ask your permission to record this interview. Warm-up phase How would you describe your experience with pressure ulcer issues in your unit? What about repositioning practices? Competency, experience, training, and understanding of nurses' empathy. Focus on facts and situation descriptions. Core - Why do you think you perform repositioning for some patients in trauma units?
- Why do you think some nurses do not perform repositioning?
- What do you think makes them do that?
- How do they come to that result? Difficult part Explore the situation Process thinking Wrap-up - What do you think you and other nurses need?
- What should be the nature of repositioning? Less sensitive topics Closing - Is there anything you would like to add?
- Thanks for your participationClosing the discussion
Interviews were conducted by the lead researcher in a private room located within the hospital, away from the trauma units. On the day of each interview, the lead researcher requests an official leave from the nurse manager of the nurse's unit. The researcher arranged seating accommodations in the room and offered hot or cold beverages based on participants’ preferences, as well as bottled water. Except for one interview conducted in the afternoon (1:20 p.m.), all interviews were held in the early morning (between 7:15 a.m. and 8:15 a.m.), as this was the most convenient time for participants. All participants consented to audio recording. The interviews were conducted between October and November 2019. No financial incentives were offered for participation. All interviews were conducted in private, with only the participant and the lead researcher present in the room. The duration of the interviews ranged from 30 to 55 minutes, as detailed in Table 2 alongside participants' demographic data. No signs of discomfort or stress were observed among the participants; all appeared relaxed and engaged in the discussion.
Data Analysis
The audio recordings were transcribed into Word documents by research team members and independently verified by the lead researcher and other team members. All members reviewed the recordings and cross-checked them against the written transcripts to ensure accuracy.
Data analysis was conducted using a thematic analysis approach, which followed four main steps27,28. First, themes were independently generated for each interview. Three research team members individually read the transcripts and identified recurring themes based on their interpretation of the data. Second, themes were compared between pairs of interviews. Each pair of transcripts was independently analyzed by the researchers. Third, themes from each interview were compared with the themes generated by the three researchers from the same interview27. Fourth, all themes were compared together for all interviews. The data collected are available for free access and consultation in Mendeley Data29.
Rigor
This research employed the rigor criteria established by Lincoln and Guba. Credibility was addressed by thoroughly documenting each participant's statements in full and without alteration, thereby enhancing the study's descriptive validity. Through this interpretation, the researchers deepened their understanding and analysis of the expressions and thematic clusters, further strengthening the validity of the findings. For data triangulation, the researcher cross-examined the information provided by each participating nurse. To improve the verification of interviews, each participant was consulted regarding the transcript of their interview. Meanwhile, the researchers ensured that all collected data were verifiable, thereby supporting dependability. Comparable outcomes may be achieved by replicating this study. The researchers conducted a confirmability test guided by objectivity, ensuring that the findings reflected the participants' perspectives. To further ensure trustworthiness of the results, the researchers triangulated data from multiple sources and conducted member database check-ins to support transferability.
Ethical Considerations
Ethical approval was obtained from the Institutional Research Board of King Saud Medical City prior to data collection (Ref: H1RI-03-Dec18-01). This study is a part of a broader study titled “The Scale Development of Nursing Repositioning Practice for Bedridden Patients in Saudi Arabia.” All nurses involved in this study agreed to participate in interviews and were informed of their right to withdraw from the study at any time. The participants provided informed written consent before the interviews, following hospital protocol30.
Results
Fifteen nurses were interviewed: eight from the trauma emergency unit and seven from the trauma intensive care unit. Participants' demographic characteristics are summarized in Table 2. The findings indicate that nurses go through two critical decision points before performing repositioning, as described below. No notable differences were observed in responses based on gender, experience, or nationality.
Table 2 Participants' demographic dataVariable n=15 % (n) /Mean ± SD Age years (SD) 31.86 ± 6.32Sex Female 86.00 (13) Male 14.00 (2) Years of experience (SD) 9.8 ± 6.32 Years in current unit (SD) 4 ± 1.6 Nationality Saudi 60.00 (9) Indian20.00 (3) Filipino6.67 (1) Jordanian 6.67 (1) British 6.67 (1) Unit Trauma Emergency 53.33 (8) Non-Trauma Emergency 46.67 (7) Qualification BSN 80.00 (12) Diploma 20.00 (3) *SD: standard deviation BSN: Bachelor of Science in Nursing
From realization to decision
There was consensus among the participants that repositioning is important for preventing pressure ulcers in immobile patients, whether due to trauma or other medical conditions. Participants agreed that nurses can determine when a patient needs repositioning and describe this as a basic nursing skill. However, participants indicated that after recognizing the need for repositioning, nurses often encountered differences related to external factors. These included the following:
Repositioning policy for trauma patients
Although the hospital has a repositioning policy for immobile patients, it lacks specific guidelines for trauma patients, a distinction that sets trauma care and trauma units apart. Most participants said that unclear instructions influenced their decision to proceed with repositioning, whether to perform it as part of routine care or to avoid it due to concerns about patient safety. Participants reported feeling less confident and more stressed when planning repositioning, as the policy does not directly provide trauma-specific guidance. Despite this, the participants clearly relied on institutional policy.
“We know from the American Heart Association's BLS [Basic Life Support] guidelines …to not extend the neck if there's trauma, so I should follow that as the policy we have doesn't say anything specific about trauma patients when it comes to repositioning, right?” Participant 5
“Nurses feel safer when there's a clear policy guiding their actions.” Participant 8
“…repositioning should be done according to a specific protocol that tell us how and when to turn a trauma patient, but we just don't have one.” Participant 7
Delayed medical decisions
Medical decisions in trauma care often depend on the results of several diagnostic examinations before a final treatment plan can be established. These evaluations may take several hours to complete all required radiological investigations. However, the participants identified the delay in decision-making as a demotivating factor when it comes to initiating repositioning, as reflected in the following quotes:
“…they [doctors] keep doing their rounds over and over, and there's still no final decision. Is there a spinal cord injury or not? Is it safe to reposition or not? So we just can't take that responsibility! It could make the injury worse.” Participant 4
“We [nurses] need to wait for three or four different teams to come and tell us what to do, or what not to do, and there's no time limit for when the doctors have to make that decision.” Participant 3
- “Nurses can't take the risk until they get the okay from the doctors. Sometimes, that takes a whole shift [a shift equals 12 hours in trauma units] or even longer.” Participant 6*
Teamwork spirit
Repositioning is a task that requires the collaboration of two or more nurses. Thus, teamwork plays a significant role in its successful execution. Participants explained that having a cooperative and supportive team facilitates repositioning for nurses. When one nurse requests assistance, others are willing to assist, which promotes compliance.
“Many things enhance repositioning, like teamwork. When you ask me to help you reposition your patient, then later you’ll help with mine…” Participant 4
**Workload **
Nurses reported that they are more likely to perform patient repositioning when the workload is manageable. However, nurses are less likely to perform patient repositioning when the workload is perceived as high. This concern was raised by four participants, suggesting the need for further investigation into this point for a deeper understanding of how nurses prioritize nursing tasks and where repositioning falls among their other competing tasks.
“When there’s too much work going on, you end up forgetting about repositioning…” Participant 9
- “The workload, sir… when there’s a high workload, no one's available to help with repositioning.” Participant 11*
Managerial follow-up
Participants agreed on the important role of head nurses in following up on repositioning practice. Nurses are often subjected to multiple distractions. The participants felt that the role of the unit head nurse was to oversee nurses' compliance with nursing care protocols, including repositioning. As such, the lack of managerial oversight was perceived to have a negative impact.
-
“…The head [head nurse] should keep following up nurses’ performance in all aspects of nursing care, including repositioning.” Participant 1*
-
“Reminding nurses about repositioning, follow up to see if they do it, probably do it, or don't do it, and even help them…” Participant 8.*
From the decision to behavior
Even after deciding to perform repositioning, nurses will encounter additional challenges that prevent them from proceeding with repositioning. Some barriers identified are the following:
Repositioning equipment
Although the participants agreed on the importance of repositioning aids, many argue that such devices are not available in sufficient quantities. As a result, when a nurse needs a device that is unavailable, this often leads to delays or even avoidance of the procedure.
*“Sometimes, we can't turn a patient with bilateral chest tubes. There is something that can help, like the lifting devices.” Participant 4 *
*“… there's only one lifting device. So by the time you request it and it arrives, it takes a while, and sometimes it's already taken on the fifth floor [referring to the bariatric unit], so it takes more than an hour to get here.” Participant 6 *
Lack of required skills
It is reasonable to expect that nurses should have the necessary skills to perform repositioning safely and effectively. However, analysis of participants' responses indicated a perceived lack of sufficient skills for repositioning patients with specific trauma-related conditions, particularly those involving tractions, fixators, or connected devices. Participants noted that this skill gap increased their stress levels when attempting to reposition patients connected with different kinds of devices. Moreover, they emphasized that skills are needed to practice repositioning safely and effectively.
“… how to do it in a good way with many devices or tractions... so...[they] just try not do it…” Participant 4
-
“We also need further support by doing this in front of us. Someone should come and do it for me, right? Not just say 'You should put the device here or there' but [with] no actual application, it's still a problem.” Participant 12 *
-
“I don't think they [nurses] have a proper kind of training. So even if they [nurses] plan to do it, when seeing the devices and connections, they [nurses] back out [of repositioning].” Participant 3*
Discussion
Repositioning practice for trauma patients is the result of two points of interaction: the pre-decision point, when the nurse decides whether or not to reposition the patient, and the pre-behavior point, as illustrated in Figure 1.
The presence of clear policies, the timing of medical decisions, teamwork, workload, and managerial follow-up are crucial factors influencing nurses' decisions to either perform or defer patient repositioning. The impact of delays in medical decision-making on repositioning practice was clearly a contentious issue. Although such delays are not within the scope of nursing responsibility, they significantly affect the overall quality of nursing care. Therefore, establishing a maximum timeframe for making medical decisions is necessary for repositioning interventions.
Figure 1. Conceptual Diagram of Repositioning Practice
The interplay of these factors, whether proceeding with patient repositioning or not, is consistent with other studies18, as nurses evaluate the environment before conducting interventions. The Theory of Planned Behavior refers to this evaluation phase as behavioral intention31. Similarly, Orem's Theory of Self-Care describes it as nursing agency, when nurses recognize the need for care and initiate strategies to meet that need32. Consequently, maintaining a positive decision-making environment is crucial to promoting repositioning behavior. The results suggest that a lack of policies, delayed medical decisions, and high workload collectively reduce the possibilities of repositioning being performed. Thus, hospitals should strive to clarify their policies, improve the perceived workload, and minimize delays in medical decision-making. Hospitals should also support frontline nurse managers' responsibility in monitoring this nursing behavior. Frontline nurse managers play a crucial role in monitoring patient repositioning, which includes head nurses, charge nurses, and ward sisters33.
The data further indicated that, even after deciding to perform patient repositioning, nurses face a second critical point, which is evaluating their competencies and equipment availability in relation to the patient's needs. Lifting devices help nurses place patients in a new position34,35, reduce the physical effort required to reposition them36,37, and protect nurses’ backs from injuries during repositioning35,38. However, even when nurses decide to proceed with patient repositioning, a perceived lack of skills or inadequate equipment may ultimately prevent them from performing the procedure.
It is evident that human behavior is influenced by many individual and interconnected, complex factors; therefore, it is not always easy to understand all the relevant factors. However, gathering descriptions of patient repositioning from the participants' accounts provides valuable insight into the urgent need to modify policies and procedures related to trauma care services. Specifically, the findings highlight the urgent need to develop clear policies and protocols for repositioning different types of immobilized trauma patients, establish time limits for medical teams to clarify repositioning restrictions, ensure these timeframes align with accepted repositioning intervals in Saudi Arabia (approximately every two hours)39, and provide tools and equipment to support repositioning in trauma units.
Limitations
The current study had some limitations. First, four members of the research team were employed at the hospital where the study was conducted, which may have influenced participants' responses in some way. Second, this study was conducted in a trauma center; therefore, these results might differ if the study were replicated in other healthcare centers or discussed in different contexts. Finally, the current study explored the views of clinical nurses, excluding those in managerial or administrative roles who might have different viewpoints or perceptions of the facts.
Conclusions
There are two overarching explanatory themes regarding trauma patient repositioning: factors influencing the decision to perform repositioning, and factors supporting the transition from decision to action. The results highlight the challenges trauma nurses face in implementing repositioning and the need for clear policies, teamwork support, further follow-up from frontline managers, appropriate skills, and equipment. Additionally, previous studies have shown a significant correlation between pressure ulcer development and workload; however, the extent to which this relationship may differ in trauma units needs further research. Moreover, follow-up studies are required to investigate the changes in the repositioning practice and pressure ulcer prevalence among these units after modifying these factors. Finally, future studies should develop and validate tools to measure repositioning practices in trauma units.
Relevance for clinical practice
Nurse managers are encouraged to use these findings to improve hospital policies related to trauma patient repositioning, clarifying indications, contraindications, patient conditions, timing, and the number of staff needed for safe implementation of repositioning. A clear and specific standard is needed for each ward. Additionally, nurse managers should promote skill development and updating in the use of repositioning devices. Their role in supervising and motivating nursing staff to perform repositioning is crucial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Global status report on road safety 2015: World Health Organization. [Internet] 2015 Jan 20, 2020 https://www.who.int/publications/i/item/9789241565066
- 2Abukhashabah E Summan A Balkhyour M Occupational accidents and injuries in construction industry in Jeddah city Saudi J Biol Sci 202027 8 1993 810.1016/j.sjbs.2020.06.03332714023 PMC 7376124 · doi ↗ · pubmed ↗
- 3Al-Naami MY Arafah MA Al-Ibrahim FS Trauma care systems in Saudi Arabia: an agenda for action Ann Saudi Med 2010 301 50 8 10.4103/0256-4947.5937420103958 PMC 2850182 · doi ↗ · pubmed ↗
- 4Rafiei H Abdar ME Iranmanesh S Lalegani H Safdari A Dehkordi AH Knowledge about pressure ulcer prevention, classification and management: A survey of registered nurses working with trauma patients in the emergency department International Journal of Orthopaedic and Trauma Nursing 201418 3135 42 10.1016/j.ijotn.2014.03.004 · doi ↗
- 5Ham HW Schoonhoven LL Schuurmans MMJ Leenen LLP Pressure ulcer development in trauma patients with suspected spinal injury; the influence of risk factors present in the Emergency Department International emergency nursing 2017 30 13 9 10.1016/j.ienj.2016.05.00527450044 · doi ↗ · pubmed ↗
- 6Baldwin KM Ziegler SM Pressure ulcer risk following critical traumatic injury Journal of Orthopaedic Nursing 1998 24 234 10.1016/S 1361-3111(98)80058-710326336 · doi ↗ · pubmed ↗
- 7Cyriacks B Spencer C Reducing HAPI by cultivating team ownership of prevention with budget-neutral turn teams Medsurg Nursing 2019 281 4852 https://www.proquest.com/openview/dd 9dc 13fc 3f 9b 8e 9ebc 9f 38e 0b 97da 49/1?pq-origsite=gscholar&cbl=30764
- 8Wu T Wang S-T Lin P-C Liu C-L Chao Y-FC Effects of using a high-density foam pad versus a viscoelastic polymer pad on the incidence of pressure ulcer development during spinal surgery Biological research for nursing 201113 4 419 24 10.1177/109980041039277221196422 · doi ↗ · pubmed ↗