The effects of the introduction of the single-family room in neonatal and paediatric intensive care on the outcomes of paediatric patients, families, staff, and organizations: a mixed method systematic review
Giulia Ottonello, Silvia Rossi, Nicoletta Dasso, Roberta Da Rin Della Mora, Simona Calza, Giuseppe Minniti Caracciolo, Ilaria Artuso, Simona Serveli, Fulvia Esibiti, Chiara Rebuffi, Stefano Parodi, Silvia Scelsi

TL;DR
Single-family rooms in neonatal and pediatric intensive care improve patient outcomes and family involvement but require careful implementation to support staff and avoid sensory deprivation.
Contribution
A mixed-method systematic review analyzing the effects of single-family rooms in NICUs and PICUs on patients, families, staff, and organizations.
Findings
SFRs in NICUs improve neonatal neurodevelopment, parental participation, and staff satisfaction.
Infants in SFRs show better sleep regulation, higher breastfeeding rates, and shorter hospital stays.
SFRs may cause sensory deprivation risks and communication challenges for healthcare staff.
Abstract
The introduction of single-family rooms (SFRs) in neonatal (NICUs) and paediatric intensive care units (PICUs) enhances family involvement and transforms healthcare professionals’ approach to patient care. This shift promotes family-centred care while requiring adjustments in staff workflows and communication. Given the significant implications of this structural change, this review examines the effects of SFRs on paediatric intensive care patient outcomes, families, healthcare staff, and healthcare organizations. A systematic search was conducted in PubMed, CINAHL, PsycINFO, EMBASE, SCOPUS and Web of Science databases and grey literature. Studies published in English, Italian, and Spanish from 2009 to 2025 were included. The review adhered to the Johanna Briggs Institute methodology and PRISMA reporting guidelines to ensure rigor and transparency. A total of 649 records were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
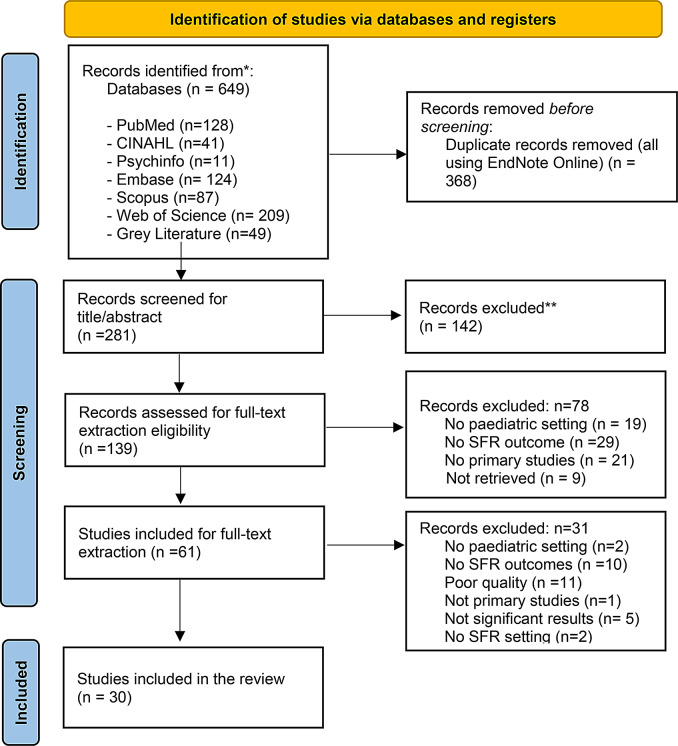 Figure 1
Figure 1- —Ministero della Salute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Development and Preterm Care · Family and Patient Care in Intensive Care Units · Neonatal Respiratory Health Research
Background
Over the past two decades, the physical environment of neonatal (NICU) and paediatric intensive care units (PICU) has gained increasing attention for its impact on patient care, family well-being, and healthcare staff experiences. Traditional Open Bay (OB) models, where multiple patients share a single space, have long been the standard in NICUs and PICUs. However, a growing emphasis on family-centred care (FCC**)** has led to the introduction of single-family rooms (SFRs)**—**private hospital spaces that allow parents to remain with their child in a single room 24 h a day throughout hospitalization. This model is designed to create a home-like environment that fosters continuous parental involvement, strengthens parent-child bonding, and reduces stress for both patients and families [1].
Since 2009, SFRs have been progressively introduced in NICUs, with evidence suggesting significant benefits for neonatal health outcomes, parental well-being, and healthcare delivery [2, 3]. Inside these rooms, families have access to essential amenities such as sleeping areas, kitchens, and designated spaces for relaxation and play. Unlike the OB model, which exposes infants to excessive noise, light, and frequent disruptions, SFRs offer greater control over the environment, helping to regulate sensory stimulation and improve the overall care experience [4].
The existing literature indicates that SFRs have a positive impact on multiple aspects of care [2, 5]. Many studies have found that infants in SFRs experience better neurodevelopmental outcomes, improved sleep patterns, increased exclusive breastfeeding rates, and a shorter length of hospital stay. Parents who remain continuously present report stronger emotional bonding, earlier milk expression, and reduced stress and anxiety [6]. From a healthcare system perspective, SFRs have been associated with enhanced infection control, improved workflow efficiency, and potential cost savings due to a reduction in hospital days [5, 7].
Additionally, while healthcare staff generally acknowledge the advantages of SFRs, there are challenges associated with their implementation. Some studies report increased job satisfaction, improved family-centred care delivery [8, 9] and reduced noise and alarm fatigue among healthcare professionals [10]. However, others highlight concerns such as emotional strain, professional isolation, and reduced peer support, particularly among nurses [4].
A key challenge is maintaining effective communication and teamwork in a setting where staff interactions may be reduced due to the physical separation of patient rooms [8, 11]. Furthermore, there are concerns that sensory deprivation in SFRs—due to reduced exposure to hospital environment sounds and human interactions—might negatively influence language acquisition and motor development in infants, warranting further investigation [12–14]. However, while the benefits are well-documented in NICUs, research on SFRs in PICUs remains scarce. Given the different needs of critically ill paediatric patients—who often require more intensive monitoring and interventions—the feasibility and impact of SFRs in PICU settings are less understood [15]. Assessing how SFRs influence clinical outcomes, parental involvement, staff experiences, and healthcare organization dynamics is crucial to optimize intensive care environments.
The purpose of this review is to identify the impact of SFRs on paediatric patient outcomes, family engagement, staff experiences and organization, contributing to the ongoing development of evidence-based neonatal and paediatric intensive care models. Therefore, the research question was as follows: “What are the effects of the introduction of SFR in paediatric intensive care units and neonatal intensive care units on paediatric patients (0–18 years) outcomes, on family outcomes, on staff outcomes, and on organizational outcomes?”
Methods
Aim
The aim of this review is to identify the effects of the introduction of the SFR in NICU and PICU settings on paediatric patients (premature infants, newborns, infants, children and adolescents) outcomes, on the outcomes of families (intended as parents /caregiver in reference to the figures connected to the child who are physically in the room together with the patient) [16], on the outcomes of the clinical, care and transitional care staff, and on the organizational outcomes.
Design
This is a mixed-methods systematic review with protocol registered in PROSPERO (International Prospective Register of Systematic Reviews)- CRD42024501520. Authors followed the mixed-methods systematic reviews guidelines (Mixed Methods Systematic Review of the Johanna Briggs Institute (JBI)). More protocols details can be found here [17].
Inclusion and/or exclusion criteria
In this review, studies were included if they: (1) examined the impact of the single-family room (SFR) setup in neonatal and paediatric (0–18 years) intensive care units (NICUs and PICUs) on patients, families, healthcare staff, or organizations; (2) were primary studies using quantitative, qualitative, or mixed-methods designs; (3) were published in English, Italian, or Spanish; (4) were published from 2009 to June 2025 following the introduction of the SFR design in neonatal and paediatric intensive care units [2, 3].
Non-primary studies, including literature reviews and meta-analyses, were excluded.
Search strategy
The search strategy was developed in collaboration with a librarian (CR), and details and keywords are outlined in Table 1. The terms, as well as indexed terms from each database, were incorporated into the search strategy, which was adapted for each database to ensure a comprehensive retrieval of relevant studies.
Table 1. Search strategyDATABASESearch Strategy PubMed ((“single family room*“[Title/Abstract] OR “single family room*“[All Fields] OR “single room*“[Title/Abstract] OR “private room*“[Title/Abstract]) AND (“intensive care“[Title/Abstract] OR “intensive care unit*“[Text Word] OR “ICU“[Title/Abstract] OR “pediatric intensive care unit“[All Fields] OR “PICU“[Title/Abstract] OR “neonatal intensive care unit“[All Fields] OR “NICU“[Title/Abstract]) AND ((english[Filter] OR italian[Filter] OR spanish[Filter]) AND (allchild[Filter] OR newborn[Filter] OR allinfant[Filter] OR infant[Filter] OR preschoolchild[Filter] OR child[Filter] OR adolescent[Filter]) AND (2009:2025[pdat])) CINAHL AB (single family room OR single-family room OR single room OR private room) AND AB (intensive care OR intensive care unit OR ICU OR pediatric intensive care unit OR PICU OR neonatal intensive care unit OR NICU) Limiters - Publication Date: 20090101–20250630Expanders - Apply related words; Apply equivalent subjectsNarrow by Language: - english. italian, spanishNarrow by SubjectAge: - child, preschool: 2–5 yearsNarrow by SubjectAge: - child: 6–12 yearsNarrow by SubjectAge: - adolescent: 13–18 yearsNarrow by SubjectAge: - infant: 1–23 monthsNarrow by SubjectAge: - infant, newborn: birth-1 monthNarrow by SubjectAge: - all infantNarrow by SubjectAge: - all childSearch modes - Boolean/Phrase PsychInfo (single family room* or single-family room* or single room* or private room*) AND (intensive care or intensive care unit or ICU or pediatric intensive care unit or PICU or neonatal intensive care unit or NICU).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures, mesh word]limit 3 to (human and english, italian, spanish language and (100 childhood < birth to age 12 yrs > or 120 neonatal < birth to age 1 mo > or 140 infancy < 2 to 23 mo > or 160 preschool age < age 2 to 5 yrs > or 180 school age < age 6 to 12 yrs > or 200 adolescence < age 13 to 17 yrs>) and yr="2009–2025”) Embase (‘single family room*’:ab, ti OR ‘single-family room’:ab, ti OR ‘single room’:ab, ti OR ‘private room’:ab, ti) AND (‘intensive care’:ab, ti OR ‘intensive care unit*’:ab, ti OR ‘pediatric intensive care unit*’:ab, ti OR ‘neonatal intensive care unit*’:ab, ti OR picu: ab, ti OR nicu: ab, ti) AND ([newborn]/lim OR [infant]/lim OR [child]/lim OR [preschool]/lim OR [school]/lim OR [adolescent]/lim) AND [2009–2025]/py AND ([english]/lim OR [italian]/lim OR [spanish]/lim) Scopus (TITLE-ABS-KEY (“single family room*” OR “single- family room” OR “single room” OR “private room”) AND TITLE-ABS-KEY (“intensive care” OR “intensive care unit” OR “ICU” OR “pediatric intensive care unit” OR “PICU” OR “neonatal intensive care unit” OR “NICU”)) AND PUBYEAR > 2008 AND PUBYEAR < 2024 AND (LIMIT-TO (EXACTKEYWORD, “Infant, Premature”) OR LIMIT-TO (EXACTKEYWORD, “Child”) OR LIMIT-TO (EXACTKEYWORD, “Infant Care”) OR LIMIT-TO (EXACTKEYWORD, “Nursing Staff, Hospital”) OR LIMIT-TO (EXACTKEYWORD, “Health Care Personnel”)) AND (LIMIT-TO (LANGUAGE, “English”, “Italian”, “Spanish”)) Web of Science (WoS) (TS= (“single family room*” OR “single- family room*” OR “single room” OR “private room”)) AND TS=(“intensive care” OR “intensive care unit” OR ICU OR PICU OR NICU)Refined by: languages English, Italian, SpanishPublication date: 2009–2025
A comprehensive systematic search was carried out in December 2023 and then updated in June 2025 across six electronic databases: PubMed, CINAHL, PsycINFO, EMBASE SCOPUS and Web of Science. Grey Literature was explored. In addition, reference lists from relevant systematic reviews and other types of reviews were screened to identify any additional studies that may not have been retrieved in the initial search.
Study selection and screening
All citations retrieved from the search were imported into EndNote Web, where duplicates were removed. The titles and abstracts of the studies were screened by five groups of researchers, each consisting of two members to determine eligibility for inclusion. Screening for full-text articles inclusion was assessed, and reasons for exclusion at this stage were recorded by the same groups of researchers. Any disagreements regarding study inclusion were resolved through discussion among the review team.
A detailed account of the studies excluded in the review process and reasons for exclusion is documented in PRISMA [18] diagram (Fig. 1).
Fig. 1PRISMA 2020 flow diagram *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/
Data extraction
Three reviewers (GO, SR, ND) independently conducted the critical full-text evaluation and data extraction using a specific Data Extraction Table on Excel sheet. To test the quality of the table and the data extraction process, three authors independently extracted the data from the first three studies (in alphabetical order). After that, the authors came together to share and determine whether their approaches of the data extraction were consistent with each other’s output and whether the content of the table was in line with the research question. No reason was found to modify the data extraction tables or planned process. After a consensus of the data extraction process was reached, the data were extracted by the three independent reviewers. They then met to discuss their findings and reach a final agreement for included studies. In cases of disagreement that could not be resolved through discussion, a further reviewer was consulted for the final evaluation.
This data extraction table included the following elements: Author and Year, Country, Study Aim, Study design, Study population, Sampling, Sample size, Participants, Setting, Data Collection, Data analysis, Outcome measurements tools, Key findings, Patient outcomes, Family outcomes, Healthcare staff outcomes, Organizational outcomes, Conclusions, Limitations and Quality Appraisal.
The JBI’s Critical Appraisal Tools [19] (specific JBI’s tool for each type of study reviewed) were used to evaluate the quality of the included studies.
Data synhtesis
The three reviewers mentioned above performed the narrative synthesis to describe the key findings and identify gaps in the literature. The narrative synthesis utilized words and text to describe study characteristics, context, quality, and results. To facilitate comparison of the extracted data, tables developed with information in the data extraction Excel table are presented in the sections below [20].
Results
Search results
From six different electronic databases, 649 citations were identified as being potentially relevant to the review. Then, 368 duplicates were removed by an automation tool (EndNote Online). The titles and abstracts of 281 citations were reviewed, and a total of 139 records were assessed for full text extraction eligibility. A total of 61 studies were included for full text extraction. Based on the eligibility criteria, 30 studies were critically appraised and deemed suitable for inclusion in the review. The search results and selection process are presented in the PRISMA [18] flow diagram (Fig. 1) while key findings and study characteristics are described below and in Tables 2 and 3.
Table 2. Characteristics of included studiesAuthor(s)(Year)CountryDesign/Study typePopulationSettingCone et al., 2010USACross-sectional survey-based study107 NICU staff members (nurses, physicians, respiratory therapists, and other support personnel)NICUDoede & Trinkoff, 2020USAQualitative interpretive description15 neonatal nursesNICUDomanico et al., 2010USAProspective studyNICU parentsNICUFay et al., 2023USAPre-/post-occupancy evaluation with a multimethodological design using staff surveys, observations, and focus groups.NICU Staff members (81 pre and 131 post)NICUGrundt et al., 2021NorwayLongitudinal, prospective, comparative, observational study77 Infant and 66 mothersNICU with SFR and OBJoshi et al., 2018The NetherlandsRetrospective comparativeNICU patients(SFR 158; OB 170)Two NICUsKainiemi et al., 2021FinlandPre–post studyParents of preterm infants born before 35 weeks of gestation and admitted to the NICUNICUKudchadkar et al., 2016USAA cross-sectional studyPICU nursesPICULester et al., 2014USALongitudinal, prospective, quasi-experimental cohort study403 NICU patients 151 OB; 252 SFR)NICULester et al., 2016USALongitudinal, follow-up, quasi-experimental cohort study216 NICU patients (93 OB; 123 SFR)NICUMachry et al., 2023USAQualitative, ethnographic observational studyNICU families (20) and (30) healthcare staffTwo NICUsPickler et al., 2013USASecondary analysis87 preterm between 30–32 weeks gestationOB and SFR NICUPineda et al., 2017USAObservational longitudinal study58 preterm infants born at ≤ 28 weeksNICUPineda et al., 2014USAProspective longitudinal cohort study136 preterm infants born < 30 weeksNICUSilva et al., 2024BrazilComparative observational study40 preterm neonates20 in the Open-Bay NICU (OB NICU)20 in the Single-Family Room NICU (SFR NICU)NICUSmith et al., 2009USAMixed method studyNICU nursesNICUSolís-García et al., 2024SpainObservational and multi- centre study63 neonatal units in 17 Spanish Regions: 17 (27%) were IIIA, 35 (56%) were IIIB and 11 (17%) were IIIC.NICUSoni et al., 2022Qatar, Middle EAstDescriptive studyHealthcare staff, including nurses, physicians, advanced neonatal nurse practitioners, respiratory therapists, allied health professionalsNICUStevens et al., 2010USAComparative studyNICU staff, including nurses, neonatologists, nurse practitioners, clinical staff, non-clinical staff, pediatricians, and pediatric specialistsNICUTanberg et al., 2018NorwayCase control studyNICU patients (29SFR; 31 OB)OB and SFR NICUTandberg et al., 2019aNorwayCase control studyNICU parents (60 SFR, 72 OB)OB and SFR NICUTandberg et al., 2019bNorwayNICU patients (35 SFR; 42 OB) and parents (60SFR; 72 OB)NICUToivonen et al., 2017FinlandComparative observational study20 NICU nursesNICUvan der Hoeven et al., 2022The NetherlandsRetrospective cohort studyNICU patients (1433)NICUvan der Hoeven et al., 2023The NetherlandsRetrospective cohort studyNICU patients (OB 1236; SFR 777)NICUvan Veenendaal, 2020The NetherlandsRetrospective before-after study1046 NICU patients (468 SFR; 578 OB)NICUVohr et al., 2017USARetrospective cohort study691 Preterm infants weighing ≤ 1250 g at birth (394 OB, 297 SFR)NICUWatson et al., 2014CanadaDescriptive studyHealthcare NICU staff (171) and parents (173)NICUWielenga et al., 2025The NetherlandsObservational longitudinal cohort study833 dyads of parents and infants (365 were hospitalised in the OBU phase, 140 in the transition phase, and 328 in the SFR phase)NICUWinner-Stoltz et al., 2018USAProspective cohort study64 NICU staff RNs full-time, part-timeNICU
Table 3. Outcome for included studiesAuthor(s)(Year)Patient outcomeFamily outcomeStaff outcomeOrganizational outcomeCone et al., 2010xxxxDoede & Trinkoff, 2020xxDomanico et al., 2010xxxFay et al., 2023xxGrundt et al., 2021xxJoshi et al., 2018xKainiemi et al., 2021xxxxKudchadkar et al., 2016xxLester et al., 2014xxxXLester et al., 2016xxxMachry et al., 2023xxxPickler et al., 2013xPineda et al., 2017xxxPineda et al., 2014xxxSilva et al., 2024xxSmith et al., 2009xxSolis- Garcia, 2024xSoni et al., 2022xxxxStevens et al., 2010xxxxTanberg et al., 2018xxxTandberg et al., 2019axTandberg et al., 2019bxToivonen et al., 2017xxxxvan der Hoeven et al., 2022xxxXvan der Hoeven et al., 2023xxxxvan Veenendaal, 2020xxxxVohr et al., 2017xxxxWatson et al., 2014xxxWielenga et al., 2025xxWinner-Stoltz et al., 2018xx
Key findings from included studies
This review included 30 studies conducted between 2009 and 2025 across North America, Europe, the Middle East and one in South America. Included studies employed different methodologies, with prospective cohort and observational designs being most common, enabling assessment of clinical, developmental, and experiential outcomes over time [21–23]. Retrospective cohort studies were also frequently used to analyse existing clinical data [24–26]. Several studies adopted qualitative or ethnographic approaches to explore staff and parental experiences in depth [11, 27]. Mixed-method and pre-/post-designs combined surveys, observations, and interviews to evaluate changes before and after SFR implementation [28, 29]. Lastly, cross-sectional surveys provided snapshots of perceptions and satisfaction [8, 30]. Overall, the dominant use of cohort designs was complemented by qualitative insights, offering a comprehensive understanding of SFR impacts.
Study populations comprised NICU staff, parents, and preterm infants across both single-family room (SFR) and open-bay (OB) settings.
Outcomes were classified into four main domains: patient, family, staff, and organisation. Most studies reported improvements in patient outcomes—including neurodevelopment, breastfeeding, and reduced length of stay—in SFRs compared to OBs [21, 23, 26].
Single-family rooms (SFRs) in NICUs enhance neurodevelopmental outcomes and support family-centred care [8, 9, 30], offering greater privacy, improved parental involvement, and better environmental control [31, 32, 40, 41]. SFRs are associated with earlier breastfeeding [22], fewer alarms [24], improved sleep [15], shorter hospital stays [37], and enhanced cognitive outcomes [26]. Nurses report increased job satisfaction and efficiency [21, 28], though concerns about professional isolation and teamwork persist [28, 30, 33]. While infection rates are comparable, hand hygiene adherence is higher in SFRs [34], with fewer sepsis cases and catheter use [23]. Parents experience greater emotional support and involvement [32, 35], but nurse concerns about declining parental trust remain. Although concerns about sensory deprivation and delayed maturation exist [36], overall, SFRs contribute to better developmental care, workflow efficiency, and long-term cost-effectiveness [26, 31].
Patient outcomes
The SFR environment generally supports neonatal neurodevelopment by providing a quieter [40, 41], more controlled setting that reduces noise exposure [33, 36]. Infants in SFRs show improved sleep regulation and circadian rhythms [15], along with enhanced parent-infant closeness, privacy, skin-to-skin contact, communication with medical staff, and easier parental access [8, 29, 42] promoting parent-infant bonding, and contributing to more supportive developmental care [42].
Clinical outcomes are also improved in SFR settings. Infants experience shorter lengths of stay (LOS) and reduced mortality rates [23, 33], better growth including higher discharge weight and faster weight gain, earlier attainment of full enteral feeding at lower gestational ages, improved biobehavioral regulation and reduced stress levels [40]. They undergo fewer medical procedures, have lower sepsis incidence, and demonstrate improved neurobehavioral outcomes, such as reduced pain, stress, and hypertonicity [21]. Cognitive and language development at 18 months is enhanced, with a decreased risk of autism spectrum disorder symptoms [37]. Furthermore, exclusive breastfeeding rates at discharge and up to four months are higher in SFR infants [22].
However, some concerns remain. Infants in SFRs have shown reduced hemispheric asymmetry and delayed cerebral maturation on EEG, with lower language and motor scores at two years, possibly due to sensory deprivation in a less stimulating environment [36]. Infection control also requires attention, as cases of infection among twins suggest simultaneous acquisition rather than cross-transmission [34].
Parental involvement is significantly increased in SFRs, with mothers and fathers engaging in an additional eight and 37 h of skin-to-skin contact, respectively, over the hospital stay [32]. These factors contribute to enhanced patient safety and improved long-term neurodevelopmental outcomes [26, 31]. Overall, these findings support implementing SFRs in NICUs to optimize developmental, clinical, and psychosocial outcomes.
Family outcomes
SFRs in NICUs provide enhanced privacy, allowing families increased time with their infants and greater involvement in caregiving activities [11, 23, 29, 30, 33]. Parents report improved comfort and a heightened sense of environmental control within SFRs, which facilitates active participation in infant care [33, 42] contributing to reductions in parental stress and improved emotional outcomes [40]. However, the increased privacy inherent to SFRs may limit interparental communication and social interaction, potentially contributing to parental isolation [8, 33].
Quantitative data indicate significantly higher parental presence in SFRs, with mothers and fathers spending an additional 13 and 4 h per day at the bedside, respectively [12, 27, 32, 36]. This increased presence correlates with earlier initiation of milk expression and breastfeeding, supported by enhanced lactation resources and breastfeeding support programs [22, 26]. Maternal involvement in kangaroo care and feeding practices is also increased, accompanied by reductions in maternal stress and enhanced opportunities for skin-to-skin contact [21, 22, 36, 37, 40]. Fathers similarly benefit from increased skin-to-skin contact during the infant’s hospitalization [32].
Parental emotional well-being appears improved in SFR environments, with mothers reporting lower stress levels and decreased prevalence of depressive symptoms compared to those in open-bay units [9, 21, 35]. Environmental stressors such as noise and light exposure are also reduced in SFRs, further supporting parental mental health [38]. Enhanced parental engagement [42] fosters greater confidence in caregiving abilities and contributes to improved adjustment following discharge [9, 12]. Furthermore, SFRs facilitate improved communication between parents and healthcare providers, resulting in increased parental trust and involvement in clinical decision-making, although some nursing staff express concerns regarding diminished professional trust due to greater family autonomy [32].
Healthcare staff outcomes
SFRs contribute to a more structured and quieter work environment, which staff generally perceive as beneficial [30]. However, reduced peer interaction in SFRs often leads to feelings of isolation among staff, negatively affecting teamwork and collegial support [8, 28, 30]. Despite this, nurses acknowledge that SFRs enhance family-centred care (FCC) by enabling greater focus on individualized infant care and parental support [27, 30].
The emotional burden on nurses increases in SFRs, particularly when compensating for limited parental involvement, often due to social challenges, which can heighten stress levels [11, 33]. Nurses transitioning to SFRs initially report increased stress and concerns about patient safety but tend to experience improved job satisfaction over time [15, 21, 28, 33].
Overall, staff report higher job satisfaction in SFRs, with lower stress and reduced alarm fatigue contributing to better well-being [15, 24]. Nurses spend more time engaging with parents and providing lactation support, reinforcing their role in FCC. For example, in one study is reported that nurse-infant interaction increases from 119 to 166 min per shift and the number of interactions from 22 to 26 per shift in SFRs compared to open-bay (OB) units. Similarly, nurse-family interaction time rises from 35 to 117 min per shift, with interactions increasing from 8 to 13 per shift [12].
Challenges remain, including increased physical demands [27], communication difficulties with staff, and fewer opportunities for peer support [8, 33]. Conversely, some studies report improved physical work environments in SFRs, characterized by lower noise levels, greater privacy, fewer interruptions [31], and enhanced concentration [9]. Staff also express greater satisfaction with both physical and emotional aspects of the workspace [2].
SFRs positively influence infection control, with nurses demonstrating higher hand hygiene compliance [25]. Nonetheless, concerns about reduced teamwork and potential declines in trust-building between nurses and families persist [32].
Organizational outcomes
From an institutional perspective, SFRs offer multiple advantages, including enhanced infection control and increased compliance with hygiene protocols, which contribute to improved patient safety [25, 30]; Although concerns exist regarding multidrug-resistant organism (MDRO) colonization, evidence suggests these infections arise from external introduction rather than intra-unit transmission [34].
SFR implementation is associated with greater workflow efficiency, improved access to supplies, better workspace utilization [28], and more streamlined communication [25]. However, design elements can act as both facilitators and barriers to SFR effectiveness [27]. While transitioning to SFRs necessitates additional staff training, these environments ultimately enhance developmental care and support stronger adherence to FCC principles [12, 21, 31].
A key benefit of SFRs is the potential for reduced hospital costs. Shorter lengths of stay observed in infants cared for in SFRs lead to fewer medical interventions and lower healthcare expenses [23, 37]. Furthermore, improved developmental outcomes associated with SFRs may yield long-term cost savings by decreasing the need for future medical and educational services [26].
Despite these improvements in care quality and efficiency, SFRs have not been shown to significantly affect staff sick leave, turnover, or injury rates [9].
Discussion
This mixed-methods systematic review contributes to the growing body of evidence supporting the benefits of SFR designs in NICUs, while highlighting the paucity of research in PICU settings. Given the distinct clinical profiles and care demands of NICU versus PICU patients, this gap underscores an urgent need for studies assessing the impact of SFRs in older paediatric populations, staff workflows, and family engagement within high-acuity environments.
In line with previous research [2–4], our findings reinforce that SFRs promote family-centred care (FCC), enhance infant neurodevelopment, improve maternal and parental well-being, and optimize healthcare delivery. Enhanced parent-infant bonding, increased skin-to-skin contact, and earlier breastfeeding initiation were recurrently observed, affirming the critical role of parental presence in neonatal development [1, 6]. These improvements correlate with better clinical outcomes, including improved sleep regulation, reduced pain and stress responses, and shorter hospital stays [21, 26, 33]. From a developmental care standpoint, environmental regulation—through controlled light, sound, and minimized disruptions—emerges as central in supporting preterm infants’ physiological and neurological stability [36]. However, the review also echoes concerns from earlier work [4, 13] about the potential for sensory deprivation in highly isolated SFR environments due to reduced auditory and social stimulation. This has been associated with delayed cerebral maturation and lower language and motor scores at two years of age. These findings emphasize the need to carefully balance sensory exposure in SFRs—ensuring that the environment remains developmentally appropriate while minimizing harmful stimuli. Incorporating structured developmental stimulation programs may help address this balance and warrants further research.
From the staff perspective, SFRs are perceived to improve the physical work environment, reduce alarm fatigue, and facilitate enhanced family interactions, aligning with reported increases in job satisfaction and quality of care [2, 9]. Nevertheless, challenges remain, including increased emotional labour, feelings of isolation, and diminished team cohesion, especially when parental involvement is limited [11, 30]. These findings suggest that while SFRs support FCC principles, they may inadvertently hinder staff collaboration unless supplemented by organizational interventions such as team-building initiatives, peer support mechanisms, and targeted training programs.
Organizationally, evidence indicates improved workflow efficiency, better infection control adherence, and reduced costs linked to shorter lengths of stay in SFR units, corroborating prior claims of operational benefits associated with SFR implementation [5, 7]. While concerns about multidrug-resistant organism (MDRO) colonization persist, current data suggest colonization primarily arises from community rather than in-unit transmission [34]. Effective infection control practices and staff adherence to hygiene protocols remain critical components of successful SFR adoption.
Equity considerations also emerge as essential. Socioeconomic factors significantly influence parental presence and engagement, affecting both infant developmental outcomes and parental well-being [26]. Future research should explore how institutional policies—such as provision of housing, transportation assistance, and parental leave—can mitigate disparities and ensure equitable access to SFR benefits. Broader inclusion of diverse caregiver populations, including those facing cultural, linguistic, or systemic barriers, is also critical. Moreover, it is plausible that infants whose parents are unable to be present in SFRs due to personal, social, or structural constraints may experience fewer benefits from family-centred care. To mitigate the risk of widening disparities, healthcare institutions might consider implementing strategies such as enhanced nursing presence or structured care programmes to ensure consistent developmental and emotional support. Further research is needed to explore how best to safeguard equitable care experiences for this potentially vulnerable subgroup.
Advancements in technology and artificial intelligence (AI) hold promise for mitigating some of the structural and interpersonal challenges associated with SFR designs. AI-driven monitoring systems could reduce alarm fatigue by providing more precise and context-aware alerts, allowing nurses to focus their attention more efficiently [24]. Telehealth platforms and digital communication tools may facilitate improved collaboration and information sharing among dispersed staff members, helping to overcome the isolation and reduced peer interaction inherent in SFR layouts [28]. Additionally, AI-enabled predictive analytics could support individualized patient care planning, enhancing developmental care and parental involvement by providing real-time decision support tailored to each infant’s needs. These technologies could also empower families through remote access to care teams and educational resources, further strengthening FCC. However, successful integration of such innovations requires thoughtful implementation strategies, including training and workflow redesign, to ensure that technology complements rather than complicates the caregiving environment.
While the SFR model represents a significant advance in delivering developmentally sensitive, family-centred care, its optimal implementation requires coordinated structural, emotional, and organizational support. Future research, particularly in PICU settings, alongside interventions targeting staff collaboration and equity, is essential to maximize the benefits of SFR designs across paediatric intensive care environments.
Limitation
A notable limitation of this review is the heterogeneity across included studies, encompassing variations in design, populations, outcomes, and reporting styles. This diversity precluded meta-analytic synthesis and limits causal inference. Additionally, the language restriction to English, Italian, and Spanish may have omitted pertinent evidence from other linguistic contexts. Furthermore, the predominance of observational study designs underscores the need for high-quality randomized controlled trials to strengthen the evidence base.
Conclusions
The shift from open-bay to SFRs NICUs offers clear benefits, notably increased parental presence and engagement linked to improved infant neurodevelopment and reduced parental stress [21, 26, 29, 32, 35, 37]. However, these gains do not always result in significant clinical improvements [25]. While SFRs support earlier developmental milestones [21, 22], reduced auditory stimulation raises concerns about sensory exposure [13, 36]. Infection rates show little change after transitioning to SFRs [34].
Staff report better work environments and communication but face increased emotional demands and mixed effects on workflow efficiency [8, 11, 28]. Physical design influences staff responsiveness and alarm management, though improvements in care quality are not uniform [24, 39].
Overall, SFRs enhance family-centred care but present complex challenges. Future research should focus on refining NICU design and care models to balance infant development, parental involvement, staff well-being, and operational efficiency. Additionally, exploring technological innovations and targeted support strategies may help overcome current limitations and maximize the benefits of SFR environments.
These findings are relevant for healthcare planners and clinical leaders aiming to enhance family-centred care, staff well-being, and developmental outcomes in intensive care contexts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1European Foundation for the Care of Newborn Infants. The NICU of the future: design meets function [Internet]. 2019. Available from: https://www.efcni.org/news/the-nicu-of-the-future-design-meets-function
- 2Meredith JL, Jnah A, Newberry D. The NICU environment: infusing single-family room benefits into the open-bay setting. Neonatal Netw. 2017;36(2):69–76. Available from: 10.1891/0730-0832.36.2.6910.1891/0730-0832.36.2.6928320493 · doi ↗ · pubmed ↗
- 3White RD, Consensus Committee on Recommended Design Standards for Advanced Neonatal Care. Recommended standards for newborn ICU design, 9th edition. J Perinatol. 2020;40(Suppl 1):2–4. Available from: 10.1038/s 41372-020-0766-210.1038/s 41372-020-0766-232859957 · doi ↗ · pubmed ↗
- 4Alsadaan N, Ramadan OME, Alqahtani M, Shaban M, Elsharkawy NB, Abdelaziz EM, et al. Impacts of integrating family-centered care and developmental care principles on neonatal neurodevelopmental outcomes among high-risk neonates. Children (Basel). 2023;10(11):1751. Available from: 10.3390/children 1011175110.3390/children 10111751 PMC 1067063738002842 · doi ↗ · pubmed ↗
- 5Ortenstrand A, Westrup B, Broström EB, Sarman I, Akerström S, Brune T, et al. The Stockholm neonatal family-centered care study: effects on length of stay and infant morbidity. Pediatrics. 2010;125(2):e 278–85. Available from: 10.1542/peds.2009-151110.1542/peds.2009-151120100748 · doi ↗ · pubmed ↗
- 6Doede M, Trinkoff AM. Emotional work of neonatal nurses in a single-family room NICU. J Obstet Gynecol Neonatal Nurs. 2020;49(3):283–92. Available from: 10.1016/j.jogn.2020.03.00110.1016/j.jogn.2020.03.00132298637 · doi ↗ · pubmed ↗
- 7Johanna Briggs Institute. JBI critical appraisal tools [Internet]. Available from: https://jbi.global/critical-appraisal-tools
- 8Grundt H, Tandberg BS, Flacking R, Drageset J, Moen A. Associations between single-family room care and breastfeeding rates in preterm infants. J Hum Lact. 2021;37(3):593–602. Available from: 10.1177/089033442096270910.1177/0890334420962709 PMC 841482033035125 · doi ↗ · pubmed ↗