Levosimendan in Decompensated Heart Failure with Reduced Ejection Fraction in Older Adults: A Systematic Review of Safety and Efficacy
Esteban Zavaleta-Monestel, Jeaustin Mora-Jiménez, Kevin Cruz-Mora, Ernesto Martinez-Vargas, José Pablo Díaz-Madriz, Sebastián Arguedas-Chacón, Abigail Fallas-Mora, Carlos Wu-Chin, Jose Miguel Chaverrí-Fernandez

TL;DR
This paper reviews whether levosimendan is safe and effective for treating heart failure in older adults.
Contribution
It provides a systematic review of levosimendan's efficacy and safety in older patients with decompensated heart failure.
Findings
Levosimendan improved short-term hemodynamic parameters like cardiac index and pulmonary capillary wedge pressure.
No significant differences in mortality or rehospitalization rates were observed.
Adverse events included hypotension and atrial arrhythmias, but treatment discontinuation was low.
Abstract
Background/Objectives: Heart failure with reduced ejection fraction (HFrEF) is a leading cause of hospitalization and functional decline in older adults, accounting for over 80% of all heart failure cases. Given the narrow therapeutic window of currently available inotropes and the vulnerability of this population, levosimendan has been proposed as a potential alternative. This systematic review aimed to evaluate the clinical efficacy and safety of levosimendan in older adults with decompensated HFrEF. Methods: A systematic search of PubMed, Embase, Scopus, and the Cochrane Library was conducted between January and May 2025, following PRISMA 2020 guidelines. The review was registered in PROSPERO (CRD420251032329). Of 379 articles initially identified, 8 studies (randomized, observational, and single-arm designs) enrolling patients aged ≥65 years with decompensated HFrEF met the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
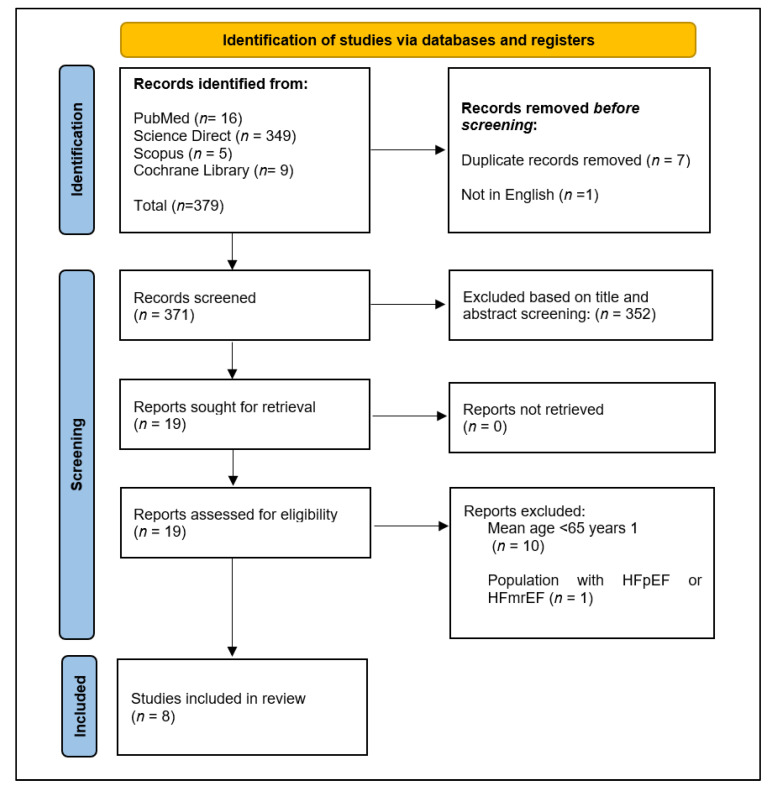 Figure 1
Figure 1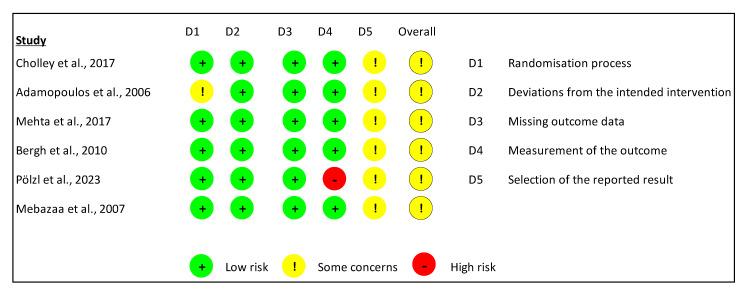 Figure 2
Figure 2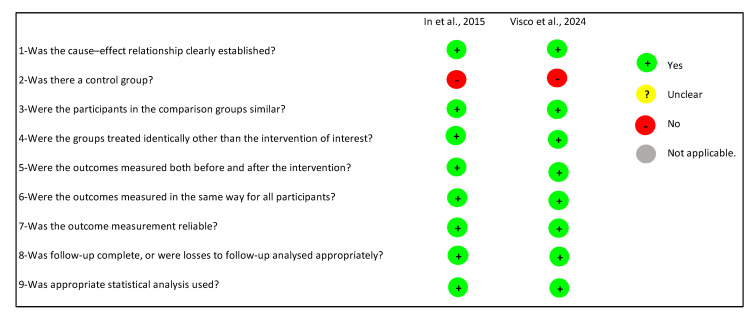 Figure 3
Figure 3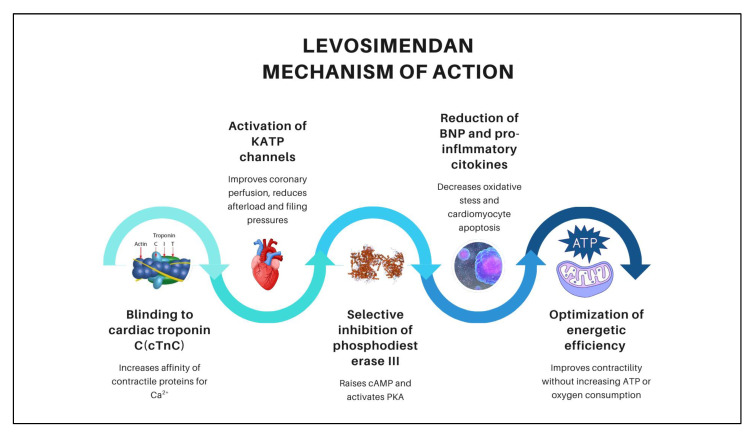 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Cardiovascular Function and Risk Factors · Cardiac, Anesthesia and Surgical Outcomes
1. Introduction
Heart failure (HF) is a clinical syndrome characterized by the heart’s inability to pump blood efficiently to meet the body’s metabolic demands. It is classified according to left ventricular ejection fraction (LVEF) into reduced, preserved, or mildly reduced categories, and by clinical presentation as acute or chronic [1]. In heart failure with reduced ejection fraction (HFrEF), LVEF is <40%, and patients often experience symptoms refractory to optimal medical therapy, recurrent episodes of decompensation, functional decline, and high hospitalization rates [2].
HFrEF predominantly affects older adults, with over 80% of cases occurring in individuals aged ≥65 years and an incidence close to 10 per 1000 persons per year. Its progression is often accompanied by hemodynamic deterioration and neurohormonal activation, leading to common comorbidities such as renal insufficiency, chronic obstructive pulmonary disease (COPD), and anemia. Moreover, currently available inotropic agents have a narrow therapeutic window and carry a substantial risk of arrhythmias, further complicating pharmacological management in this population [2].
The use of levosimendan in older adults requires a carefully individualized clinical approach due to their increased susceptibility to hemodynamic and arrhythmic adverse events. In patients with acute or decompensated HF, levosimendan has been shown to improve clinical stability and hemodynamic parameters without significantly increasing the incidence of serious complications. Nevertheless, administration should always be accompanied by close monitoring to ensure safety [3,4].
Although current evidence offers a general understanding of HFrEF management, it remains insufficient to guide therapy specifically in older adults. Therefore, this systematic review aims to evaluate the impact of levosimendan in patients aged ≥65 years with decompensated HFrEF, comparing it with standard care—either without inotropes or with alternative inotropic agents—and analyzing outcomes related to efficacy (hemodynamic function, mortality, rehospitalization) and safety (symptomatic hypotension, arrhythmias).
2. Methods
This systematic review was conducted following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [5]. Additional details, including the PRISMA 2020 Checklist and the full search strategies for each database, are provided in the Supplementary Materials.
2.1. Protocol Registration
The protocol was registered in the PROSPERO database (International Prospective Register of Systematic Reviews) under registration number CRD420251032329. The full registration record is publicly available at: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251032329 (accessed on 16 September 2025).
2.2. Search Strategy
A comprehensive search was performed in PubMed, MEDLINE, Embase, Scopus, and the Cochrane Library to identify relevant studies evaluating levosimendan in older adults with decompensated heart failure with reduced ejection fraction (HFrEF).
The search strategy combined controlled vocabulary (MeSH terms) and free-text terms with Boolean operators (AND, OR) to maximize sensitivity. The keywords included: “Levosimendan”, “Simdax”, “Heart Failure, Systolic”, “Heart Failure with Reduced Ejection Fraction”, “HFrEF”, “Older Adults”, “Elderly”, “Geriatric Patients”, “Patients over 65 years”, “Clinical Trial”, “Randomized Controlled Trial”, “Observational Study”, “Hemodynamics”, “Cardiac Output”, and “Left Ventricular Function”. Searches were restricted to articles published between January 2005 and May 2025. The detailed search strategies for each database are provided in Appendix A.
2.3. Eligibility Criteria
This systematic review was conducted in accordance with the PRISMA statement and structured around the PICO question. Older adults with heart failure with reduced ejection fraction (HFrEF) were included as the population (P), assessing the administration of levosimendan (I) in comparison with other pharmacological treatments such as dobutamine, milrinone, or no inotropes (C). The outcomes analyzed (O) were improvement in cardiac function, reduction in mortality, hospitalizations, and adverse events. The research question posed was: In older adults with HFrEF, does levosimendan improve clinical outcomes compared to standard treatment?
2.3.1. Inclusion Criteria
Articles written entirely in English and published within the last 20 years were selected, including patients with decompensated heart failure with reduced ejection fraction (HFrEF). Studies with participants over 18 years of age were accepted, provided the population was representative of a geriatric profile, defined as having a mean age of 65 years or older. The search was limited to clinical trials, analytical observational studies, systematic reviews, and meta-analyses.
2.3.2. Exclusion Criteria
Studies that did not specify the age of participants were excluded. Additionally, studies involving patients with heart failure with preserved ejection fraction (HFpEF), as well as those with incomplete or inaccessible data, were also excluded. Any discrepancies between reviewers were resolved by a third investigator through analysis and discussion.
2.4. Study Selection and Documentation
Two reviewers independently screened titles and abstracts for eligibility. Full texts of potentially relevant studies were retrieved and assessed against the inclusion criteria. Reference lists of selected articles and relevant reviews were manually screened to identify additional eligible studies. Any disagreements were resolved through discussion with a third reviewer
2.5. Risk of Bias
Data collection was carried out using a predesigned table developed before evaluating the selected articles. Two independent reviewers assessed the methodological quality of the eligible studies and reached a consensus. For randomized clinical trials, the Cochrane Risk of Bias Tool (RoB-2) was used, which evaluates seven domains related to study design, conduct, and reporting. For non-randomized studies (observational and single-arm), the Joanna Briggs Institute (JBI) Critical Appraisal Tool was applied, using the appropriate version to each study design. Any discrepancies between reviewers were resolved by consensus or with the intervention of a third evaluator.
3. Results
3.1. Study Selection
Figure 1 illustrates the study selection process. A total of 379 records were initially identified through comprehensive searches in PubMed (n = 16), ScienceDirect (n = 349), Scopus (n = 5), and the Cochrane Library (n = 9). Before screening, 7 duplicate records were removed, along with 1 article written in a language other than English, resulting in 371 unique records for title and abstract screening. During this phase, 352 records were excluded because they did not meet the predefined eligibility criteria, which included population characteristics, study design, and relevance to the research question. Nineteen full-text articles were subsequently retrieved and assessed for eligibility. Of these, 10 were excluded because the mean age of participants was below 65 years, and 1 was excluded because the study population comprised patients with heart failure with preserved ejection fraction (HFpEF) or heart failure with mildly reduced ejection fraction (HFmrEF), conditions outside the scope of the review. Consequently, 8 studies fulfilled all inclusion criteria and were incorporated into the final systematic review.
3.2. Characteristics of the Included Studies
Table 1 summarizes the clinical characteristics and main outcomes of the included studies. Eight studies were included, comprising predominantly randomized controlled trials, along with one observational study and one single-arm interventional study. The populations evaluated varied, including older adults with decompensated HFrEF as well as patients undergoing cardiac surgery with reduced LVEF. Interventions assessed levosimendan either in comparison with standard care, placebo, or alternative inotropes such as dobutamine. Outcomes spanned hemodynamic parameters (cardiac index, pulmonary capillary wedge pressure), clinical endpoints (all-cause mortality, rehospitalization), and safety events (hypotension, arrhythmias). Given the heterogeneity in study designs, populations, and outcome measures, no meta-analysis was performed, and results are presented descriptively without pooled quantitative synthesis.
3.3. Primary Outcomes
3.3.1. Mortality and Hospitalization
As shown in Table 2, studies on HFrEF do not demonstrate clear mortality benefits from levosimendan. Mebazaa et al. (2007) [7], Cholley et al., 2017 [10] and Mehta et al., 2017 [11] found no significant differences in survival at 30, 90, or 180 days, nor in comparisons at 28 and 180 days (p values between 0.12 and 0.59). In García-González et al. (2015) [9] reported a 75% 30-day survival rate following aortic valve replacement; however, the lack of a control group and insufficient statistical power preclude attributing this outcome to the drug.
Following discharge, Pölzl et al. (2023) [12] also found no reduction in decompensation events through week 14 (p = 0.064), and even recorded a higher number of cardiovascular events in the levosimendan arm. Lastly, Visco et al. (2024) [13] reported a 50% reduction in hospitalizations and a 68% decrease in inpatient days using CardioMEMS and on-demand levosimendan administration; however, the absence of statistical validation and the small sample size limit the reliability of these findings.
3.3.2. Cardiac Function and Hemodynamics
As shown in Table 2, Levosimendan may exert an acute and sustained effect on hemodynamic parameters in older adults with HFrEF. For instance, Adamopoulos et al. 2006 [6] reported that, following a single 72 h infusion of levosimendan, pulmonary capillary wedge pressure (PCWP) decreased from 24 ± 3 to 19 ± 2 mmHg, cardiac index (CI) increased from 1.7 ± 0.4 to 1.9 ± 0.5 L/min/m^2^, and left ventricular ejection fraction (LVEF) improved from 24 ± 5% to 28 ± 6% (p < 0.05 for all parameters).
Similarly, Bergh et al. (2010) [8] observed at 48 h a reduction in PCWP of 8.3 ± 6.7 mmHg and an increase in CI of 0.66 ± 0.63 L/min/m^2^; they also reported a mean decrease in NT-proBNP of 507 ng/mL (p ≤ 0.05). Likewise, In et al. (2015) [9] found that at 24 h, CI increased from 1.65 ± 0.20 to 2.37 ± 0.49 L/min/m^2^, PCWP dropped from 31 ± 10 to 16 ± 4 mmHg, and stroke volume index (SVI) rose from 21.1 ± 7.1 to 30.1 ± 7.4 mL/m^2^ (p ≤ 0.002 in all cases), findings are consistent with a vasodilatory and inotropic profile.
3.4. Secondary Outcomes
3.4.1. Adverse Events (AE)
As shown in Table 3, hypotension was the most frequently reported adverse effect with levosimendan, affecting 35–57% of patients compared to 7–48% in the comparator groups [8,9,10,12]. Arrhythmias, particularly atrial fibrillation (AF), were observed in a wide range (9–50% vs. 6–40%), although several studies did not show significant differences [8,11,12]. Other events such as hypokalemia (6–9%), headache (5–8%), third-degree atrioventricular block (4% vs. 9%), or stroke (2.4–3.5%) were infrequent, indicating an overall acceptable tolerability profile, except for the need to monitor blood pressure and heart rhythm closely [7,10,11].
3.4.2. Treatment Discontinuations
As shown in Table 3, levosimendan discontinuation due to adverse events was infrequent, occurring in 5% to 8% of treated patients compared to 3–4% in control groups (Cholley et al., 2017 [10] Mehta et al., 2017 [11], with no statistically significant differences in patients undergoing cardiopulmonary bypass surgery. The fact that other studies did not report discontinuation rates further supports the overall acceptable tolerability of the drug, despite the incidence of hypotension and arrhythmias.
3.5. Methodological Quality
3.5.1. Assessment Using the ROB-2 Tool
Two reviewers (J.M-J and K.C-M) independently assessed the risk of bias and study quality. Figure 2 presents the evaluation of six randomized clinical trials using the RoB-2 tool. All studies appropriately managed deviations from the intended interventions and missing outcome data (Domains D2–D3). However, Adamopoulos et al. [6] showed weaknesses in the randomization process (D1), and Pölzl et al. [12] raised concerns regarding the reliability of outcome measurements (D4). Additionally, all studies presented inconsistencies in the selection of reported outcomes (D5). Consequently, each trial received a global judgment of moderate risk of bias, which may reduce the overall confidence in the findings.
3.5.2. Evaluation Using the JBI Critical Appraisal Tool
In Section 3.5.2, two reviewers (J.M.-J. and K.C.-M.) applied for the JBI Critical Appraisal Tool for Quasi-Experimental Studies, which includes nine domains to assess methodological quality. Based on these criteria, no study received a score indicative of low quality (0–4 domains), while both articles were rated as high quality, fulfilling between 5 and 9 domains. Details of these assessments are presented in Figure 3.
3.6. Summary of Findings for the Prespecified Outcomes and Certainty of the Evidence (GRADE)
As shown in Table 4, the evidence synthesis indicates that levosimendan, compared with standard care without inotropes or with alternative inotropes, probably results in a small to no difference in mortality (low certainty) and may be associated with a slight increase in hypotension (moderate certainty). The effect on arrhythmias is uncertain, with a possible small to no difference (low certainty). Levosimendan probably reduces pulmonary capillary wedge pressure (moderate certainty) but shows little to no effect on cardiac index at 48 h (moderate certainty). For hospitalization outcomes, the evidence is very uncertain (very low certainty) due to reliance on a single observational study at high risk of bias and potential confounding. Hemodynamic outcomes from a single observational study with nine participants were not included in the SoF table due to very low certainty and limited applicability; these results are described narratively in the main text.
4. Discussion
4.1. Effectiveness of Levosimendan in Decompensated Heart Failure in Older Adults
4.1.1. Mortality and Hospitalizations
Several studies in geriatric and surgical populations have assessed the impact of levosimendan on mortality, yielding inconsistent results. In older adults with HFrEF, Mebazaa et al. (2007) and Pölzl et al. (2023), after propensity score adjustment in critically ill patients, reported no significant differences at 30, 90, or 180 days (p > 0.05) [7,12,14]. In patients undergoing cardiopulmonary bypass surgery, Cholley et al. (2017) and Mehta et al. (2017) also found no mortality benefit. Conversely, a meta-analysis by Landoni et al. (2018) demonstrated a significant reduction in perioperative mortality following CABG (RR 0.45; 95% CI: 0.29–0.71; p = 0.0005), but no effect in patients undergoing valvular surgery (RR 0.64; 95% CI: 0.12–3.38; p = 0.60) [10,11,15]. These discrepancies may be explained by differences in study design, patient heterogeneity, and variations in drug administration protocols
Although evidence in older adults with decompensated heart failure does not consistently show a benefit in reducing rehospitalizations [12]. The literature is generally heterogeneous. A meta-analysis of 45 randomized trials (n = 5480) reported that levosimendan reduced hospital length of stay by –1.31 days (95% CI: –1.95 to –0.31; p = 0.007), although substantial heterogeneity was observed (I^2^ = 71%) [16]. Overall, these findings suggest that while levosimendan may shorten hospital stays, its effects on mortality and rehospitalizations remain inconsistent, and its use should be individualized based on each patient’s clinical profile.
4.1.2. Hemodynamic Effects
In older adults, levosimendan exhibits both vasodilatory and inotropic properties, leading to measurable improvements in PCWP, CI, LVEF, and NT-proBNP levels, sustained for periods ranging from 24 to 72 h [6,8,9]. These results are consistent with evidence from several meta-analyses showing that both inpatient and outpatient infusions are associated with an approximate increase in cardiac output of 0.6–0.7 L/min/m^2^, along with improvements in multiple hemodynamic markers. Notably, in post-surgical patients, these hemodynamic benefits may persist for up to 7 days [17,18].
The hemodynamic benefits of levosimendan in improving cardiac performance and myocardial perfusion arise from five synergistic mechanisms of action, as illustrated in Figure 4. First, it binds to cardiac troponin C (cTnC), increasing the affinity of contractile proteins for Ca^2+^, thereby enhancing inotropy without elevating myocardial oxygen consumption or intracellular calcium levels [19]. Second, it activates adenosine triphosphate (ATP)-sensitive potassium (KATP) channels in the sarcolemma of vascular smooth muscle, improving coronary perfusion, reducing afterload, and lowering filling pressures. Simultaneously, activation of mitochondrial KATP channels exerts cardioprotective, anti-ischemic, anti-inflammatory, and anti-apoptotic effects [20]. Third, selective inhibition of phosphodiesterase III in the myocardium increases cyclic adenosine monophosphate (cAMP) levels, activates protein kinase A (PKA), and induces phosphorylation of L-type calcium channels and phospholamban, enhancing both calcium influx during action potentials and its reuptake into the sarcoplasmic reticulum—producing potent inotropic and lusitropic effects [21].
Additionally, levosimendan reduces circulating levels of brain natriuretic peptide (BNP) and pro-inflammatory cytokines, attenuates oxidative stress, and prevents cardiomyocyte apoptosis. By optimizing contractility without increasing ATP consumption or oxygen demand, it enhances energetic efficiency and consolidates its therapeutic value in the management of decompensated heart failure in older adults [22].
4.2. Security of Levosimendan in Decompensated Heart Failure in Older Adults
4.2.1. Tolerability and Adverse Effects of Levosimendan in Decompensated Heart Failure in Older Adults
When administering levosimendan to older adults, potential adverse reactions must be carefully anticipated and monitored. Across the reviewed studies, hypotension emerged as the most frequent adverse event, reported in 36–57% of patients [8,10,11]. In the REVIVE II trial, which included patients aged ≥65 years hospitalized for acute decompensated heart failure, hypotension occurred in 50.2% of participants and was the leading cause of treatment discontinuation [23].
The second most common adverse event was arrhythmia, particularly atrial fibrillation and ventricular tachycardia, with incidence rates ranging from 9% to 50% [8,12,15]. Some studies reported atrial fibrillation in up to 14% of patients, noting that most episodes were brief and clinically manageable [24]. Additional adverse events—including headache, nausea, hypokalemia, and stroke—were infrequent. Overall, while the incidence of serious adverse events in this population is relatively low, close hemodynamic and electrocardiographic monitoring is warranted throughout treatment [25].
4.2.2. Considerations and Precautions for the Use of Levosimendan in Decompensated Heart Failure in Older Adults
In advanced heart failure with reduced ejection fraction (advHFrEF), levosimendan may be considered as a palliative intervention or as a strategy for transient hemodynamic improvement in cases with clinical or hemodynamic evidence of organ hypoperfusion. The initial infusion should be administered in a hospital setting, starting at 0.2 µg/kg/min over 24 h, to ensure safety and detect potential complications such as symptomatic hypotension or ventricular tachycardia. For palliative use, clinical benefit is primarily assessed through subjective improvement in symptoms and quality of life, which can be complemented by reductions in NT-proBNP levels. In cases aimed at optimizing hemodynamics before advanced therapies (e.g., LVAD implantation), assessment may include echocardiography or right heart catheterization [19].
In patients with systolic blood pressure > 100 mmHg and mildly reduced renal function (estimated glomerular filtration rate [eGFR] > 45 mL/min/1.73 m^2^), intermittent dosing of 6.25 mg every two weeks is suggested. In those with systolic blood pressure < 100 mmHg, significantly impaired renal function (eGFR < 45 mL/min/1.73 m^2^), or a history of complex ventricular arrhythmias, the regimen should be adjusted to 12.5 mg every four weeks [26].
In patients scheduled for LVAD implantation, levosimendan should be administered 24 h before surgery at 0.2 µg/kg/min, with the addition of norepinephrine or epinephrine (0.1–0.2 µg/kg/min) if the risk of post-implant right ventricular dysfunction is high. Dosing should be individualized according to the patient’s clinical profile and treatment response, with close monitoring due to the increased risk of adverse effects in older adults with multiple comorbidities [27].
4.2.3. Practical Precautions and Titration Guidelines for Levosimendan in Geriatric Decompensated Heart Failure
Levosimendan can be administered at doses ranging from 0.05 to 0.2 µg/kg/min over 24 h. Although traditionally preceded by a 6–12 µg/kg bolus, the use of a loading dose is no longer routinely recommended in clinical practice due to safety concerns. The most commonly employed regimen is a continuous infusion of 0.1 µg/kg/min without a bolus, as loading doses are associated with a higher risk of hypotension and arrhythmias, particularly in frail, hypovolemic, or hypotensive patients [28].
Current best practice favors starting the infusion at the target rate and adjusting gradually based on the patient’s hemodynamic response. The total infusion volume typically ranges from 3 to 12 mL, depending on dose and body weight. A slow, individualized titration is advised to minimize the risk of hypotension [28].
For preparation, one vial containing 12.5 mg (5 mL) of levosimendan should be diluted in 250 mL of 5% dextrose solution. Alternatively, two vials (25 mg total) can be diluted in 500 mL of the same diluent. Using 5% dextrose is essential to maintain solubility and chemical stability, preventing precipitation and infusion-related reactions. Other diluents, such as saline or Ringer’s lactate, are not recommended due to an increased risk of drug instability or precipitation [10,28].
4.3. Strengths and Limitations
This systematic review has several strengths, including a comprehensive and reproducible search strategy across multiple databases, adherence to PRISMA 2020 guidelines, and the use of validated tools (RoB-2 and JBI) for quality assessment. The inclusion criteria ensured a focus on older adults (mean age ≥65 years), addressing a clinically relevant but often underrepresented population in heart failure research.
However, important limitations must be acknowledged. The evidence base is limited by the small number of studies specifically designed for older adults with HFrEF, and the substantial heterogeneity in study design, patient populations, intervention protocols, and outcome measures precluded meta-analysis. Most trials were not powered to detect differences in hard clinical outcomes such as mortality or rehospitalization, and several presented moderate risk of bias, particularly regarding allocation concealment, blinding, and selective reporting. The certainty of the evidence for several key outcomes was downgraded due to imprecision and indirectness.
These limitations restrict the generalizability of the findings and make the interpretation of results inherently cautious. Larger, multicenter, randomized controlled trials specifically designed for the geriatric HFrEF population are needed to clarify the potential role of levosimendan, particularly for clinical endpoints beyond transient hemodynamic improvement.
5. Conclusions
The use of levosimendan has not shown a consistent effect on survival in older adults with decompensated HFrEF at 30, 90, or 180 days. Additionally, no clear reduction was observed in rehospitalization rates or hospital length of stay in this population. However, the results suggest potential hemodynamic benefits from 24 to 72 h after administration, particularly in patients undergoing surgical intervention.
On the other hand, the most frequently reported adverse event was hypotension, occurring in up to 57% of cases. Transient arrhythmias such as atrial fibrillation and supraventricular tachycardia (SVT) were also observed; although manageable, these require close monitoring. Other adverse events were infrequent, but their occurrence in a clinically fragile population supports the need for rigorous monitoring.
Overall, this review provides relevant evidence for geriatric clinical practice by showing that although levosimendan does not appear to improve survival or reduce hospitalizations in older adults with HFrEF, it might have a role in selected clinical scenarios, such as palliative care as a potential action for transient hemodynamic improvement. However, this potential use should be interpreted with caution given the lack of consistent benefit in clinical outcomes. Its administration should occur in a hospital setting, with appropriate monitoring and individualized dose adjustments based on blood pressure and renal function.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uchmanowicz I. Nessler J. Gobbens R. Gackowski A. Kurpas D. Straburzynska-Migaj E. Kałuzna-Oleksy M. Jankowska E.A. Coexisting Frailty with Heart Failure Front. Physiol.20191079110.3389/fphys.2019.0079131333480 PMC 6616269 · doi ↗ · pubmed ↗
- 2Zhou S. Li D. Zhang L. Li J. The Anti-Inflammatory and Haemodynamic Effects of Levosimendan on Advanced Heart Failure Patients: A Meta-Analysis of Published Studies J. Int. Med. Res.202351300060522114840210.1177/0300060522114840237490021 PMC 10387701 · doi ↗ · pubmed ↗
- 3Zhang D. Yao Y. Qian J. Huang J. Levosimendan Improves Clinical Outcomes of Refractory Heart Failure in Elderly Chinese Patients Med. Sci. Monit. Int. Med. J. Exp. Clin. Res.2015212439244510.12659/MSM.893580 PMC 454870126289557 · doi ↗ · pubmed ↗
- 4Kirlidis T.T. Skoularigis J. Tsaknakis K.T. Karayiannis G. Tsaknakis T.K. Triposkiadis F. The Influence of Beta-Blockade on the Hemodynamic Effects of Levosimendan in Elderly (>= 70 Years) Patients with Acutely Decompensated Systolic Heart Failure Int. J. Clin. Pharmacol. Ther.20094745445910.5414/CPP 4745419640352 · doi ↗ · pubmed ↗
- 5Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews BMJ 2021372 n 7110.1136/bmj.n 7133782057 PMC 8005924 · doi ↗ · pubmed ↗
- 6Adamopoulos S. Parissis J.T. Iliodromitis E.K. Paraskevaidis I. Tsiapras D. Farmakis D. Karatzas D. Gheorghiade M. Filippatos G.S. Kremastinos D.T. Effects of Levosimendan versus Dobutamine on Inflammatory and Apoptotic Pathways in Acutely Decompensated Chronic Heart Failure Am. J. Cardiol.20069810210610.1016/j.amjcard.2006.01.06816784930 · doi ↗ · pubmed ↗
- 7Mebazaa A. Nieminen M.S. Packer M. Cohen-Solal A. Kleber F.X. Pocock S.J. Thakkar R. Padley R.J. Põder P. Kivikko M. Levosimendan vs Dobutamine for Patients with Acute Decompensated Heart Failure: The SURVIVE Randomized Trial JAMA 20072971883189110.1001/jama.297.17.188317473298 · doi ↗ · pubmed ↗
- 8Bergh C.-H. Andersson B. Dahlström U. Forfang K. Kivikko M. Sarapohja T. Ullman B. Wikström G. Intravenous Levosimendan vs. Dobutamine in Acute Decompensated Heart Failure Patients on Beta-Blockers Eur. J. Heart Fail.20101240441010.1093/eurjhf/hfq 03220335355 PMC 2844760 · doi ↗ · pubmed ↗