Perceived Decline in Straight Blade Direct Laryngoscopy Skills in the Era of Video Laryngoscopy: An Exploratory Pilot Survey Study
Lawrence W Chinn, Myriam Lin, Dhvani Shihora

TL;DR
This study explores how the increasing use of video laryngoscopy may be reducing opportunities to practice direct laryngoscopy skills among anesthesiologists.
Contribution
It is the first exploratory pilot study to assess perceived skill decline in direct laryngoscopy due to video laryngoscopy reliance.
Findings
Residents reported low confidence and infrequent use of the Miller blade for direct laryngoscopy.
Confidence in direct laryngoscopy strongly correlated with frequency of use.
Attendings acknowledged the importance of direct laryngoscopy but noted limited teaching and a risk of it becoming a 'lost art.'
Abstract
Background Video laryngoscopy is increasingly used for airway management and is often chosen for both routine and complex intubations. While video laryngoscopy offers clear advantages, direct laryngoscopy remains an important fallback technique when visualization is impaired or equipment fails. As video laryngoscopy becomes more common, questions have been raised about whether reliance on this technology may reduce opportunities for trainees to practice and maintain direct laryngoscopy skills. Methods We conducted a cross-sectional survey of anesthesiology residents and attending anesthesiologists at a single academic institution. The survey assessed self-reported confidence using the Miller blade, frequency of use, perceived importance of maintaining this skill, and beliefs about the effectiveness of current teaching practices. Responses were recorded using a 1-5 Likert scale.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
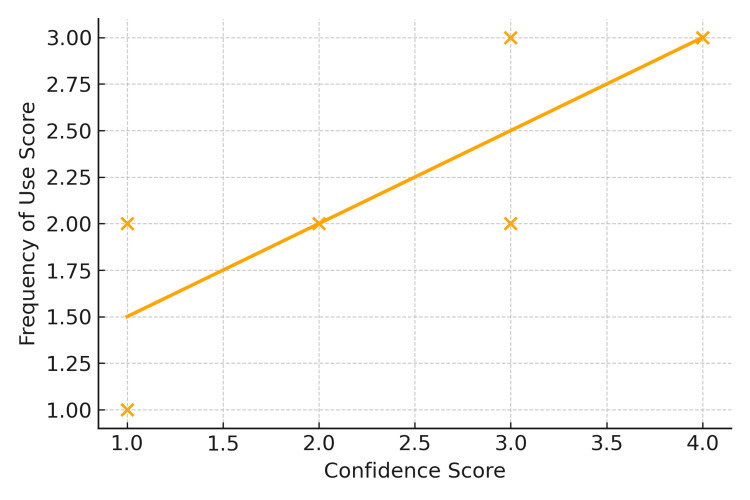 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Voice and Speech Disorders · Tracheal and airway disorders
Introduction
Video laryngoscopy (VL) has become a cornerstone of modern airway management. Initially introduced for difficult airways, VL is now routinely used across a range of clinical scenarios, from high-risk intubations to standard elective cases. Randomized trials demonstrate that VL improves glottic visualization and first-pass success, even in patients without predicted airway difficulty [1-6]. Additional studies confirm its advantages in patients with cervical spine immobilization, head and neck tumors, and other predictors of difficult intubation, with reduced laryngoscopy force and cervical spine motion compared to direct laryngoscopy (DL) [7]. These benefits have supported the broad adoption of VL across operating rooms, ICUs, and emergency settings.
Despite VL's advantages, DL remains an essential fallback technique. Airway guidelines from the American Society of Anesthesiologists and the Difficult Airway Society emphasize that clinicians must remain proficient in multiple techniques, including DL, to ensure readiness when visualization is obscured by blood, secretions, or device malfunction [8,9]. Straight blade laryngoscopy with the Miller blade retains clinical relevance in pediatric airways, patients with anterior laryngeal anatomy, and situations where camera visualization fails [10,11]. These scenarios underscore the ongoing importance of maintaining DL skills as a safety net.
As VL becomes increasingly dominant, hands-on exposure to DL may decline, particularly among trainees. Residents may graduate with limited DL experience, especially with straight blades like the Miller, potentially reducing confidence in fallback readiness. This concern is not unique to anesthesiology; procedural specialties such as surgery and endoscopy have documented "deskilling" effects when reliance on robotics or AI-assisted technology displaces foundational manual practice [12-14]. A similar dynamic may exist in airway management. While the Miller blade remains essential in scenarios such as pediatric intubation or when secretions obscure the VL view, it may now be encountered only rarely in training, not due to disinterest, but due to decreased opportunity.
Importantly, this study does not seek to demonstrate actual skill decay, nor to assert that video laryngoscopy should be curtailed. Rather, it aims to explore clinician perceptions of confidence, usage, and teaching of foundational techniques in a VL-driven landscape. Perceived gaps in training are educationally relevant, even when they reflect reduced exposure rather than actual incompetence. By quantifying these perceptions, we can begin to understand how reliance on advanced tools may quietly displace deliberate practice-and how that shift is being felt by clinicians at different stages of training.
This exploratory pilot survey study examined anesthesiology residents' and attendings' perceptions of Miller blade DL training in a VL-dominant era. Specifically, we assessed confidence, frequency of use, perceived importance, and beliefs about how teaching has changed. While this single-site study is not intended to draw generalizable conclusions, it offers early data to inform future research and training strategies aimed at preserving critical fallback skills when technology fails or is unavailable.
Materials and methods
This cross-sectional survey was administered via REDCap to anesthesiology residents and attending anesthesiologists at a single academic medical center. Residents were asked to report their confidence in using the Miller blade for DL, frequency of use, perceived importance of maintaining this skill, and beliefs regarding whether foundational manual airway techniques are being adequately taught. Attendings were asked about the frequency with which they teach DL, their perceived importance of preserving it, and their agreement with the statement that DL is becoming a "lost art".
Survey items were developed de novo by the study team, as no validated instrument addressed this specific topic. Questions were based on expert consensus and clinical experience, and no formal pilot testing or psychometric validation was performed prior to distribution. The full survey instrument is provided in Appendix A.
While the survey focused specifically on the Miller blade, we acknowledge that the Macintosh blade remains more commonly used in routine clinical DL. The Miller blade was selected for its pedagogical significance in teaching fallback techniques.
Survey responses used ordinal scales (e.g., 1-4 for confidence, 1-5 for importance), and results were summarized using medians and interquartile ranges. Because the data were ordinal and not normally distributed, Spearman's rank correlation coefficients were calculated to assess associations between confidence, frequency of use, perceived importance, and beliefs about declining teaching among residents. Confidence scores were not assessed among attendings; therefore, no direct statistical comparisons were made between cohorts.
This study was approved by the Rutgers Institutional Review Board (IRB# Pro2025001199).
Results
A total of 23 clinicians completed the survey, including 12 anesthesiology residents and 11 attending anesthesiologists. The overall response rate was 46%, with 33% of residents (12 of 36) and 65% of attendings (11 of 17) participating.
Among residents, the mean confidence score for performing Miller blade DL was 2.5 (on a 1-4 scale), and the mean frequency of use score was 2.2 (on a 1-5 scale). Residents rated the importance of maintaining Miller blade skills as relatively high (mean 3.75), and reported a high level of agreement with the belief that teaching of these skills is declining (mean 4.08).
Spearman correlation analyses among residents revealed a strong positive association between confidence and frequency of use (ρ=0.77, p=0.0031), and a moderate positive association between confidence and perceived importance (ρ=0.65, p=0.02). The correlation between confidence and the belief that DL teaching is declining was weak and not statistically significant (ρ=0.32, p>0.1). These relationships are illustrated in Figure 1.
Residents' confidence versus frequency of Miller blade useScatterplot with trend line showing the correlation between anesthesiology residents' self-reported confidence in using the Miller blade for direct laryngoscopy and their reported frequency of use. Each point represents one resident respondent. A positive association was observed (Spearman's ρ=0.77, p=0.0031).
Attendings reported a mean score of 1.8 for frequency of teaching DL techniques, a mean importance score of 3.8 for preserving these skills, and a mean agreement score of 3.36 with the statement that DL is becoming a "lost art". Confidence scores were not collected for attendings, and no direct statistical comparisons were made between resident and attending groups due to differences in survey structure.
Discussion
In this exploratory pilot survey, anesthesiology residents reported low confidence and infrequent use of the Miller blade for DL, yet consistently rated the skill as important. Confidence was strongly correlated with frequency of use, underscoring the role of regular exposure in perceived competence. Attendings likewise endorsed the importance of preserving DL but reported only occasional teaching of this technique. Together, these findings suggest a potential gap between the acknowledged value of DL and the opportunities provided to practice and teach it.
The growing dominance of VL in airway management is supported by randomized trials demonstrating improved first-pass success and glottic visualization [1-7]. However, guidelines continue to emphasize that fallback strategies-including DL-must remain part of clinician training and preparedness [8,9]. Our findings support this concern from an educational standpoint: residents perceive DL as important but report limited practice opportunities and teaching exposure. These perceived gaps are educationally meaningful, even if not indicative of skill decay per se.
Comparable patterns have been observed in other procedural specialties. In surgical education, increasing reliance on robotic platforms has prompted discussion about declining competence in open surgical techniques [12,13]. In gastrointestinal endoscopy, Sinagra et al. described how reliance on artificial intelligence may reduce trainee autonomy and tactile judgment, raising concerns about procedural deskilling [14]. These parallels suggest that technology-driven displacement of manual practice is a broader educational issue, with implications for airway training in anesthesiology.
While we do not claim that DL skills are being lost outright, our findings suggest that reduced exposure and hands-on practice may be contributing to declining confidence. This is not a failure of residents or faculty, but rather a training environment that increasingly favors newer tools. Deliberate reinforcement of fallback techniques, such as DL with the Miller blade, may help maintain readiness when VL fails or is unavailable. Structured simulation, supervised repetition, and case-based review could help preserve these skills, as has been recommended in surgical and endoscopy training [12-14].
This study has several limitations. It was conducted at a single academic center with a modest sample size, limiting generalizability. The survey instrument was developed de novo and has not been formally validated. Confidence was self-reported and may not reflect actual clinical performance. Additionally, the study focused on the Miller blade specifically, which may not represent all forms of direct laryngoscopy. No comparisons were made between residents and attendings due to differences in survey design.
Despite these limitations, this pilot offers structured data on how clinicians perceive foundational skill preservation in a VL-dominant training environment. Future research should expand to multi-center designs, use validated instruments, and incorporate objective performance metrics to better understand how modern airway training impacts fallback technique readiness.
Conclusions
VL has significantly advanced airway management and improved first-pass success, but it does not eliminate the need for DL. In this exploratory pilot survey, anesthesiology residents and attendings acknowledged the enduring importance of Miller blade skills while reporting limited confidence, infrequent use, and reduced teaching exposure. These findings suggest a potential training gap in preserving fallback techniques within a VL-dominant environment.
The study's single-center design, modest response rate, and use of a non-validated survey instrument limit generalizability. Nevertheless, the consistency of responses across both trainees and faculty highlights a perceived shift in training priorities that warrants further investigation. Multi-center studies using validated tools and objective skill assessments are needed to determine whether reliance on VL is contributing to reduced exposure and proficiency in foundational direct laryngoscopy techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Video laryngoscopy vs direct laryngoscopy for endotracheal intubation in the operating room: a cluster randomized clinical trial JAMA Ruetzler K Bustamante S Schmidt MT 1279128633120243849799210.1001/jama.2024.0762 PMC 10949146 · doi ↗ · pubmed ↗
- 2Expected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients Br J Anaesth Jungbauer A Schumann M Brunkhorst V 54655010220091923388110.1093/bja/aep 013 · doi ↗ · pubmed ↗
- 3A randomized controlled trial comparing C Mac D Blade and Macintosh laryngoscope for nasotracheal intubation in patients undergoing surgeries for head and neck cancer Saudi J Anaesth Hazarika H Saxena A Meshram P Kumar Bhargava A 35411220182941645410.4103/sja.SJA_239_17PMC 5789504 · doi ↗ · pubmed ↗
- 4Randomized controlled trial of the Pentax AWS, Glidescope, and Macintosh laryngoscopes in predicted difficult intubation Br J Anaesth Malik MA Subramaniam R Maharaj CH Harte BH Laffey JG 76176810320091978353910.1093/bja/aep 266 · doi ↗ · pubmed ↗
- 5Management of the predicted difficult airway: a comparison of conventional blade laryngoscopy with video-assisted blade laryngoscopy and the Glide Scope Eur J Anaesthesiol Serocki G Bein B Scholz J Dörges V 24302720101980932810.1097/EJA.0b 013e 32832 d 328d · doi ↗ · pubmed ↗
- 6A randomized controlled comparison of non-channeled king vision, Mc Grath MAC video laryngoscope and Macintosh direct laryngoscope for nasotracheal intubation in patients with predicted difficult intubations BMC Anesthesiol Zhu H Liu J Suo L Zhou C Sun Y Jiang H 1661920193147081410.1186/s 12871-019-0838-z PMC 6717380 · doi ↗ · pubmed ↗
- 7Measurement of forces applied using a Macintosh direct laryngoscope compared with a Glidescope video laryngoscope in patients with predictors of difficult laryngoscopy: a randomised controlled trial Eur J Anaesthesiol Cordovani D Russell T Wee W Suen A Cooper RM 2212263620193030852410.1097/EJA.0000000000000901 · doi ↗ · pubmed ↗
- 82022 American Society of Anesthesiologists practice guidelines for management of the difficult airway Anesthesiology Apfelbaum JL Hagberg CA Connis RT 318113620223476272910.1097/ALN.0000000000004002 · doi ↗ · pubmed ↗