Persistent risk of hepatocellular carcinoma despite improvement of liver stiffness in patients with chronic HBV with advanced fibrosis
Lesley A. Patmore, Lilian Y. Liang, George Papatheodoridis, Mai Kilany, Arno Furquim d’Almeida, Vincent W.S. Wong, Margarita Papatheodoridi, Thomas Vanwolleghem, Pieter Honkoop, Hans Blokzijl, Özgür M. Koc, Harry L.A. Janssen, Matthijs Kramer, Joep de Bruijne, Apichat Kaewdech

TL;DR
Patients with chronic hepatitis B and advanced liver damage still face a high risk of liver cancer even if their liver stiffness improves during treatment.
Contribution
This study clarifies that improved liver stiffness during treatment does not reduce the risk of hepatocellular carcinoma in patients with chronic HBV and advanced fibrosis.
Findings
On-treatment liver stiffness improvement was not associated with reduced hepatocellular carcinoma (HCC) risk.
Patients with decreased liver stiffness had a lower risk of hepatic decompensation.
HCC surveillance should continue regardless of liver stiffness improvement during treatment.
Abstract
Patients with chronic HBV (CHB) with advanced fibrosis are at high risk for hepatocellular carcinoma (HCC). Liver stiffness measurement (LSM) correlates with fibrosis in untreated patients, and is used to monitor changes in severity of liver disease. However, the association between on-treatment LSM and HCC risk is controversial. We conducted an international multicenter retrospective cohort study of patients with CHB with advanced fibrosis and assessed the association between on-treatment LSM, HCC development, and decompensation events. We analyzed 562 patients (62.8% F4 LSM measurement, 69.2% Asian). During antiviral therapy, the on-treatment LSM decreased to <6 kPa in 209 (37.2%), to 6–9 kPa in 174 (31.0%), and remained >9 kPa in 179 (31.9%) patients. During a median follow-up of 6.8 years after the on-treatment LSM, 56 patients developed HCC and 18 (32.2%) had an on-treatment LSM…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
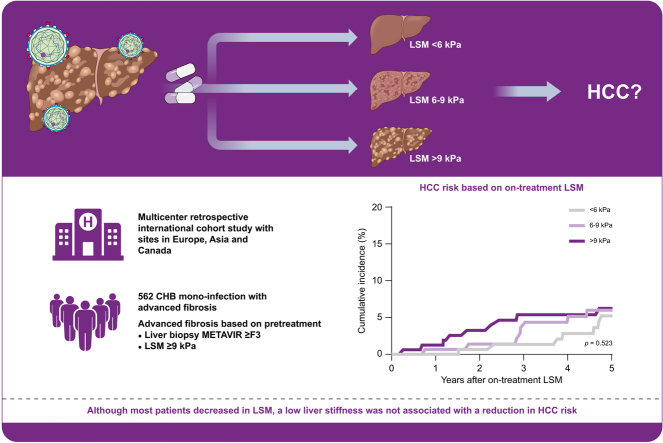 Figure 1
Figure 1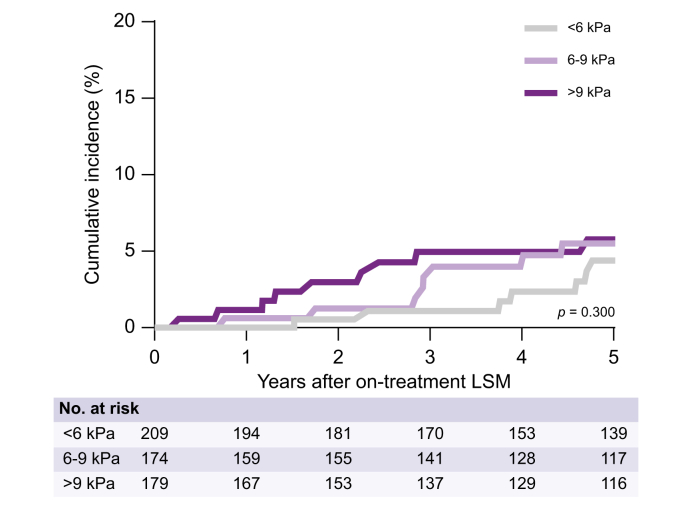 Figure 2
Figure 2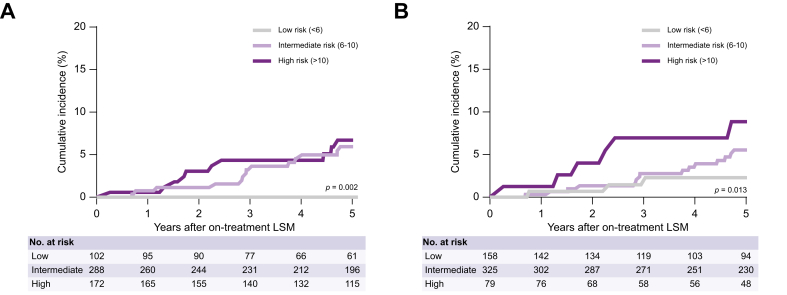 Figure 3
Figure 3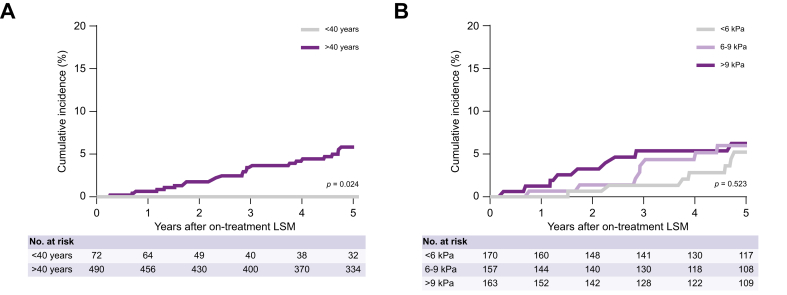 Figure 4
Figure 4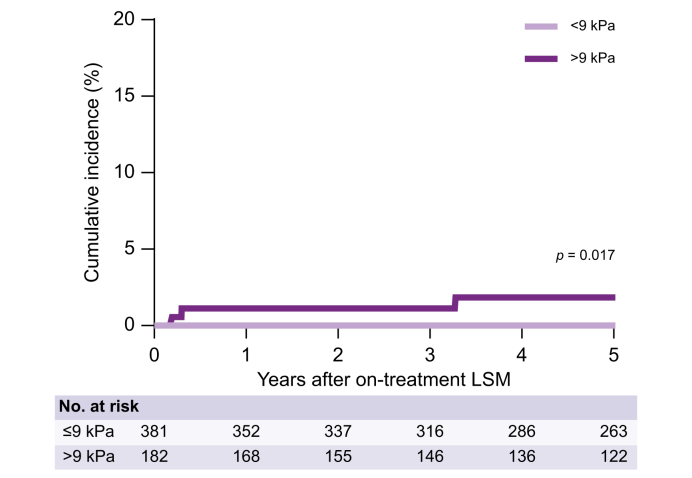 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis B Virus Studies · Liver Disease Diagnosis and Treatment · Hepatitis C virus research
Introduction
Patients with chronic HBV (CHB) with advanced fibrosis are at high risk for hepatocellular carcinoma (HCC). Studies have shown that suppression of viral replication with nucleo(s)tide analogs (NUCs) can reduce the risk of HCC, potentially through decreasing hepatic inflammation and liver fibrosis.1^,^2 Therefore, monitoring changes in fibrosis grade is important in the management of patients with CHB.
Liver biopsy is considered the gold standard for the grading of fibrosis stage, but it is invasive, expensive, and associated with risks such as severe bleeding and even mortality. Therefore, liver stiffness measurement (LSM) using vibration-controlled transient elastography (VCTE) has largely replaced liver biopsy as the preferred method for assessing liver fibrosis in patients with currently untreated CHB, because LSM correlates well with liver histology in this population.[3], [4], [5] In addition, there appears to be a direct correlation between higher LSM values and HCC risk in patients with currently untreated CHB.6^,^7
Interestingly, various studies have reported an improvement in LSM after initiation of antiviral therapy in patients with CHB with advanced fibrosis, but whether this decrease in LSM reflects a reduction in severity of inflammation, fibrosis, or both, is unknown.[8], [9], [10] Furthermore, several studies have incorporated LSM obtained during treatment to predict subsequent HCC risk; however, it remains unclear to what extent a decrease in LSM in CHB with advanced fibrosis is associated with a clinically significant reduction in the risk of HCC.[11], [12], [13] Nevertheless, LSM is widely applied to monitoring changes in liver disease severity in patients with chronic liver disease, and recently updated FDA guidance for the design of trials in HBV and HDV suggest the use of non-invasive assessment of liver fibrosis, such as LSM, as surrogate endpoints in trials of novel agents.14
Therefore, the aim of this study was to study changes in LSM over time in patients with CHB with advanced fibrosis initiating antiviral therapy, and to study the association between on-treatment LSM with subsequent risk of HCC and hepatic decompensation.
Patients and methods
Study design
We conducted an international multicenter retrospective cohort study of all consecutive HBV mono-infected patients with advanced fibrosis who underwent LSM at least 3 years after initiation of NUC therapy. Advanced fibrosis (METAVIR ≥F3) was diagnosed based on compatible histological findings, a pretreatment LSM ≥9.0 kPa, and/or other findings consistent with cirrhosis (e.g. nodular liver on imaging with signs of portal hypertension on imaging or endoscopy).
We excluded patients with a history of hepatic decompensation, presence or past viral co-infections (HDV, HCV, or HIV) or presence or development of other known chronic liver diseases (documented alcohol-related liver disease/alcohol misuse, Wilson’s disease, primary biliary cholangitis, primary sclerosing cholangitis, autoimmune hepatitis, and hemochromatosis). Patients who did not start antiviral therapy with a NUC or who developed HCC or hepatic decompensation before the on-treatment LSM were also excluded.
Data collection and endpoint definitions
Data were collected from academic and non-academic sites in Belgium, Canada, Greece, Hong Kong, the Netherlands, and Thailand. Baseline was set as the date of the first off-therapy fibrosis assessment that met the inclusion criteria. An LSM >12 kPa was considered as cirrhosis. Data at on-treatment LSM were obtained at the time of the first on-treatment LSM performed after at least 3 years of follow-up. LSM was obtained by VCTE (Fibroscan, Echosens, Paris, France; equipped with both M and XL probes) by trained healthcare providers. Only examinations with at least 10 valid individual measurements and acceptable variances, defined as IQR <30%, were deemed valid. On-treatment LSM values were categorized according to cut-offs validated against METAVIR stage in untreated patients; <6 kPa (F0-1), 6–9 kPa (F2) and >9 kPa (F3–4).15
Diagnosis of HCC was based on compatible imaging findings or histology, as per clinical guidelines. Decompensation was defined as the first of a composite of variceal bleeding, clinically relevant ascites that required the use of diuretics, or large volume paracentesis or overt hepatic encephalopathy that required treatment.
Statistical analysis
The primary aim of the study was assessment of the cumulative incidence of HCC across on-treatment LSM strata and according to LSM-based risk scores. The key secondary aim was to study the cumulative incidence of hepatic decompensation across on-treatment LSM strata and according to BAVENO VII criteria for ruling out clinically significant portal hypertension (i.e. LSM <15 kPa with platelet count >150×10^6^/L).16 Continuous variables were described using median and IQR or mean values and SD. Categorical variables were described as frequencies or percentages. The CAGE-B (based on baseline presence of cirrhosis, age, and follow-up LSM) and the SAGE-B (based on age and LSM at follow-up) scores were calculated as previously reported,11 and patients were classified as low (<6), intermediate (6–10) or high (>10) risk for HCC development based on previously reported cut-offs.11 The cumulative incidence of HCC and decompensation after the on-treatment LSM was assessed using the Kaplan-Meier method and compared between different groups using the log-rank test. Follow-up time was calculated as the interval between the date of the on-treatment (follow-up) LSM and the date of the event of interest (HCC or hepatic decompensation). Univariable Cox regression models were used to estimate the effect of various variables on the hazard of HCC and hepatic decompensation. Multivariable Cox regression was used to identify independent prognostic factors. Hazard ratios (HRs) and their 95% CIs along with corresponding p values are presented. A p value <0.05 was considered to be statistically significant. All data were analyzed using IBM SPSS Statistics Version 28.
Ethics
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and the principles of Good Clinical Practice. The study protocols were primarily reviewed by the Erasmus MC Medical Ethical Committee. The requirement for informed consent was waived, and the institutional review boards of participating sites gave necessary approval whenever required.
Results
Patient characteristics at baseline (pretreatment) fibrosis assessment
We screened 800 patients for eligibility; 122 patients were excluded because they had no off-treatment LSM or biopsy; 92 patients had <3 years of follow-up; and 24 developed HCC before the on-treatment LSM (Fig. S1). We included and analyzed 562 patients with a median age at baseline of 50 years (IQR 41–58), 75.6% were men. Most of the patients were Asian (69.2%) or Caucasian (21.7%). Median alanine aminotransferase (ALT) was 57 U/L (IQR 38–109), median platelet count was 179 × 10^9^/L (IQR 142–229) and median HBV DNA was 5.5 log_10_ IU/ml (IQR 3.9–6.6). At baseline, 209 (37.2%) of the patients had F3 and 353 (62.8%) had F4 based on histology (15.7%) or LSM (65.3%). Among patients with baseline LSM data (n = 367, 65.3%), the median baseline LSM was 12.5 kPa, (IQR 10.5–17.1). Information on the presence of metabolic comorbidities was available for a subset of patients; 95 patients (16.9%) had diabetes, 160 (28.5%) had hypertension, 58 (10.3%) had dyslipidemia, and 100 (17.8%) had steatosis. All patients initiated antiviral therapy with a NUC; most were treated with entecavir (ETV; 52%). All patient characteristics at baseline are described in Table 1.Table 1. Baseline characteristics.Table 1. At start of therapy (n = 562)Age, years50 (41–58)Male, n (%)425 (75.6)Ethnicity, n (%) Asian389 (69.2) Caucasian122 (21.7) Other51 (9.7)ALT, U/L57 (38–109)Platelet count, × 10^9^/L179 (142–229)HBeAg, n (%)191 (34)HBV DNA, log_10_ IU/ml5.5 (3.9–6.6)Fibrosis n (%)/(biopsy, n/LSM, n) F3209 (37.2)/(64/145) F4353 (62.8)/(81/222)Initial antiviral therapy, n (%) ETV292 (52.0) TDF/TAF123 (21.9) Other147 (26.2)Diabetes, n (%)95 (16.9)Hypertension, n (%)160 (28.5)Dyslipidemia, n (%)58 (10.3)Overweight, n (%)111 (19.8)Steatosis, n (%)100 (17.8)At on-treatment LSM (n = 562)Median time between baseline and on-treatment LSM, years4.7 (3.6–6.6)Age, years56 (47–63)ALT, U/L28 (21–41)Platelet count, ×10^9^/L173 (139–214)Undetectable HBV DNA, n (%)472 (84)LSM, n (%) <6 kPa209 (37.2) 6–9 kPa174 (31.0) >9 kPa179 (31.9)Antiviral therapy, n (%) ETV298 (53.0) TDF/TAF156 (27.8) Other108 (19.1)End of follow-upMedian follow-up time after on-treatment LSM, years6.4 (3.7–11.1)HCC, n (%)56 (10.4)Decompensation, n (%)16 (2.8)Data are presented as mean (SD) for normally distributed data, as median (IQR) for non-normally distributed data and as n(%) for categorical variables. ∗Some patients received multiple types of antiviral therapy. ALT, alanine aminotransferase; ETV, entecavir; HCC, hepatocellular carcinoma; LSM, liver stiffness measurement; TAF, tenofovir alafenamide fumarate; TDF, tenofovir disoproxil fumarate.
Patient characteristics at on-treatment LSM
All patients underwent an on-treatment LSM. The median time between baseline fibrosis assessment and on-treatment LSM was 4.7 years (IQR 3.6–6.6) and median on-treatment LSM was 7.1 kPa (IQR 5.1–10.3). On-treatment LSM was <6 kPa in 209 (37.2%) patients, 6–9 kPa in 174 (31.0%) patients, and >9 kPa in 179 (31.9%) patients. The median ALT at on-treatment LSM was 28 U/L (IQR 21–41) and 84% had undetectable HBV DNA at on-treatment LSM. All patient characteristics at on-treatment LSM are described in Table 1.
HCC development in the overall cohort and stratified by LSM
During a median follow-up of 6.4 years (IQR 3.7–11.1) after the on-treatment LSM, 56 patients developed HCC. The 5- and 10-year cumulative incidences of HCC were 5.2% and 14.1% (Fig. S2). There was no significant difference in HCC risk between Asian and non-Asian patients (4.9% vs. 5.4% at 5 years, p = 0.675).
In univariable analysis, older age (HR 1.065, 95% CI 1.038–1.093, p <0.001), lower platelet count (HR 0.990, 95% CI 0.985–0.996, p <0.001), diabetes mellitus (HR 2.393, 95% CI 1.347–4.251, p = 0.003), and hypertension (HR 3.352, 95% CI 1.910–5.884, p <0.001) were predictors for HCC development, whereas on-treatment LSM was not (HR 1.016, 95% CI 0.983–1.050, p = 0.357; Table 2).Table 2. Univariable and multivariable analysis of factors associated with incident HCC.Table 2. UnivariableMultivariableHR95% CIp valueaHR95% CIp valueAge, years1.0651.038–1.093<0.0011.0581.026–1.091<0.001Male sex0.9840.529–1.8310.9601.1550.598–2.2300.667Platelet count, ×10^9^/L0.9900.985–0.996<0.0010.9920.992–0.9980.005Baseline F41.3680.692–2.7030.3671.2440.676–2.2890.483Diabetes2.3931.347–4.2510.0031.2090.646–2.2600.553Hypertension3.3521.910–5.884<0.0011.8160.971–3.3950.062On-treatment LSM, kPa1.0160.983–1.0500.3570.9740.932–1.0180.974Results were obtained with Cox proportional hazard analysis and given as (a)HR with 95% CI and p value. aHR, adjusted hazard ratio; HCC, hepatocellular carcinoma; HR, hazard ratio; LSM, liver stiffness measurement.
Of the 56 patients who developed HCC after the on-treatment LSM, 18 (32.2%) had an on-treatment LSM <6 kPa, 19 (33.9%) had an on-treatment LSM 6–9 kPa, and 19 (33.9%) had an on-treatment LSM >9 kPa. The 5-year cumulative HCC incidence was comparable across on-treatment LSM strata; 4.4% for <6 kPa, 5.5% for 6–9 kPa, and 5.8% for >9 kPa (p = 0.300, Fig. 1). Findings were consistent among the subset of patients enrolled in this study based on either advanced fibrosis diagnosed on liver biopsy (n = 145, p = 0.371) or non-invasive assessment (n = 417, p = 0.146).Fig. 1. Cumulative HCC incidence after on-treatment LSM stratified by on-treatment LSM category. Data were analyzed using the Kaplan-Meier method and the log-rank test was used to compare the groups; p ≤0.05 indicates a statistically significant difference. HCC, hepatocellular carcinoma; LSM, liver stiffness measurement.Fig. 1
In a multivariable analysis adjusting for sex, baseline fibrosis status, diabetes mellitus, and hypertension, only older age (adjusted HR [aHR] 1.058, 95% CI 1.026–1.091, p <0.001) and lower platelet count (aHR 0.992, 95% CI 0.992–0.998, p = 0.005) were significantly associated with HCC development, whereas on-treatment LSM was not (aHR 0.974, 95% CI 0.932–1.018, p = 0.974) (Table 2).
Performance of the CAGE-B and SAGE-B score for the prediction of HCC
The median CAGE-B score was 9 (IQR 6–11), and 102 (18.1%), 288 (51.2%), and 172 (30.6%) patients were classified as low, intermediate, and high risk, respectively, based on their CAGE-B score. The 5-year cumulative incidence of HCC in the low-risk CAGE-B group was 0%, compared with 5.9% in the intermediate-risk group and 6.7% in the high-risk group (p = 0.002 by log-rank test; Fig. 2A).Fig. 2. Cumulative HCC incidence after on-treatment LSM stratified by (A) CAGE-B strata and (B) SAGE-B strata. Data were analyzed using the Kaplan-Meier method and the log-rank test was used to compare the groups; p ≤0.05 indicates a statistically significant difference. HCC, hepatocellular carcinoma; LSM, liver stiffness measurement.Fig. 2
The median SAGE-B risk was 6 (IQR 4–9), and 158 (28.1%), 325 (57.8%), and 79 (14.1%) patients were classified as low, intermediate, and high risk, respectively, based on their SAGE-B score. The 5-year cumulative incidence of HCC in the low-risk SAGE-B group was 2.3%, compared with 5.5% in the intermediate-risk group and 8.9% in the high-risk group (p = 0.013 by log-rank test; Fig. 2B).
Importantly, the association between CAGE-B/SAGE-B scores and HCC appeared to be predominantly driven by age. We observed no HCC in the subset of patients aged <40 years at follow-up LSM, compared with a 5-year cumulative HCC incidence of 5.8% for patients aged >40 years (p = 0.024; Fig. 3A). Therefore, we performed a sensitivity analysis in a subset of patients older than 40 years at on-treatment LSM. Among these 490 patients, 170 (34.7%) patients had an on-treatment LSM <6 kPa, 157 (33.4%) patients had 6–9 kPa, and 163 (33.3%) patients had >9 kPa. The 5-year cumulative HCC incidence was comparable across on-treatment LSM strata; 5.2% for <6 kPa, 6.0% for 6–9 kPa, and 6.2% for >9 kPa (p = 0.523, Fig. 3B).Fig. 3. Cumulative HCC incidence after on-treatment LSM stratified by (A) age and (B) on-treatment LSM strata in the subset of patients >40 years. Data were analyzed using the Kaplan-Meier method and the log-rank test was used to compare the groups; p ≤0.05 indicates a statistically significant difference. HCC, hepatocellular carcinoma; LSM, liver stiffness measurement.Fig. 3
Decompensation events in the overall cohort and stratified by LSM
After the on-treatment LSM, 16 patients experienced hepatic decompensation (seven developed hepatic decompensation, six developed variceal bleed, and three developed hepatic encephalopathy). In 10 of the 16 patients, the decompensation event was preceded by the development of HCC.
The 5-year cumulative incidence of decompensation was 0.6%. In univariable analysis, older age (HR 1.074, 95% CI 1.021–1.130, p = 0.006) and on-treatment LSM (HR 1.047, 95% CI 1.004–1.091, p = 0.034) were predictors for decompensation. Given the low number of events, no multivariable analysis was performed.
We found no decompensation events in patients with an on-treatment LSM <9 kPa and, therefore, we combined patients from the <6 kPa group with the 6–9 kPa group. The cumulative incidence of hepatic decompensation for patients with <9 kPa at the on-treatment LSM (n = 381) was 0%, compared with the 1.8% for patients with an on-treatment LSM >9 kPa (p = 0.017; Fig. 4). Findings were consistent after excluding patients with a decompensation event after HCC development (p = 0.002). In 317 (56.4%) patients, clinically significant portal hypertension could be ruled out based on BAVENO VII criteria. No cases of hepatic decompensation were observed in this group (p = 0.008; Fig. S3).Fig. 4. Cumulative incidence of hepatic decompensation after on-treatment LSM stratified by LSM ≤9 kPa and LSM >9 kPa. Data were analyzed using the Kaplan-Meier method and the log-rank test was used to compare the groups; p ≤0.05 indicates a statistically significant difference. LSM, liver stiffness measurement.Fig. 4
Discussion
In this study of 562 patients with previously untreated CHB with advanced fibrosis enrolled from 11 centers in Asia, Europe, and North America, we observed that most patients experienced a marked improvement in LSM after initiation of antiviral therapy. Although a reduction in LMS to ≤9 kPa was associated with a reduced risk of hepatic decompensation, we observed a persistent risk of HCC in this population. These findings suggest that on-treatment LSM values should not be used to guide HCC surveillance strategies.
The current study provides important insights into the risk of liver-related events in patients with CHB with advanced fibrosis who are treated with NUCs. First of all, the risk of de novo decompensation events appears to be very low; the 5-year cumulative incidence after the follow-up LSM assessment was 0.6%. Unfortunately, our study also highlights the persistent risk of HCC development in this population; the 5- and 10-year cumulative HCC incidences were 5.2% and 14.1%. These observations are in line with previous reports and underscore that HBV DNA suppression alone is insufficient to eliminate HCC risk.17 Based on these findings, exploration of alternative strategies to increase rates of functional cure is paramount if the risk of HCC is to be mitigated. Pending availability of such options, our findings support current recommendations to continue HCC surveillance in this patient group despite viral suppression.
The high persistent risk of HCC remains disappointing in the light of previous data suggesting that reversal of cirrhosis is possible in most patients with cirrhosis treated with ETV or tenovofir disoproxil fumarate (TDF).1 Based on these observations, we hypothesized that a reduction in fibrosis stage, assessed using LSM, would also reflect a reduction in HCC risk. In the current cohort, 77.4% had an on-treatment LSM suggestive of fibrosis improvement, a number that is remarkably similar to the proportion reported by Marcellin et al. using histology as a reference.1 Nevertheless, LSM can be influenced by a myriad of factors beyond liver fibrosis, such as inflammation, cholestasis, and cardiac congestion.18
There are multiple potential explanations for our findings. First, it is unclear whether an on-treatment reduction in LSM reflects a decrease in inflammatory activity, a decrease in liver fibrosis severity, or both. As such, a significant proportion of patients with an improvement in LSM might not have achieved fibrosis regression, which could account for the failure to achieve a significant reduction in HCC risk. Another potential explanation pertains to the fact that many oncogenic processes associated with HBV infection, including HBV DNA integration, have already occurred before therapy initiation and might not be reversible even with long-term treatment. In this scenario, reductions in fibrosis stage, even if confirmed with liver biopsy, might not be sufficient to completely eliminate the risk of HCC.
Our results do not appear to confirm the findings from a recent follow-up analysis of the PAGE-B cohort, in which Papatheodoridis et al. compared the cumulative incidence of HCC beyond 5 years of therapy with ETV or TDF in White patients with CHB according to fibrosis status at baseline and the LSM at year 5.11 In this study, higher follow-up LSM values were linked to a statistically higher HCC risk during subsequent follow-up. However, careful assessment showed that, although HCC might have occurred somewhat earlier in patients with higher LSM, HCC was observed in 4.9% of patients with cirrhosis at baseline who had a decrease in LSM to <12 kPa.11 Therefore, these findings are consistent with the current report. Recently, Semmler et al. investigated dynamic changes in LSM in patients with advanced chronic liver disease. They reported that a reduction of at least 20% in LSM was associated with a lower risk of hepatic decompensation. However, their study population included patients with various underlying liver disease etiologies, only a small proportion of whom had CHB, as well as shorter intervals between LSM assessments and different clinical endpoints. These differences limit direct comparability with our cohort. In our study, 305 patients experienced a ≥20% decrease in LSM, but showed a similar 5-year incidence of HCC compared with those without such a decrease (4.5% vs. 4.9%, p = 0.997; Fig. S4).
We also attempted to validate two proposed risk scores, CAGE-B and SAGE-B, for prediction of HCC risk after the follow-up LSM. Both risk scores include age and LSM after 5 years of treatment. In our cohort, HCC risk was higher in patients with higher CAGE-B and SAGE-B scores, but this appeared to be driven by age, not by LSM. In our cohort, all HCCs developed in patients over 40 years of age at the time of follow-up LSM. Therefore, we performed a sensitivity analysis in patients >40 years at on-treatment LSM and found comparable cumulative incidences across different on-treatment LSM strata. These discrepant findings might be explained by differences in patient and viral characteristics, given that the PAGE-B cohort comprised a White population and the current cohort was predominantly Asian patients.
Our findings could have important clinical implications. Given the persistent HCC risk, continued HCC surveillance is recommended despite successful HBV DNA suppression among patients with CHB with advanced fibrosis. As the HBV population ages, the number of patients eligible for HCC surveillance will increase rapidly.19 Although baseline risk scores, such as PAGE-B, might be valuable in stratifying HCC risk, the validity in patients with advanced fibrosis is uncertain, and clinical application is hampered by the fact that only a few patients with cirrhosis have low PAGE-B scores.[20], [21], [22] As such, alternative methods are urgently needed. The current study suggests that a reduction in LSM to values associated with the absence of fibrosis in untreated patients is not associated with elimination of HCC risk and, therefore, that surveillance should be continued in patients with advanced fibrosis at baseline regardless of LSM values obtained during therapy. Furthermore, our findings also indicate that on-treatment LSM could have value in predicting subsequent decompensation events in this population.
Although this is a unique cohort comprising a mixed-ethnicity population obtained from expert centers across the globe, our study has limitations. First, this is an international retrospective cohort study in which not all potential risk factors for the development of HCC, use of moderate alcohol consumption (patients with alcohol misuse were excluded), smoking, and other lifestyle factors could be taken into account. In addition, the decisions to start treatment and when to perform LSM varied by site and country. However, sensitivity analyses revealed no influence of center on the study findings. Second, some patients used older antiviral agents, such as lamivudine or adefovir, potentially increasing the risk of HCC development. However, most started treatment with ETV or tenofovir, and most of those who did not initially use these antivirals transitioned to them before the on-treatment LSM or during follow-up. We found similar results in a sensitivity analysis excluding patients on antiviral therapy other than ETV or tenofovir. Furthermore, detectable HBV DNA at on-treatment LSM was not associated with an increased risk of HCC and excluding patients with detectable HBV DNA at follow-up LSM also did not influence any of the findings. Third, liver stiffness thresholds remain controversial and variable across studies. LSM values of >8–9 kPa are typically associated with the presence of significant or advanced fibrosis.4^,^23 For the current study, we used a cut-off of 9 kPa to enrich our study population for patients with more severe liver disease. Unfortunately, we were unable to determine whether LSM in our cohort correlated accurately with histological stages F3 or F4, because no paired liver biopsies were performed for validation. Furthermore, with the current dataset, we were unable to additionally calculate other fibrosis scores, such as the enhanced liver fibrosis score. However, existing literature has consistently demonstrated that, in treatment-naïve patients, LSM values corresponding to F3 and F4 stages generally show good concordance with histological fibrosis grading.3 Moreover, there is currently no established evidence to determine the optimal timing for on-treatment fibrosis assessment after initiation of antiviral therapy. Therefore, we selected a pragmatic cut-off of a minimum of 3 years between the first and second assessments. To further ensure the robustness of our findings, we conducted a subanalysis including only patients with at least a 5-year interval between fibrosis measurements and found consistent results: the 5-year HCC risk was 4.0% for patients with LSM <6 kPa, 3.8% for those with LSM 6–9 kPa, and 5.2% for those with LSM >9 kPa (p = 0.800). However, long-term follow-up after the on-treatment LSM, preferably with multiple LSMs, is needed to confirm our findings. In addition, most of the sites were academic centers, which could influence the external validity of our findings. In our cohort, 90.7% of patients were eligible for HCC surveillance based on the presence of cirrhosis, PAGE-B ≥10, or other criteria. Findings were consistent when limiting our analyses to patients eligible for HCC surveillance based on these criteria (Fig. S5A and B). Finally, although we observed a lower risk of decompensation events in patients with a follow-up LSM ≤9 kPa, the number of events was small and, therefore, this finding requires further confirmation.
In conclusion, most patients with CHB with advanced fibrosis experienced a decrease in LSM during antiviral therapy. Unfortunately, although this improvement in LSM was associated with a reduced risk of subsequent decompensation events, it was not associated with a clinically relevant reduction in the risk of HCC. Therefore, baseline fibrosis stage and not on-treatment LSM should be used to guide HCC surveillance strategies.
Abbreviations
aHR, adjusted hazard ratio; ALT, alanine aminotransferase; CI, confidence interval; CHB, chronic HBV; ETV, entecavir; HCC, hepatocellular carcinoma; HR, hazard ratio; IQR, interquartile range; LSM, liver stiffness measurement; NUC, nucleo(s)tide analog; TAF, tenofovir alafenamide fumarate; TDF, tenofovir disoproxil fumarate; VCTE, vibration-controlled transient elastography.
Financial support
The study was sponsored by the 10.13039/501100015383Foundation for Liver and Gastrointestinal Research (10.13039/501100015383SLO), Rotterdam, The Netherlands. The SLO had no influence on study design, data acquisition or analysis, or the decision to submit for publication.
Authors’ contributions
Collection of data: LAP, LYL, MK, AK. Study design, writing of manuscript and approval of final version: LAP, MJS. Critical review of the manuscript and approval of final version: LYL, GP, MKilany, AFA, VW, MP, TV, PH, HB, OMK, HLAJ, MKramer, JdB, AK, RAdM, RBT, GLW, JJF.
Data availability
The data that support these findings are not publicly available, because they are subject to (inter)national data protection laws to ensure data privacy of the study participants. Therefore, the data cannot be shared.
Conflicts of interest
LAP: research grant from Gilead Sciences. GP: advisor/lecturer for 10.13039/100006483AbbVie, Albireo, 10.13039/100002429Amgen, Dicerna, and Genesis; research grant from Gilead Sciences; member of data safety monitoring board or advisory board for Gilead Sciences, Novo Nordisk, Janssen, 10.13039/501100014382Ipsen, 10.13039/100020955GSK, and 10.13039/100004337Roche. VW: consultant or advisory board member for 10.13039/100006483AbbVie, Boehringer Ingelheim, 10.13039/100024223Echosens, Gilead Sciences, 10.13039/100018262Intercept, 10.13039/100016915Inventiva, 10.13039/501100004191Novo Nordisk, 10.13039/100004319Pfizer, Sagimet Biosciences, 10.13039/100031397TARGET PharmaSolutions, and Visirna; speaker for Abbott, 10.13039/100006483AbbVie, 10.13039/100024223Echosens, Gilead Sciences, 10.13039/501100004191Novo Nordisk, and Unilab; research grant from Gilead Sciences; co-founded Illuminatio Medical Technology. TV: senior clinical investigator fellowship from the Research Foundation Flanders (FWO) (18B2821N). His institution has received grants from 10.13039/100020955GSK, Gilead Sciences, 10.13039/100008021Bristol Myers Squibb, and Fujirebio. TVW: consultant for 10.13039/100030732MSD, 10.13039/100008897Janssen Pharmaceuticals, Gilead Sciences, 10.13039/100006483AbbVie, Bristol Myers Squibb; sponsored lectures for Gilead Sciences, and AbbVie; received support for attending conferences/travel from 10.13039/501100014382Ipsen, Gilead and 10.13039/100006483AbbVie. HLAJ: research grants from Gilead Sciences, GSK, Janssen, 10.13039/100004337Roche, Vir Biotechnology; consultant for Aligos, Gilead Sciences, 10.13039/100020955GSK, 10.13039/501100016387Grifols, 10.13039/100004337Roche, 10.13039/100019650Vir Biotechnology Inc, and Precision Biosciences. JdB: research support from 10.13039/501100008645Terumo. AK: research grants or support from 10.13039/100004337Roche, 10.13039/100016545Roche Diagnostics, and 10.13039/100001316Abbott Laboratories, and honoraria from 10.13039/100004337Roche, 10.13039/100016545Roche Diagnostics, 10.13039/100001316Abbott Laboratories, and Esai. RAdM: research support from 10.13039/100004337Roche. RBT: research support from 10.13039/501100023453Norgine, speaker fees from WL Gore and Falk; consultant for Gilead, Boehringer Ingelheim, Astra Zenica, and 89Bio. GLHW: research grants from Gilead Sciences; consultant for 10.13039/100004325AstraZeneca, Gilead Sciences, 10.13039/100020955GSK, and Janssen; speaker fees from Abbott, 10.13039/100006483AbbVie, Ascletis, 10.13039/100008021Bristol Myers Squibb, 10.13039/100024223Echosens, Gilead Sciences, Janssen, and Roche; JJF: personal fees for consulting from 10.13039/100006483AbbVie, Enanta, Gilead, Janssen, and 10.13039/100004337Roche, and research funding from AbbVie, Abbott, Gilead, and 10.13039/501100013899FUJIFILM Wako Chemicals. MJS: research support and consultancy from 10.13039/100004337Roche, Gilead, Albireo/10.13039/501100014382Ipsen, Fujirebio. None of the remaining authors have any interests to declare.
Please refer to the accompanying ICMJE disclosure forms for further details.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marcellin P.Gane E.Buti M.Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study Lancet 38120134684752323472510.1016/S 0140-6736(12)61425-1 · doi ↗ · pubmed ↗
- 2Papatheodoridis G.V.Lampertico P.Manolakopoulos S.Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos(t)ide therapy: a systematic review J Hepatol 5320103483562048349810.1016/j.jhep.2010.02.035 · doi ↗ · pubmed ↗
- 3Marcellin P.Ziol M.Bedossa P.Non-invasive assessment of liver fibrosis by stiffness measurement in patients with chronic hepatitis B Liver Int 2920092422471863706410.1111/j.1478-3231.2008.01802.x · doi ↗ · pubmed ↗
- 4Li Y.Huang Y.S.Wang Z.Z.Systematic review with meta-analysis: the diagnostic accuracy of transient elastography for the staging of liver fibrosis in patients with chronic hepatitis B Aliment Pharmacol Ther 4320164584692666963210.1111/apt.13488 · doi ↗ · pubmed ↗
- 5Seo Y.S.Kim M.Y.Kim S.U.Accuracy of transient elastography in assessing liver fibrosis in chronic viral hepatitis: a multicentre, retrospective study Liver Int 352015224622552568271910.1111/liv.12808 · doi ↗ · pubmed ↗
- 6Fung J.Lai C.L.Seto W.K.Prognostic significance of liver stiffness for hepatocellular carcinoma and mortality in H Be Ag-negative chronic hepatitis BJ Viral Hepat 1820117387442065930610.1111/j.1365-2893.2010.01355.x · doi ↗ · pubmed ↗
- 7Chon Y.E.Jung E.S.Park J.Y.The accuracy of noninvasive methods in predicting the development of hepatocellular carcinoma and hepatic decompensation in patients with chronic hepatitis BJ Clin Gastroenterol 4620125185252268814610.1097/MCG.0b 013e 31825079 f 1 · doi ↗ · pubmed ↗
- 8Kim M.N.Kim S.U.Kim B.K.Long-term changes of liver stiffness values assessed using transient elastography in patients with chronic hepatitis B receiving entecavir Liver Int 342014121612232426773710.1111/liv.12377 · doi ↗ · pubmed ↗