Mode of Patient Sexual Orientation and Gender Identity Disclosure and Receipt of Tailored Cancer Resources
Victor Basil, Charles Kamen, Austin R. Waters, N. F. N. Scout, Megan A. Mullins

TL;DR
This study finds that how LGBTQ+ cancer patients disclose their identity affects whether they receive tailored resources, suggesting a need for better data collection and care integration.
Contribution
The study introduces a national analysis linking SOGI disclosure modes to receipt of tailored clinical resources for LGBTQ+ cancer survivors.
Findings
LGBTQ+ cancer survivors who self-disclosed or did not disclose SOGI were less likely to receive tailored resources.
Only 38% of participants received at least one LGBTQ+-tailored clinical resource.
Clinic-collected SOGI data was associated with higher odds of receiving tailored care.
Abstract
Is the mode of sexual orientation and gender identity (SOGI) disclosure associated with receipt of clinical resources tailored to LGBTQ+ individuals among cancer survivors? In this cross-sectional study of a national sample of 2342 LGBTQ+ cancer survivors, those who self-disclosed or did not disclose SOGI information were less likely to receive at least 1 LGTBQ+ clinical resource compared with those who had SOGI information collected by the clinic. This study suggests that continued efforts for systematic SOGI data collection and use are needed to improve delivery of tailored resources and care for LGBTQ+ people with cancer. For lesbian, gay, bisexual, transgender, queer, questioning, and other (LGBTQ+) individuals with cancer, disclosing sexual orientation and gender identity (SOGI) in a safe clinical environment can improve survivorship outcomes and satisfaction. Although SOGI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | No. (%) (N = 2342) |
|---|---|
| Sex assigned at birth | |
| Female | 900 (38) |
| Male | 1428 (61) |
| I prefer not to share this information | 14 (1) |
| Physical differences in sexual anatomy at birth (intersex) | |
| No | 2277 (97) |
| Yes | 49 (2) |
| I prefer not to share this information | 16 (1) |
| Gender | |
| Female | 775 (33) |
| Male | 1394 (60) |
| Nonconforming or nonbinary | 101 (4) |
| Transgender | 43 (2) |
| Another gender | 29 (1) |
| Sexual orientation | |
| Bisexual | 116 (5) |
| Gay | 1272 (54) |
| Lesbian | 581 (25) |
| Multiple orientations | 246 (11) |
| Another orientation | 127 (5) |
| Age at cancer diagnosis, y | |
| ≤18 | 39 (2) |
| 19-44 | 572 (24) |
| 45-64 | 1438 (61) |
| ≥65 | 256 (11) |
| Missing | 37 (2) |
| Age at time of survey, y | |
| 18-44 | 270 (12) |
| 45-64 | 1281 (55) |
| ≥65 | 665 (28) |
| Missing | 126 (5) |
| Region of US where patient resides | |
| Midwest | 382 (16) |
| Northeast | 400 (17) |
| South | 574 (25) |
| West | 536 (23) |
| Unknown | 450 (19) |
| Types of cancer | |
| Blood | 305 (13) |
| Breast | 388 (17) |
| Gastrointestinal | 310 (13) |
| Genitourinary | 523 (22) |
| Gynecologic | 192 (8) |
| Lung | 102 (4) |
| Other | 504 (22) |
| Missing | 18 (1) |
| Currently have health insurance | |
| No | 70 (3) |
| Yes | 2164 (92) |
| Unknown | 108 (5) |
| Highest level of education completed | |
| Graduate school | 885 (38) |
| College or vocational school degree or certificate | 864 (37) |
| Some college or vocational school | 381 (16) |
| High school diploma | 75 (3) |
| Some high school | 15 (1) |
| I prefer not to share this information | 7 (<1) |
| Unknown | 115 (5) |
| Race | |
| Black | 79 (3) |
| White | 2019 (86) |
| Other | 90 (4) |
| Multiracial | 64 (3) |
| I prefer not to share this information | 33 (2) |
| Missing | 57 (2) |
| Ethnicity | |
| Hispanic | 136 (6) |
| Non-Hispanic | 2078 (89) |
| Missing | 128 (5) |
| Currently have cancer | |
| No | 1691 (72) |
| Yes | 514 (22) |
| Unknown | 137 (6) |
| Currently receiving cancer treatment | |
| No | 153 (7) |
| Yes | 354 (15) |
| Unknown | 144 (6) |
| No current diagnosis | 1691 (72) |
| Mode of LGBTQ+ identity disclosure | |
| Clinic collected | 994 (42) |
| Self-disclosed | 804 (34) |
| Did not disclose | 288 (12) |
| Don’t know, missing, or other | 256 (11) |
| Disclosure mode | Respondents, No. (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Survivorship plan (n = 1056) | Tobacco resource (n = 342) | Alcohol resource (n = 767) | Physical activity resource (n = 2342) | Mental health resource (n = 2342) | Any resource (n = 2342) | |||||||
| No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | |
| Clinic collected | 397 (38) | 102 (82) | 100 (29) | 36 (11) | 297 (39) | 50 (7) | 857 (38) | 103 (5) | 627 (28) | 318 (14) | 580 (25) | 414 (18) |
| Self-disclosed | 305 (29) | 57 (5) | 95 (28) | 40 (12) | 239 (31) | 29 (4) | 696 (31) | 63 (3) | 203 (9) | 70 (3) | 506 (22) | 298 (13) |
| Did not disclose | 98 (10) | 9 (1) | 33 (10) | 9 (3) | 64 (9) | 11 (1) | 262 (31) | 16 (1) | 168 (8) | 59 (3) | 200 (9) | 88 (4) |
| Do not know, missing, or other | 82 (8) | 6 (1) | 19 (6) | 10 (3) | 66 (9) | 11 (1) | 217 (9) | 19 (1) | 537 (24) | 220 (10) | 164 (7) | 92 (4) |
| .001 | .61 | .57 | .05 | .02 | .004 | |||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLGBTQ Health, Identity, and Policy · Cancer survivorship and care · Family Support in Illness
Introduction
Patient-centered care, a core component of high-quality cancer care, is not only responsive to patient needs and values but is emotionally supportive, allows for involvement of loved ones, and supports informed patient decision-making with information and education.^1,2,3^ To deliver patient-centered care, clinical care teams need to know salient patient identities and relationships. For lesbian, gay, bisexual, transgender, queer, questioning, and other (LGBTQ+) patients, disclosing this information may not always feel safe or welcomed, but evidence shows that LGBTQ+ patients have more satisfaction with care and better survivorship outcomes when they can safety disclose their identities with their clinical care team.^4,5,6,7,8^
Although identity disclosure may happen informally in a clinical encounter, lack of systematic processes to elicit this information respectfully from all patients can result in unequal targeting of patients based on appearance or other staff perceptions, and it burdens patients with fear of disclosure and negative reactions.^4,9,10^ In addition, ad hoc identity disclosure may not be documented at all, or if it is documented, not in a place where it is easily identifiable and useful to clinical staff.^9^ Because discrete data fields facilitate systematic collection, a 2015 policy mandated that electronic health record systems in the US should have the capacity to collect sexual orientation and gender identity (SOGI) data by 2018 under the US Meaningful Use Stage 3 incentive program.^9,11,12^ Although rates of SOGI data collection have increased in recent years, most oncology practices are still not systematically collecting these data from patients, although SOGI data still may be disclosed and used in visits.^12,13^ Given the volume of information in the electronic health record and the lack of SOGI data awareness among clinical teams, it is unknown whether systematic SOGI data collection or informal SOGI disclosure are resulting in increased use of SOGI data in clinical practice.^9,14^ There are numerous ways SOGI data can be used to inform clinical practice, including informing the language used in clinical encounters, referrals to LGBTQ+-specific support groups or clinicians, or provision of clinical resources (such as education about substance use, mental health, or physical activity) that are tailored to the experience of LGBTQ+ patients.^15,16,17^
Several studies have shown that LGBTQ+ individuals with cancer have unmet informational and educational needs and a desire for LGBTQ+-tailored cancer resources.^18,19,20,21^ Tailored resources can address critical population-specific needs and improve clinical outcomes, satisfaction, and engagement.^15,16,20,22,23,24^ To understand the association between mode of SOGI disclosure and use of SOGI data to provide LGBTQ+-tailored resources to patients, we analyzed data from the OUT National Cancer Survey, a national survey of LGBTQ+ cancer survivors.^25^ We evaluated how survivors’ care teams knew their SOGI and whether the mode of identity disclosure was associated with receipt of LGBTQ+-tailored clinical resources for tobacco cessation, mental health, physical activity, alcohol consumption, or cancer survivorship care.
Methods
Study Setting and Participants
The OUT National Cancer Survey, conducted from September 2020 through March 2021, has previously been described in detail.^25,26,27^ In brief, adults (≥18 years) with a self-reported history of a cancer diagnosis who identify as LGBTQ+ and live in the US were eligible and recruited for survey response via online platforms and targeted ad campaigns.^25^ From an initial sample of 4517 respondents, we excluded ineligible individuals, including those who did not report having cancer (n = 488), who did not identify as LGBTQ+ (n = 49), who were not at least 18 years of age (n = 9), and who were outside the US (n = 28) (eFigure in Supplement 1). Because this was a web-based survey, we also took additional steps to identify and exclude fraudulent responses from survey bots and other illegitimate respondents.^28^ To identify fraudulent responses, we deployed a Stata, version 17 (StataCorp LLC) module (checkipaddresses) that queries an IP address verification service to determine if participants were located outside of the US or used a virtual private network or server to mask their true location.^29,30^ A total of 2175 responses were excluded due to ineligibility (n = 574) or being flagged as fraudulent (n = 1601), resulting in a final analytic sample of 2342 LGBTQ+ cancer survivors. The protocol and survey were approved by the Western institutional review board. After confirming eligibility and reading the informed consent form, participants electronically consented to participate. Participation was voluntary and anonymous, and participants were not provided with incentives for participation. This report followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.^31^
Outcome
The primary outcome, receipt of LGBTQ+-tailored clinical resources, was assessed by the following survey questions: “Does your post-treatment care plan include resources for LGBTQ+ individuals?” “Have you ever received resources to help you stop using tobacco that were developed for LGBTQ+ individuals?” “Have you ever received resources related to alcohol consumption developed for LGBTQ+ individuals?” “Have you ever received resources related to physical activity developed for LGBTQ+ individuals?” “Have you ever received resources related to mental health developed for LGBTQ+ individuals?” Response options were “yes,” “no,” and “don’t know/prefer not to answer.” For smoking and alcohol resource reporting, we assessed receipt among those with a smoking history or drinking history. From item-specific responses, a composite variable for receipt of tailored resources (yes or no) was created to indicate receipt of at least 1 type of tailored resource.
Exposure
The primary exposure of interest, mode of SOGI disclosure, was assessed by the survey question “Were/are any of your cancer healthcare professionals aware of your LGBTQ+ identity?” Response options were “yes,” “no,” and “don’t know/prefer not to answer.” Respondents answering “no” were categorized as “did not disclose.” Respondents answering “yes” were asked, “How did this generally come about? (select all that apply).” Responses were grouped into categories: clinic collected (includes responses: “Patient or medical forms gave the option for me to say,” “Health professional asked during a consultation,” “Nurses asked,” and “It is embedded in my medical information”), self-disclosure (includes responses: “Self-disclosed during a consultation”), and don’t know, missing, or other (includes responses: “People can usually tell by my appearance,” “Someone else told the healthcare professional,” and “Something else”). If respondents selected “other” and provided their own text, we assigned the response to the most pertinent category.
Covariates
Other variables examined include respondent clinical and sociodemographic characteristics: sex assigned at birth (male, female, or prefer not to share), physical differences in sexual anatomy at birth (intersex; yes, no, or prefer not to share), gender (female, male, nonconforming or nonbinary [includes genderqueer], transgender, other, or prefer not to share), sexual orientation (lesbian, gay, bisexual, another orientation [includes asexual spectrum, pansexual, queer, and another orientation], or multiple orientations), age when diagnosed with cancer and age at time of survey completion (18-44 years, 45-64 years, ≥65 years, or missing), region of US where patient resides (Northeast, Midwest, South, West, or unknown), cancer type (blood, breast, gastrointestinal, genitourinary, gynecologic, lung, other, missing, or unknown), currently have health insurance (yes, no, or unknown), highest level of education completed (some high school, high school diploma, some college or vocational school, college or vocational school degree or certificate, graduate school, unknown or missing), ethnicity (Hispanic, non-Hispanic, or prefer not to share), current cancer diagnosis (yes, no, or unknown), and currently participating in treatment (yes, no, unknown, or no current diagnosis). Race was collapsed into Black, White, another racial minority (including Alaska Native, American Indian, Asian or Asian American, Middle Eastern or North African, Native Hawaiian or Pacific Islander, and a text value for “a racial identity not listed here”), multiracial, and prefer not to share. Participants self-identified their race in the survey. Race and ethnicity data were collected to further understand and describe the participants in this study. LGBTQ+ identities, their salience, and their disclosure can differ across racial and ethnic identities.
Statistical Analysis
Bivariate analyses were conducted using χ^2^ tests to assess unadjusted associations between SOGI disclosure mode and receipt of each individual tailored resource (tobacco cessation, alcohol use, physical activity, mental health, posttreatment care, and general LGBTQ+ cancer information). A multivariable logistic regression model was used to examine the association between mode of SOGI disclosure and receipt of at least 1 LGBTQ+-tailored clinical resource, adjusted for US region of residence, age at cancer diagnosis, current cancer diagnosis status (yes or no), and type of cancer. Missing values for variables that did not require an answer to submit the assessment were listed as missing or were collapsed into the category “unknown” with responses “other” and “don’t know.” A 2-sided P < .05 was statistically significant. Analyses were conducted using SAS, version 9.4 (SAS Institute Inc).
Results
This national sample of 2342 LGBTQ+ cancer survivors (mean [SD] age, 58.4 [16.7] years; 1428 assigned male at birth [61%] and 900 assigned female at birth [38%]) included 79 Black participants (3%), 136 Hispanic participants (6%), 2019 White participants (86%), 64 multiracial participants (3%), and 90 participants of other race or ethnicity (4%) (Table 1). More than half of the respondents were cisgender males (1394 [60%]), followed by cisgender females (775 [33%]), nonbinary or nonconforming individuals (101 [4%]), transgender individuals (43 [2%]), and individuals of another gender (29 [1%]). Most participants reported gay sexual orientation (1272 [54%]), followed by lesbian (581 [25%]), multiple orientations (246 [11%]), another orientation (127 [5%]), and bisexual (116 [5%]). Most participants received a diagnosis of cancer between the ages of 45 and 64 years (1438 [61%]). Almost one-fourth of respondents (514 [22%]) had cancer at the time of survey completion. Respondents reported many different types of cancer, with genitourinary cancers being the most common (523 [22%]).
Most respondents (1798 [77%]) indicated that their care team knew their LGBTQ+ identity, with disclosure most often via self-disclosure (804 [34%]) or clinic collection (944 [42%]). Table 2 presents data on LGBTQ+-tailored resource receipt by the mode of SOGI disclosure. The most commonly reported tailored resource was the LGBTQ+ mental health resource (667 [28%]) and the LGBTQ+-tailored resource for tobacco cessation (95 of 342 reported smokers [28%]). Only 174 respondents (7%) received an LGBTQ+ survivorship care plan, and 892 (38%) received at least 1 resource tailored to LGBTQ+ individuals. Overall, more patients whose SOGI data were collected by the clinic received at least 1 tailored resource (414 [18%]), compared with those who self-disclosed (298 [13%]) or did not disclose (88 [4%]) (P < .001). Participants who did not disclose their identity received the fewest tailored resources across all resource types.
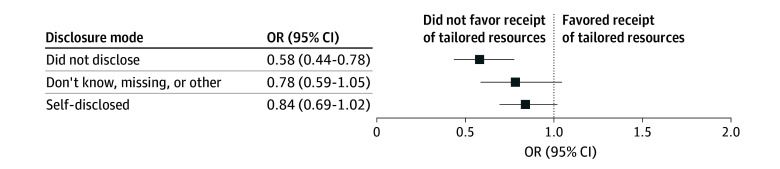
In the adjusted model, participants who did not disclose their SOGI information had significantly lower odds of receiving at least 1 tailored resource compared with those whose clinic intentionally collected SOGI information (odds ratio, 0.58 [95% CI, 0.44-0.78]) (Figure). Although not a statistically significant difference, those who self-disclosed also had lower odds of tailored resource receipt compared with those whose clinic intentionally collected SOGI information (odds ratio, 0.84 [95% CI, 0.69-1.02]).
Adjusted Odds Ratios (ORs) for Receipt of a Lesbian, Gay, Bisexual, Transgender, Queer, Questioning, and Other–Tailored Resource for OUT National Cancer Survey Respondents Who Disclosed Sexual Orientation and Gender Identity to Their Clinical Team vs Those Who Did NotThe logistic regression model includes adjustments for US region, cancer type, age at cancer diagnosis, and current cancer, allowing for estimation of the association between identity disclosure category and receipt of tailored resources while controlling for these covariates.
Discussion
In this national study of LGBTQ+ cancer survivors, most respondents (approximately 90%) reported that their care team was aware of their LGBTQ+ identity, but only one-third (38%) received an LGBTQ+-tailored resource. Receipt of tailored resources was most common among individuals whose clinic collected their SOGI information. With much of the literature focused on SOGI data collection, to our knowledge, this is the first study to assess the relevance of mode of SOGI disclosure or its use in provision of tailored clinical resources for LGBTQ+ patients with cancer, a critical first step toward precision cancer care for LGBTQ+ patients.
As demonstrated in other studies, continued efforts to implement clinic-led SOGI data collection are needed, as less than half (42%) of the reported SOGI disclosures were clinic collected.^12,13,32,33^ Approximately one-third of identity disclosures were self-disclosed without clinic solicitation. Although identity disclosure may happen easily in the course of a clinical encounter, it can also cause additional distress and emotional burden to patients and their caregivers if they deliberate whether or not to disclose their identity or fear negative reactions.^4,10^ The large proportion of patients disclosing their identities illustrates the salience of LGBTQ+ cultural competence and general familiarity with SOGI among clinical staff to ensure these disclosures are handled safely and respectfully.^9,34,35,36,37^
Our findings suggest efforts to use SOGI more intentionally in clinical care are needed. Disclosure of SOGI has been associated with improved rates of engagement in preventive care, treatment adherence, and satisfaction with care.^15,23,32^ Although safe disclosure may facilitate better outcomes through a patient feeling seen and free to bring themselves holistically to their clinical care, it can also be used to deliver tailored resources that patients value. In a prior analysis of OUT Cancer Survey data, Burnett and colleagues^19^ found that 57% of respondents felt that a survivorship care plan with LGBTQ+ information was important, and 80% of respondents agreed that LGBTQ+ mental health resources were valuable; however, in our study, approximately 10% of survivorship care plan recipients received tailored information, and approximately one-third received a tailored mental health resource. These rates were higher when clinics intentionally collected SOGI information compared with when patients self-disclosed or did not disclose SOGI information. Intentional data collection populated into discrete fields may be more visible within the electronic health record display than identities buried in clinical notes.^38^ This information could also help connect patients to tailored resources, not only written materials with LGBTQ+ content but also caregiver resources for LGBTQ+ caregivers, support groups, inclusive clinician lists for ancillary services such as mental health and counseling, or inclusive and welcoming gyms for physical activity to ameliorate cancer fatigue and improve mental health.^10,39,40^ Similar to the requisite trainings on how to collect SOGI data, training and other supports are needed to support clinicians in learning how to use SOGI data.^32^
Limitations
The study has some limitations. Our online national survey approach afforded a substantial sample size from diverse US locations and enabled participation from people who may not be actively engaged with a health care system. However, online surveys without identity verification are susceptible to fraudulent responses. It is possible that our method of removing potential fraudulent responses could have removed legitimate responses from individuals who were using a virtual proxy network, and we may have failed to capture all true fraudulent responses. Given the anonymity of the survey and our available data, we were unable to conduct a bias analysis. Future studies should warn potential participants to turn off their virtual proxy network prior to participating to avoid this issue. Second, because we used convenience sampling without a known denominator, we cannot ascertain a response rate or selection bias among those who participated. Despite intentional recruitment to produce a diverse sample, the sample included many White participants who were assigned male at birth and highly educated, which may impact generalizability. We also could not link to any medical records to verify self-reports of cancer. Systematic SOGI data collection across clinical settings is critical to facilitate future large-scale population-based surveys of LGBTQ+ cancer survivors. Given the lack of generalizable information available on LGBTQ+ cancer survivors, this large sample offers an important starting point for understanding how SOGI data are being used to provide tailored resources.
Conclusions
In this cross-sectional study of a national sample of LGBTQ+ cancer survivors, identity disclosure was common, but using that disclosure to provide tailored resources was not, especially in settings in which disclosure was not through clinic collection of SOGI data. Future studies should focus not only on SOGI data collection but also clinical use of SOGI data and the effectiveness of SOGI-tailored resources for improving patient outcomes. Systematic SOGI data collection will facilitate survey studies in the future for this understudied but growing population to better understand health disparities and outcomes for sexual and gender minority patients, contributing to the development of high-quality, patient-centered care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press; 2001. Accessed May 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK 222274/25057539 · pubmed ↗
- 2Institute of Medicine. Delivering High Quality Cancer Care: Charting a New Course for a System in Crisis. National Academies Press; 2013.24872984 · pubmed ↗
- 3Gerteis M, Edgman-Levitan S, Daley J, Delbanco TL, eds. Through the Patient’s Eyes: Understanding and Promoting Patient-Centered Care. Jossey-Bass; 2002.
- 4Power R, Ussher JM, Allison K, Hawkey A, Perz J; Out with Cancer Study Team. “A sweating moment”: impact of disclosure in cancer care on LGBTQI patient satisfaction. J Cancer Surviv. Published online September 21, 2024. doi:10.1007/s 11764-024-01677-1 39305389 PMC 12988887 · doi ↗ · pubmed ↗
- 5Seay J, Mitteldorf D, Yankie A, Pirl WF, Kobetz E, Schlumbrecht M. Survivorship care needs among LGBT cancer survivors. J Psychosoc Oncol. 2018;36(4):393-405. doi:10.1080/07347332.2018.1447528 29791273 · doi ↗ · pubmed ↗
- 6Katz A. Gay and lesbian patients with cancer. Oncol Nurs Forum. 2009;36(2):203-207. doi:10.1188/09.ONF.203-207 19273409 · doi ↗ · pubmed ↗
- 7Crangle CJ, Latini DM, Hart TL. The effects of attachment and outness on illness adjustment among gay men with prostate cancer. Psychooncology. 2017;26(4):500-507. doi:10.1002/pon.4043 26626273 PMC 6461036 · doi ↗ · pubmed ↗
- 8Kamen C, Jabson JM, Mustian KM, Boehmer U. Minority stress, psychosocial resources, and psychological distress among sexual minority breast cancer survivors. Health Psychol. 2017;36(6):529-537. doi:10.1037/hea 0000465 28165265 PMC 5444950 · doi ↗ · pubmed ↗