Unicuspid Aortic Valve Disease: The Role of Imaging in Diagnosis and Timely Surgical Planning
Mehak Gupta, Aaditya Kodamanchile, Marina Zafeiri, Pavithralakshmi Venkatraghavan, Andrew Cole

TL;DR
This paper discusses a rare heart valve condition misdiagnosed as a more common one, emphasizing the importance of accurate imaging for timely treatment.
Contribution
The paper highlights the diagnostic challenges of unicuspid aortic valve disease and the critical role of transesophageal echocardiography.
Findings
Unicuspid aortic valve is often misdiagnosed as bicuspid aortic valve using standard imaging techniques.
Transesophageal echocardiography is crucial for accurate diagnosis and surgical planning in UAV cases.
Delayed diagnosis of UAV can lead to severe complications requiring urgent surgery.
Abstract
Unicuspid aortic valve (UAV) is a rare congenital anomaly that is often misdiagnosed as bicuspid aortic valve (BAV). UAV is associated with faster clinical progression, earlier need for surgical intervention, and a higher risk of complications. Accurate diagnosis is therefore crucial for timely management. We report the case of a 31-year-old male with a family history of BAV, who had been followed for more than 15 years with a presumed diagnosis of BAV. Serial transthoracic echocardiograms (TTEs) and cardiac MRI consistently suggested a bicuspid morphology. A previous transesophageal echocardiogram (TOE) was poorly tolerated. Despite progressive aortic regurgitation and root dilation, the diagnosis remained unchanged until the patient developed exertional dyspnea and presyncope. A repeat TOE revealed a unicuspid valve with severe eccentric regurgitation, which was later confirmed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
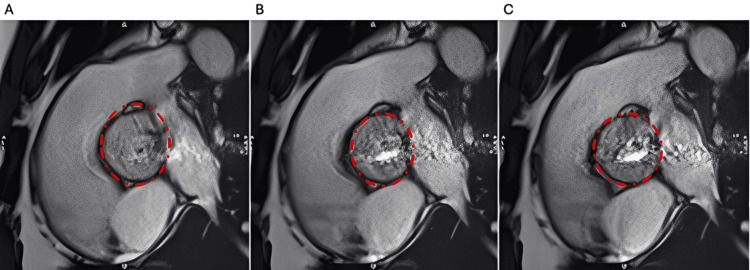 Figure 1
Figure 1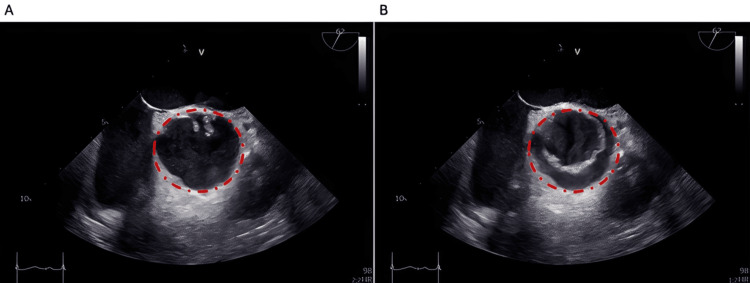 Figure 2
Figure 2| Feature | UAV | BAV |
| Prevalence | 0.02-0.06% (rare) | 1-2% (more common) |
| Valve morphology | Single commissure (unicommissural) or none (acommissural) | Two commissures with asymmetric leaflet fusion |
| Diagnostic challenge | Often misdiagnosed as BAV on TTE/MRI | Usually identifiable, though variants exist |
| Progression | More rapid, earlier degeneration | Slower progression |
| Age at surgery | 20-30 years earlier than tricuspid; ~10-20 years earlier than BAV | Typically, middle-aged or older adults |
| Common pathology | Aortic stenosis (most frequent), severe AR, root dilatation | Aortic stenosis with/without regurgitation; root dilatation |
| Risk of complications | High risk of dissection, aneurysm, and root enlargement | Elevated risk, but generally later onset |
| Best imaging modality | TOE (superior resolution for commissures) | TTE sufficient in most cases |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Infective Endocarditis Diagnosis and Management
Introduction
Unicuspid aortic valve (UAV) is a rare congenital anomaly, with an estimated prevalence of 0.02-0.06% [1,2]. UAV may be either unicommissural or acommissural and is frequently misclassified as a bicuspid aortic valve (BAV) because of overlapping echocardiographic features [3]. Unlike BAV, UAV progresses more rapidly, and patients often require aortic valve replacement (AVR) one to two decades earlier [4].
Here, we present the case of a patient with a UAV that was misdiagnosed as BAV for more than 15 years, highlighting the importance of multimodal imaging and timely diagnosis.
Case presentation
A 31-year-old male with a family history of BAV and aortic regurgitation (AR) (brother diagnosed at age 13) was referred to cardiology services in 2007. His initial transthoracic echocardiogram (TTE) revealed mild AR, a left ventricular ejection fraction (LVEF) of 45%, and raised suspicion of BAV, although valve morphology could not be clearly visualized. Following this, he underwent yearly serial TTEs. From 2007 through 2020, there were no significant changes in his echocardiographic findings, and clinically, he remained asymptomatic.
In 2020, his TTE showed progression of AR into the moderate range, with a mild increase in left ventricular (LV) cavity size. He subsequently underwent a transesophageal echocardiogram (TOE), which he did not tolerate well. The suboptimal images obtained appeared to show moderate AR with a dilated LV and moderately impaired systolic function (LVEF 45%). His aortic dimensions were normal for his body surface area. As he remained clinically asymptomatic at this point, he continued with yearly TTE surveillance.
In 2024, he developed exertional breathlessness and dizziness. A repeat TTE, which did not adequately visualize the aorta, showed a significantly dilated LV with an LVEF of 48% and at least moderate AR. His AR appeared complex, with two distinct jets, raising concern that its severity was being underestimated. To further characterize his aortic dimensions, he underwent CT cardiac angiography, which revealed a dilated aortic root measuring 42 × 30 mm and an ascending aorta measuring 43 mm, with a BAV. Cardiac MRI subsequently demonstrated a moderately dilated LV (LVEF 54%), with the aortic valve again reported as bicuspid morphology with severe AR (Figure 1).
Cardiac MRI still frames of a UAV obtained with SSFP cine sequences during different phases of the cardiac cycle: (A) diastole, (B) mid-systole, and (C) end-systoleThe red dashed circle indicates the aortic valve.SSFP, steady-state free precession; UAV, unicuspid aortic valve
He later underwent a repeat TOE, which showed a mildly stenotic UAV with severe eccentric regurgitation and a dilated LV (LVEF 51%) (Figure 2). His case was discussed at a valve multidisciplinary team (MDT) meeting. On re-review of his previous imaging, the MRI was considered to show a UAV. The MDT recommended surgical intervention with replacement of the aortic valve, aortic root, and ascending aorta.
Transesophageal echocardiographic images of a UAV in (A) diastole and (B) systole, obtained in the short-axis aortic viewThe red dashed circle indicates the aortic valve.UAV, unicuspid aortic valve
He underwent a modified Bentall procedure with replacement of the ascending aorta using a 27 mm On-X composite Valsalva graft. The operation was carried out routinely, with a total cross-clamp time of 334 minutes and a bypass time of 385 minutes. Intraoperative inspection of the native aortic valve confirmed a UAV.
Discussion
This case highlights the limitations of TTE and cardiac MRI in diagnosing UAV, particularly when overlapping features with BAV are present. TTE is widely used as the first-line imaging modality to assess valvular pathology because of its availability and tolerability. However, it is often inadequate as a sole technique due to restricted acoustic windows. Cardiac MRI cine imaging is generally robust for functional and morphological assessment, but in this case, the interpretation of the aortic valve was likely influenced by anchoring bias from the long-standing assumption and repeated reports of BAV, resulting in misclassification despite adequate image quality [5,6].
In certain cases, TOE, with its superior resolution and proximity to the aortic valve, provides additional information for assessing valve morphology and the fusion pattern characteristic of UAV [7]. However, because TOE is more invasive, patients often find it difficult to tolerate.
In this case, delayed recognition of the UAV may have influenced the intensity of surveillance and the timing of intervention. More importantly, it illustrates the effect of anchoring bias, where the initial assumption of BAV, reinforced by repeated TTE and MRI reports, led clinicians to discount alternative diagnoses despite progressive changes. Awareness of such cognitive bias is critical in rare congenital anomalies to prevent diagnostic delays.
Clinically, UAV has implications beyond valve replacement, as it carries a higher risk of root dilatation and the need for concomitant aortic surgery (Table 1). UAV is associated with early development of aortic root dilation and AR and therefore predominantly affects younger patients, in whom aortic surgery is the main consideration. A subset of patients may not be suitable candidates for surgery; although the role of transcatheter AVR remains limited at present, it may emerge as a treatment option for frailer, high-risk surgical candidates [8].
UAV and BAV share a common genetic predisposition, but UAV appears to represent a more severe phenotype, with earlier onset and faster progression of aortic stenosis. One study comparing UAV and BAV demonstrated that patients with UAV had smaller indexed aortic valve areas and higher mean and peak gradients than those with BAV. This supports the concept of UAV as a more aggressive phenotype within the BAV spectrum, presenting with more severe pathology at a younger age [9]. Given the family history in this case, genetic predisposition should be considered, and early, detailed imaging of first-degree relatives may be warranted.
Conclusions
We report a rare case of a UAV misdiagnosed as BAV for more than 15 years, ultimately identified by TOE and confirmed intraoperatively. We suspect that this prolonged misdiagnosis was influenced by anchoring bias. This case underscores the importance of employing multimodality imaging in the evaluation of valvular pathology and highlights the need for independent image review to minimize reliance on prior reports.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The unicuspid aortic valve Cardiovasc J Afr Yuan SM Jing H Lavee J 113114212010 https://pubmed.ncbi.nlm.nih.gov/20532437/20532437 PMC 5566075 · pubmed ↗
- 2Unicuspid aortic valve: demographics, comorbidities, echocardiographic features, and long-term outcomes Circulation Slostad BD Witt CM O'Leary PW Maleszewski JJ Scott CG Dearani JA Pellikka PA 1853185514020193176526210.1161/CIRCULATIONAHA.119.041835 · doi ↗ · pubmed ↗
- 3Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation Circulation Roberts WC Ko JM 92092511120051571075810.1161/01.CIR.0000155623.48408.C 5 · doi ↗ · pubmed ↗
- 4Unicuspid aortic valve in adults: a systematic review J Heart Valve Dis Mookadam F Thota VR Garcia-Lopez AM Emani UR Alharthi MS Zamorano J Khandheria BK 7985192010 https://pubmed.ncbi.nlm.nih.gov/20329493/20329493 · pubmed ↗
- 52020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines J Am Coll Cardiol Otto CM Nishimura RA Bonow RO 4505007720213334258710.1016/j.jacc.2020.11.035 · doi ↗ · pubmed ↗
- 6Considerations in the surgical management of unicuspid aortic stenosis Pediatr Cardiol Gorton AJ Anderson EP Reimer JA Abdelhady K Sawaqed R Massad MG 99310014220213404780910.1007/s 00246-021-02541-0 · doi ↗ · pubmed ↗
- 7Aortic valve embryology, mechanobiology, and second messenger pathways: implications for clinical practice J Cardiovasc Dev Dis Notenboom ML Van Hoof L Schuermans A Takkenberg JJ Rega FR Taverne YJ 491120243839226310.3390/jcdd 11020049 PMC 10888685 · doi ↗ · pubmed ↗
- 8Transcatheter aortic valve implantation in unicuspid aortic valve stenosis Euro Intervention Chopra A Uthayakumaran K Rao RS Ajit MS 0315202010.4244/EIJ-D-20-0007632038028 · doi ↗ · pubmed ↗