Healing Right Way: A Stepped Wedge Cluster Randomised Controlled Trial Aiming to Enhance Quality of Life for Aboriginal Australian Survivors of Stroke and Traumatic Brain Injury
Elizabeth Armstrong, Tapan Rai, Judith M. Katzenellenbogen, Sandra J. Thompson, Meaghan McAllister, Natalie Ciccone, Deborah Hersh, Leon Flicker, Dominique A. Cadilhac, Erin Godecke, Graeme J. Hankey, Neil Drew, Colleen Hayward, Deborah Woods, Mel Robinson, Ivan Lin

TL;DR
A study tested cultural training and support for Aboriginal Australians recovering from brain injuries but found no significant improvement in quality of life.
Contribution
This study evaluates the feasibility and impact of cultural security training and Aboriginal Brain Injury Coordinators in rural healthcare settings.
Findings
Cultural security training and Brain Injury Coordinators improved care processes but not health outcomes.
Hospital compliance with minimum processes of care improved by 6.8% in the intervention group.
Quality of life scores showed no significant difference between groups.
Abstract
To determine the effect of cultural security training (CST) for health professionals and access to an Aboriginal Brain Injury Coordinator (ABIC) for Aboriginal Australians with stroke or traumatic brain injury (TBI). A stepped wedge cluster randomised controlled trial; the intervention package consisted of CST for hospital professionals and 6‐month access to ABICs providing education, support, liaison and advocacy; the commencement order of the intervention phase was randomised. Four urban and four rural hospitals in Western Australia, 2018–2022. Aboriginal adults ≥ 18 years hospitalised with stroke or TBI. Primary outcome was quality of life (Euro QOL–5D‐3L Visual Analogue Scale (EQ‐VAS)) score at 26 weeks post‐injury. Secondary outcomes were modified Rankin Scale, Functional Independence Measure, Hospital Anxiety and Depression Scale, Modified Caregiver Strain Index at 12 and 26…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
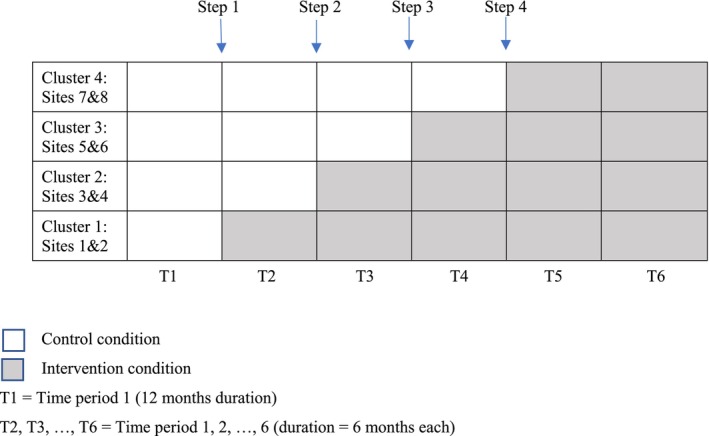 FIGURE 1
FIGURE 1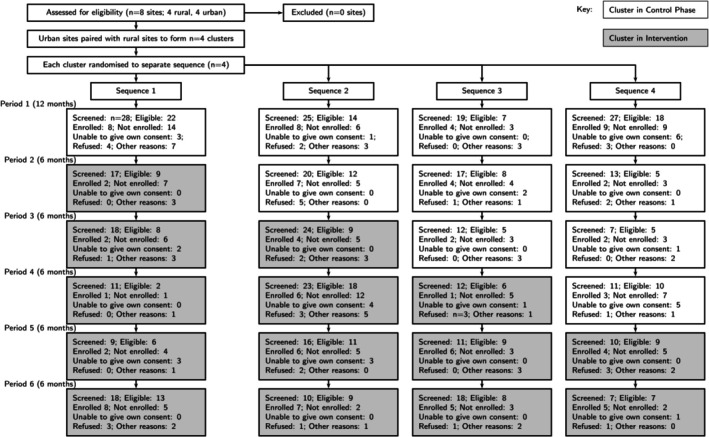 FIGURE 2
FIGURE 2| Control | Intervention | All | |
|---|---|---|---|
|
|
|
| |
| Recruitment region | |||
| Metropolitan | 35 (74.5%) | 51 (83.6%) | 86 (79.6%) |
| Regional | 12 (25.5%) | 10 (16.4%) | 22 (20.4%) |
| Patient details | |||
| Age median (IQR) | 55.7 (15) | 53.6 (20.2) | 55.1 (14.9) |
| < 65 | 38 (81%) | 50 (82%) | 88 (81%) |
| 65–80 | 8 (17%) | 10 (16%) | 18 (17%) |
| > 80 | 1 (2%) | 1 (2%) | 2 (2%) |
| Gender | |||
| Male | 26 (55%) | 38 (62%) | 64 (59%) |
| Female | 21 (45%) | 23 (38%) | 44 (41%) |
| Other/not disclosed | 0 (0%) | 0 (0%) | 0 (0%) |
| Place of residence prior to brain injury | |||
| Perth metro | 11 (23.4%) | 16 (26.2%) | 27 (25%) |
| Regional town | 22 (46.8%) | 35 (57.4%) | 57 (53%) |
| Aboriginal community | 11 (23.4%) | 5 (8.2%) | 16 (15%) |
| Not recorded | 3 (6.4%) | 5 (8.2%) | 8 (7%) |
| Living arrangements prior to brain injury | |||
| Home (alone) | 5 (11%) | 9 (14.8%) | 14 (13%) |
| Home (with others) | 41 (87%) | 50 (82%) | 91 (84%) |
| Supported accommodation, for example, nursing home, hostel | 1 (2%) | 0 (0%) | 1 (1%) |
| No fixed home | 0 (0%) | 1 (1.6%) | 1 (1%) |
| Other | 0 (0%) | 1 (1.6%) | 1 (1%) |
| Injury type | |||
| TBI | 3 (6%) | 16 (26%) | 19 (18%) |
| Stroke | 44 (94%) | 45 (74%) | 89 (82%) |
| Injury severity | N/A | mRS used | instead |
| Baseline mRS (binary) | |||
| Independent (0–2) | 7 (15%) | 13 (21%) | 20 (19%) |
| Dependent/dead (3–6) | 40 (85%) | 48 (79%) | 88 (81%) |
| Baseline HADS | |||
| Anxiety mean (SD) |
7.8 (4.7) [ |
7.7 (4.1) [ |
7.8 (4.3) [ |
| Depression mean (SD) |
5.6 (4.1) [ |
6.1 (4.2) [ |
5.9 (4.2) [ |
| Baseline FIM mean (SD) | 91 (29) | 92.7 (28.7) | 91.9 (28.8) |
| Alcohol consumption (Yes) |
20 (61%) [ |
28 (74%) [ |
48 (68%) [ |
| Drug use (Yes) |
10 (30%) [ |
11 (29%) [ |
21 (30%) [ |
| Diabetes (Yes) | 33 (70%) | 34 (56%) | 67 (62%) |
| Heart disease (Yes) [ischaemic heart disease] | 23 (49%) | 15 (25%) | 38 (35%) |
| Participant's primary language spoken | No. |
|---|---|
| English | 73 |
| Ngadju | 1 |
| Ngaatjatjara | 1 |
| Miriwoong | 2 |
| Ngarinyin | 1 |
| Walmajarri | 6 |
| Walpiri | 1 |
| Yulparija | 1 |
| Kija | 1 |
| Wajarri | 2 |
| Kukatja | 1 |
| Banyjima | 1 |
| Martuthunira | 3 |
| Ngarluma | 1 |
| Nyangumarta | 2 |
| Martuwangka | 1 |
| Nyungar | 9 |
| Not recorded | 1 |
| All mean (SD) | Control mean (SD) | Intervention mean (SD) | Unadjusted analysis | Adjusted analysis | |||
|---|---|---|---|---|---|---|---|
| Mean difference (95% CI) |
| Mean difference (95% CI) |
| ||||
| Primary outcome measure | |||||||
| EuroQoL‐5D‐3L‐VAS | 64.7 (18.8) | 70.6 (19.3) | 60.5 (17.4) | −10.1 (−17.9, −2.3) | 0.02 | −2.2 (−20.1, 15.7) | 0.81 |
| Secondary participant‐level outcomes | |||||||
| mRS (binary) | [ | [ | [ | ||||
| Independent (0–2) | 36 (39%) | 19 (49%) | 17 (32%) | OR = 2.0 | 0.11 | OR = 1.3 | 0.20 |
| Dependent/dead (3–6) | 56 (61%) | 20 (51%) | 36 (68%) | (0.8, 5.1) | (0.1, 14.9) | ||
| FIM |
105 (21) [ |
106.2 (24.1) [ |
104.0 (18.6) [ | −2.2 (−7.2, 11.7) | 0.64 | −6.5 (−23.6, 10.6) | 0.45 |
| HADS | [ | [ | [ | ||||
| HADS: anxiety | 6 (3.8) | 5.4 (3.6) | 6.5 (4) | 1.1 (−0.63, 2.8) | 0.21 | 1.8 (−1.0, 4.6) | 0.19 |
| HADS: depression | 4.7 (3.2) | 4.1 (3.3) | 5.3 (3.1) | 1.2 (−0.2, 2.7) | 0.09 | 2.9 (0.4, 5.5) | 0.03 |
| Modified Caregiver Strain Index |
8.8 (7.0) [ |
6.3 (3.4) [ |
10.7 (8.5) [ | 4.4 (−0.8, 9.7) | 0.09 | — | — |
| System‐level outcomes | [ | [ | [ | ||||
| Proportion of minimum processes of care achieved | 52% (18) | 48% (20) | 55% (16) | 7% (−0.6, 14.1) | 0.07 | 7% (0.1, 13.9) | 52% (18) |
| Occasions of service | 72.5 (76.6) | 61.8 (61.7) | 80.7 (85.9) | 18.9 (−9.3, 47.0) | 0.19 | −0.84 (−33.3, 31.6) | 0.96 |
| All mean (SD) | Control mean (SD) | Intervention mean (SD) | Unadjusted analysis | Adjusted analysis | |||
|---|---|---|---|---|---|---|---|
| Mean difference (95% CI) |
| Mean difference (95% CI) |
| ||||
| Primary outcome measure | |||||||
| EuroQoL‐5D‐3L‐VAS | 64.7 (19.6) | 70.1 (21.0) | 61.1 (17.9) | −11.0 (−17.8, −0.2) | 0.046 | −1.7 (−17.6, 14.1) | 0.83 |
| Secondary participant‐level outcomes | |||||||
| mRS (binary) | [ | [ | [ | ||||
| Independent (0–2) | 34 (39%) | 21 (55%) | 13 (26%) | OR = 3.5 (1.3, 9.5) | 0.008 | OR = 3.1 | 0.38 |
| Dependent/dead (3–6) | 54 (61%) | 17 (46%) | 37 (74%) | (0.3, 37.4) | |||
| FIM | 103.7 (23.6) | 105.9 (26.9) | 102.2 (21.3) | −3.7 (−14.7, 7.3) | 0.51 | −1.9 (−19.1, 15.2) | 0.82 |
| HADS | [ | [ | [ | ||||
| HADS: anxiety | 6.4 (3.9) | 6.0 (3.4) | 6.7 (4.3) | 0.7 (−1.0, 2.5) | 0.41 | 1.7 (−1.1, 4.5) | 0.24 |
| HADS: depression | 5.7 (4.2) | 5.3 (4.3) | 6.0 (4.0) | 0.7 (−1.3, 2.6) | 0.50 | 1.9 (−0.7, 4.6) | 0.15 |
| Modified Caregiver Strain Index |
9.9 (8.0) [ |
6.7 (6.9) [ |
12.8 (8.1) [ | 6.1 (−12.9, 0.7) | 0.08 | — | — |
| System‐level outcomes | [ | [ | [ | ||||
| Proportion of minimum processes of care achieved | 54% (18) | 51% (19) | 57% (16) | 6% (−13.4, 1.0) | 0.10 | 6.8% (0.4, 13.3) | 0.038 |
| Occasions of service | 81.4 (108) | 69.7 (69.7) | 90.4 (102.6) | 20.7 (−12.2, 53.7) | 0.21 | 4.23 (−26.2, 34.6) | 0.78 |
- —National Health and Medical Research Council10.13039/501100000925
- —Royal Perth Hospital Medical Research Foundation10.13039/100012505
- —Western Australian Department of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury Research · Spinal Cord Injury Research · Cardiac Arrest and Resuscitation
Summary
-
What this paper adds
-
○We report the first stepped wedge randomised controlled trial conducted in the area of brain injury in Aboriginal populations, with the first follow‐up data at 6 months for this predominantly rural‐located population.
-
○The paper constitutes one of the few intervention studies conducted in the area of brain injury in Aboriginal populations.
-
○This is the first clinical trial in the area and the first to evaluate the role of an Aboriginal Brain Injury Coordinator to assist with recovery.
-
○The combination of cultural security training for health professionals and provision of an Aboriginal Brain injury Coordinator for Aboriginal Australians with stroke and traumatic brain injury within the Western Australian context was feasible, acceptable, safe and improved care provided across metropolitan, rural and remote areas.
-
○This pragmatic real‐world trial of a complex intervention was able to be implemented and improved care despite significant challenges including the COVID‐19 epidemic.
-
○The study provides a networked model for both future research and clinical services in metropolitan, rural and remote communities.
-
What is already known on this subject?
-
○There is a high incidence of stroke and traumatic brain injury in Aboriginal Australian communities.
-
○Continuity of care post‐hospital discharge is sub‐optimal, with culturally secure care hampered by distance from Country and varying cultural awareness among hospital staff.
-
○From the limited research conducted in this area to date, it has been recommended that more Aboriginal staff be involved in rehabilitation and that non‐Aboriginal clinicians receive cultural training.
Introduction
1
Aboriginal and Torres Strait Islander (respectfully Aboriginal) peoples in Australia who are hospitalised with stroke or traumatic brain injury (TBI) frequently experience isolation from their home, family and culture. Many live in regional, rural and remote areas [1, 2, 3] and are initially transferred to a metropolitan centre for acute care. Their care may be compromised by health service provider ignorance of Aboriginal culture, the impacts of colonisation and ineffective communication [4, 5, 6, 7].
This study was based in Western Australia (WA) where most Indigenous people are Aboriginal, yet culturally diverse, with multiple language groups living across the vast, sparsely populated state. We thus respectfully refer to Aboriginal (rather than Torres Strait Islander) peoples throughout. The varying cultural protocols, languages and traditions across the state are relevant to service provision planning and delivery.
The Healing Right Way (HRW) trial was developed in response to the recommendations of Aboriginal people with a stroke or TBI, [4, 5, 6] with high incidence of both in communities [1, 2, 3, 7, 8]. More culturally secure experiences during hospital stays following brain injury, including better communication between non‐Aboriginal health professionals and Aboriginal patients and increased support following discharge from hospital, were needed. Research showed more Aboriginal health professionals should be involved in rehabilitation care, and non‐Aboriginal clinicians requested further cultural training [9]. No previous clinical trials in rehabilitation and few intervention reports were noted for Aboriginal people after stroke or TBI.
The aim of the HRW multicentre trial was to develop, implement and evaluate an Intervention Package within WA to improve the quality of life for Aboriginal people with stroke or TBI within 26 weeks post‐injury compared to usual care. Our secondary hypotheses included significantly greater functional and emotional improvements in participants in the intervention group at 12 and 26 weeks and improvements in service delivery (outlined below). We also hypothesised that the package would be acceptable to Aboriginal participants and their families and health professionals and be feasible to implement.
The COVID‐19 pandemic began midway through the trial, affecting most of the intervention phase of the study. The trial continued throughout the pandemic. This paper includes reference to the effects of this extenuating circumstance on HRW and adaptations made to accommodate its effects.
Methods
2
The trial rationale and design have been previously described [10, 11]. Reporting is aligned with Consolidated Standards of Reporting Trials extension statement on the reporting of stepped wedge cluster randomised control trials (CRCTs) [12] and the Guidelines for Reporting Trial Protocols and Completed Trials Modified Due to the COVID‐19 Pandemic and Other Extenuating Circumstances: The 2021 CONSERVE Statement [13].
Study Design
2.1
Stepped wedge cluster randomised controlled trial. The trial design was based on principles aligned with an Aboriginal Research Framework [14] and Indigenous Standpoint Theory [15]. These included Aboriginal leadership; acknowledgment of colonisation as a social determinant of health/disability; acknowledgment of the diversity of Aboriginal communities; and Aboriginal community capacity building. See Appendix A for details of the trial's alignment with guidelines for health research involving Aboriginal and Torres Strait Islander peoples (the CONSIDER Statement Checklist) [16].
Setting
2.2
The eight hospital sites (four rural and four urban) were located in Western Australia.
Randomisation
2.3
Each rural site was paired to an urban site. Each pair was treated as a cluster, and each urban–rural cluster was randomised to one of four sequences which determined the order of commencement of the intervention phase (see study protocol for further detail) [10].
All sites commenced in the control phase, during which baseline data were collected (Figure 1). The first sequence crossed over into the intervention phase at the end of 52 weeks and remained in intervention for the remainder of the trial. The remaining sequences switched to the intervention phase at 26‐week intervals. Starting at 130 weeks, all sites were in the intervention phase, so that at the end of 156 weeks, each cluster had achieved at least 26 weeks of enrolment in the intervention phase.
Stepped wedge design.
During the trial, external factors impacted recruitment including the COVID‐19 pandemic and changes to next‐of‐kin consent legislation in WA [17]. Due to slower than predicted recruitment at the commencement of the trial, the initial six‐month step of the wedge was extended to 12 months.
Blinding
2.4
Participants and treating clinicians were unable to be blinded to the trial phase. All assessments were performed by clinically qualified, cultural‐security trained assessors blinded to the trial phase of the participant.
Participants
2.5
Aboriginal adults ≥ 18 years who presented within 6 weeks of an acute stroke or traumatic brain injury were eligible for the trial, provided they:
- Had a neurological deficit as determined by the National Institute of Health Stroke Scales (NIHSS) [18] (if they had a stroke) or
- Had a score of at least 8 on the Glasgow Coma Scale (GCS) [19] if diagnosed with TBI; and
- Were deemed able to benefit from rehabilitation by the medical or allied health team.
In the original protocol [10], the window of recruitment closed at 4 weeks post‐injury. This was increased to 6 weeks to enrol more patients who were initially very unwell but recovered sufficiently to be eligible for rehabilitation. All eligible patients from each site were invited to participate by clinical staff trained by the research team for this study. A hospital‐based Aboriginal Liaison Officer was involved where possible. Participants were enroled in the control or intervention group according to the study phase of their recruitment site. Enrolment of family members originally entailed wet‐ink signatures. Restrictions associated with COVID‐19 required an amendment to enable the option of verbal consent obtained over the telephone.
Baseline Characteristics
2.6
Baseline participant characteristics included recruitment region and demographics. Baseline clinical characteristics included injury type/severity, disability, anxiety, depression and functional independence [10].
Intervention
2.7
The intervention had two components. The first, cultural security training (CST), consisted of a three‐hour, face‐to‐face workshop and 3 h of online modules. These were developed by the research team members experienced in cultural training, with input from local Aboriginal Hospital Liaison teams in each of the regions where the training took place, and the Aboriginal Health Council of WA. The workshops were offered to health professionals (nursing, medical, allied health staff) every 6 months during the intervention period at each site; a minimum of 20 health professionals were trained at each site. Participants were envisaged as ‘champions’ and encouraged to model behaviours and attitudes to encourage other staff to follow the principles of the training. In addition, training was repeated so that new staff members had opportunities to attend over time.
The second component provided support of an Aboriginal Brain Injury Coordinator (ABIC) for participants in hospital and until 26 weeks post‐injury onset [20]. The ABIC role was developed by research team members in collaboration with participating Aboriginal Community Controlled Health Organisations and the Neurological Council of WA [20]. The role was designated for an Aboriginal health professional and included provision of education, support, liaison and advocacy services to participants and their families. The ABIC was required to be in face‐to‐face or telephone contact with the participant at least six times during the intervention period. ABICs were experienced health professionals and were local to the regions of participants, with training in working with people with ABI provided.
Follow‐Up
2.8
Participants were followed up prospectively and assessed at 12 and 26 weeks post‐injury either face to face or by telephone/telehealth as needed.
Outcomes
2.9
The primary outcome was quality of life, measured on the Euro QOL–5D‐3L VAS (EQ‐VAS) [21] at 26 weeks post‐injury. Secondary outcome measures were assessed at 12‐ and 26‐week post‐injury. Secondary participant‐level outcome measures included disability associated with brain injury as measured by the modified Rankin Scale—mRS [22] functional independence as measured on the Functional Independence Measure—FIM [23] and anxiety and depression, measured using the Hospital Anxiety and Depression Scale (HADS) [24] Participant satisfaction with their hospital experiences was also assessed via questionnaire at 12 and 26 weeks (see Appendix B). Caregiver strain was measured by the Modified Caregiver Strain Index [25] Outcome measures could be administered face‐to‐face or over the telephone. Serious adverse events (SAEs) were recorded throughout. System‐level outcomes at 12‐ and 26‐week post‐injury included percent of the minimum processes of care (MPC) achieved, number of allied health occasions of service and resource utilisation. MPC related to aspects of care received during inpatient admission, such as involvement of family, involvement of Aboriginal Liaison Officer, documentation of participant's first language, and use of interpreter if required [10] (see Appendix C for full list). Level of acceptability to hospital staff of the CST component of the intervention was obtained through custom‐designed questionnaires. As noted above, all assessments were undertaken by culturally trained assessors. We were unable to recruit Aboriginal assessors for these roles, reflecting the shortage of available Aboriginal health professionals.
Sample Size
2.10
The trial was designed to detect a between‐group difference of 15 points (standardised effect size of d = 0.6) on the EQ‐VAS. It was estimated that 312 participants (13 per cluster per time period) would be required to achieve 80% power at a significance level of 0.05. See the Statistical Analysis Plan for details [11].
Statistical Methods
2.11
Baseline characteristics were summarised using descriptive statistics. Age was summarised using median and inter‐quartile range, while other continuous variables were summarised using means and standard deviations; categorical variables were summarised using frequencies and percentages.
Outcome measures were treated as continuous, except for mRS, which was dichotomised as independent (0–2) or dependent/dead [3, 4, 5, 6]. Summary statistics were reported for the whole cohort and by trial phase (control/intervention).
The unadjusted outcomes were supplemented by results of linear mixed models, constituting the primary analysis. For the primary outcome measure (EQ‐VAS at 26 weeks), the model adjusted for age at recruitment, injury type, injury severity (dichotomised mRS at baseline), and time period as fixed effects, and recruitment site and participant as random effects. The models for the continuous secondary outcomes also adjusted for injury type, injury severity and time period as fixed effects, and recruitment site and participant as random effects. Since these outcomes were assessed at both 12‐ and 26‐week time points, the models also included time‐since‐injury as a fixed effect, together with the interaction of time‐since‐injury and trial phase (control/intervention). The interaction effect was used to estimate the adjusted 12‐ and 26‐week between‐group differences. A logistic generalised linear mixed model supplemented the results for the dichotomised mRS. Due to convergence issues, the confounders included in this model differed from those in the models for continuous outcomes, with time‐since‐trial‐commencement entered as a continuous variable.
The analyses of primary and secondary outcomes adjusted as above were conducted on an intention to treat (ITT) basis, where all participants were included in the phase (control/intervention) to which they were recruited, regardless of completion. These analyses are reported without imputation of missing data. ITT analyses with imputation of missing data were conducted separately, under the assumption that all missing data were missing at random (MAR). A sensitivity analysis was conducted to assess the MAR assumption (see Appendix D for details).
All analyses were conducted using the R Statistical Programming Language.
A concurrent process evaluation [26] was undertaken utilising the Consolidated Framework for Implementation Research [27] to explore contextual factors influencing specific trial processes, implementation of the intervention package and ultimate outcomes.
An economic evaluation to describe the potential cost‐effectiveness of the intervention is planned. This evaluation will be reported in a future publication.
Positionality Statement
2.12
Our multidisciplinary team included Aboriginal and non‐Aboriginal experts in the fields of brain injury, cardiovascular disease, cancer, dementia and health service planning. Four Aboriginal researchers were long‐term members of the research team, nine non‐Aboriginal researchers had lengthy experience collaborating on research with Aboriginal communities, and a further six were experienced in clinical trials. Further additional Aboriginal partners for example, Aboriginal Health Council of WA, Regional Aboriginal Health Consultants, hospital‐based Aboriginal liaison teams came on board to assist in the implementation to suit local contexts. The ABICs were central to the implementation, were interviewed for the process evaluation, co‐authored publications and led or participated in several state and national seminar, conference and media presentations.
Ethical Considerations
2.13
The Protocol for Healing Right Way was approved by Royal Perth Hospital (the central ethics committee for the study), St John of God Hospital, Edith Cowan University and the WA Aboriginal Health Research Ethics.
Role of Funding Source
2.14
The funders did not influence the study design, data collection, interpretation, or writing of the report in any way.
Results
3
Participant Flow
3.1
During the trial period, 382 Aboriginal Australians who presented with acute stroke or TBI were screened from February 2018 to July 2021. Of these, 241 (63%) were eligible for the trial and 108 (45%) were enroled; 47 (43.5%) in the control phase and 61 (56.5%) in the intervention phase (Figure 2).
Flowchart of progress through phases healing right way stepped wedge trial.
Recruitment
3.2
Recruitment was predominantly in the urban sites (n = 86; 79%), although 75% of participants resided in non‐metropolitan areas (Table 1). The median age of the cohort was 55 years. More males than females were recruited (59%), and stroke presentations predominated (n = 89; 82%). Half the participants were recruited before the onset of COVID‐19 and half after the onset. Reflecting the stepped‐wedge design, 84% of the intervention group (n = 51) were recruited after the onset of COVID‐19, as compared to 6% (n = 3) of the control group. While Aboriginal Liaison Officers in recruitment were aspired to, busy hospital Liaison teams and additional pressures due to COVID‐19 (including absences due to illness) made their involvement challenging, potentially impacting recruitment. Detailed discussion of recruitment is provided in the Process Evaluation paper [28].
The baseline characteristics of the treatment groups (control/intervention) were balanced except for a larger proportion of participants with TBI in the intervention (n = 16; 26%) than in the control phase (n = 3; 6%). Participants in the intervention phase reported more symptoms of depression at baseline (Median HADS‐D = 6.0) than in the control phase (Median HADS‐D = 4.5). Diabetes and ischaemic heart disease were more common co‐morbidities in the control than in the intervention group. Table 2 provides primary language information that reflects the diversity of participants and language groups involved in the study.
Follow‐Up
3.3
At the 12‐week assessment, 92 participants (85%) were available for clinical assessments—38 of control (81%) and 54 of intervention phase (88.5%) participants (see Table 3). At the 26‐week assessment, 34 (72%) control and 50 (82%) intervention participants were clinically assessed (see Table 4). Reasons for non‐availability included assessor challenges in contacting participants due to changing residences/contact numbers, illness, funerals, travel and reliance on busy relatives.
Outcomes
3.4
In the unadjusted analysis, the control group achieved a higher quality of life at 26 weeks post‐injury (mean EQoL‐VAS 70; SD = 21) than the intervention group (mean EQoL‐VAS = 61; SD = 18). This unadjusted difference was statistically significant (p = 0.046) and similar to EQoL‐VAS scores recorded 12 weeks post‐injury. However, after controlling for age at recruitment, injury type/severity and recruitment site (the primary analysis), the adjusted mean EQoL‐VAS was 62.5 for the control group and 60.8 for the intervention group. The mean difference of 1.7 was not statistically significant (p = 0.83).
Similarly, a lower proportion of control participants displayed injury‐related disability (51% dependent/dead) than the intervention group (68% dead/dependent) at 12 weeks (unadjusted). This trend increased to a statistically significant difference at 26 weeks (Control: 45% dependent/dead; Intervention: 74% dependent/dead; p = 0.005). These differences were mitigated by our pre‐specified adjusted analyses, which showed that the differences were not statistically significant at either time point.
Both groups showed improvement in functional independence at 12 and 26 weeks compared to baseline. The between‐group differences at these timepoints were not statistically significant at either time point. The adjusted analysis indicated that the control group reported significantly fewer symptoms of depression at 12 weeks than the intervention group. However, at 26 weeks, there was no significant difference between groups.
Service Level Outcomes
3.5
A higher proportion of MPCs was achieved in the intervention (unadjusted mean = 55%; SD = 16 at 12 weeks) than in the control group (unadjusted mean = 48%; SD = 20); the unadjusted difference in means was not statistically significant (p = 0.07). The unadjusted mean difference was sustained but still statistically non‐significant at 26 weeks (intervention: mean = 57%, SD = 17; control: mean = 51%; SD = 22; p = 0.09). After adjusting for age, injury type and severity, time period and site, there was a statistically significant between‐group difference of 7% in the percent of MPCs achieved (p = 0.048) at 12 weeks. The difference was similar at 26 weeks (6.8%, p = 0.038). Between‐group differences on occasions of service at 12 weeks or 26 weeks post‐injury were not significant.
Of participant respondents to the hospital experience survey (n = 81 at 12 weeks and n = 66 at 26 weeks; 54 at both time points), the vast majority (86%) from both intervention and control groups had positive experiences at both time points, although two participants in each group reported very bad experiences. Both groups reported similar satisfaction with their hospital experience at week 12, but intervention group experiences were significantly more positive than control group experiences by week 26 (p = 0.04).
There was a relatively large amount of missing data predominantly related to the Modified Caregiver Strain Index, the HADS and the economic evaluation information. A lack of family member recruitment, often due to the dislocation of the person from family initially, contributed to the missing carer data. Some economic details were too difficult for participants to recall, were considered intrusive, for example, regarding financial matters, or were omitted due to participant fatigue.
Fidelity
3.6
The Intervention Package was implemented broadly as planned. All 61 intervention group participants received the services of an ABIC, although only 59% received ≥ 6 ABIC contacts (Range = 1–19). The CST reached the target attendance numbers for the face‐to‐face component (250 staff trained), although only 50% of attendees completed the online modules thereafter. This coincided with pressures resulting from COVID‐19, technological issues, staff workload and the completion not being compulsory. Aboriginal facilitators were involved in all training, with additional Aboriginal hospital staff contributions in the workshops.
Feasibility and Acceptability
3.7
Implementation of the ABIC role was acceptable and feasible. Feasibility was inferred through the successful employment, training and retention of Aboriginal staff to each of the ABIC positions across the state. During times of change/absence of staff, the team worked as a network to ensure that participants in all regions obtained the ABIC services either face‐to‐face or by phone. The survey of the hospital experience, to which the assessor was blinded as to intervention status and therefore could not directly address the ABIC intervention, was one measure through which acceptability was inferred. Other measures included agreement to have ABIC follow‐up visits (all participants agreeing to these visits). In regard to the CST, detailed surveys with participants in the training were conducted and revealed overwhelmingly positive responses; feasibility was also determined by attendance at face‐to‐face workshops and participation of Aboriginal cultural experts (predominantly local to the region) as co‐facilitators at all sessions. Interviews with project staff and facilitators also provided critical analysis of feasibility and appropriateness of the CST approach.
Besides providing cultural training for 250 health staff, HRW contributed significant research/clinical capacity building for Aboriginal and non‐Aboriginal staff across WA. Nine Aboriginal staff were recruited and trained as ABICs; three Aboriginal health professionals as research assistants; 46 non‐Aboriginal staff as assessors and 21 as Research Site Contacts (primary contact at the hospital recruiting site).
Adverse Events
3.8
During the trial, 51 serious adverse events were recorded. The proportion of participants who experienced at least one serious adverse event was significantly higher in the control group (n = 17; 36%) than in the intervention group (n = 9; 15%) (χ ^2^ = 6.66; p < 0.01). See Appendix E for further detail.
Discussion
4
Healing Right Way was the first brain injury related RCT within Aboriginal populations and the first to document 26‐week follow‐up of Aboriginal patients, including functional outcomes and quality of life. It was conducted in a complex, real‐world health service context, spanning metropolitan and rural areas, multiple health service providers and study partners, and a culturally diverse population. The RCT showed no significant quality of life or clinical differences between control and intervention groups, although MPC were significantly more adhered to in the intervention phases and participant‐reported hospital experiences were more positive in the intervention group. These results are suggestive only, as target numbers required to power the study to generate definitive results were not reached. Nevertheless, the findings provide important documentation and analysis of processes and experiences of care for Aboriginal people after brain injury, which is rarely recorded or focused upon to date.
The COVID‐19 pandemic starting midway into the recruitment period significantly affected all aspects of the study. As alluded to above, the involvement of Aboriginal Liaison Officers in the recruitment process was challenging, potentially affecting recruitment. Besides affecting recruitment, the pandemic was in progress for most of the intervention period, potentially negatively affecting the quality of life and clinical outcome measures in intervention compared with control periods. The infrastructural, logistical, community and health system impacts of the pandemic may have adversely affected the ability to receive family support and the ability to access health and rehabilitation services during this period [29]. The possibility that not everyone may want or need the kind of assistance offered by the ABICs must be considered in terms of the results; further qualitative feedback from participants using yarning methodology for assessing outcomes (as discussed in the Limitations section below) could have enhanced our understanding of this component of the intervention.
The fact that most participants were recruited in the metropolitan area but resided in regional, rural, or remote areas is consistent with previous studies [1, 2, 3] and reflects the need to focus on rehabilitation services in rural areas and to better address the transition of patients back to these areas after acute treatment in the metropolitan area. While the relatively young age of participants who had suffered a stroke and the high incidence of comorbidities were commensurate with other studies, it highlights the relatively complex recovery journeys that many Aboriginal people must navigate. These issues need consideration if relevant, accessible and flexible rehabilitation services are to be offered.
The follow‐up rate of participants was relatively high, given distances involved and oft‐cited anecdotal clinical reports of difficulty in follow‐up. Integral to the follow‐up in HRW was the use of existing and the establishment of new networks with Aboriginal health service providers and within Aboriginal communities across the state, that assisted the research team in locating and connecting with participants. Networks included hospital Aboriginal Liaison Officers, community services, Aboriginal Medical Services and other family members, where available. Strong relationships facilitated all study processes.
The finding of higher compliance with MPC in the intervention group suggests that CST and the presence of ABICs in hospitals can make a difference to the delivery of care. While simply running the trial may have heightened hospital staff's attention to care delivery to Aboriginal patients, the important role of training was supported by the positive response of staff to the cultural training provided and recommendations for more regular training.
The importance of a concurrent process evaluation cannot be underestimated, with ongoing feedback on trial processes informing practical modifications, while also providing implications for service delivery and future research methods. Translation and knowledge exchange occurred throughout the study, with ongoing meetings with, and presentations to clinical partners, policy advocates, community and Aboriginal people with brain injury and regular media engagement. Details are provided elsewhere [30].
In terms of generalisability of study processes and results, the presence of the pandemic during the study presented a unique set of circumstances. Nevertheless, findings related to the geographical and cultural context of the trial and many of the challenges encountered are relevant to and generalisable in the planning of future rehabilitation services. The systems used within the study to address the challenges faced are highly relevant to the provision of services across geographically large distances and in a context where patients are often flown from rural and remote areas to metropolitan areas for acute care. Findings regarding the importance of the ABIC in a ‘navigator’ role, methods for conducting rehabilitation assessments online rather than face to face, and networking methods used in HRW for follow‐up purposes should be highly generalisable.
Limitations
4.1
Diminished recruitment and sample size reduced the power of the study and the ability to detect an intervention effect, with no definite conclusions possible. The secondary outcomes are not adjusted for multiple comparisons, and any statistically significant results should be interpreted with caution. Low recruitment of TBI participants reflects challenges in reaching this group in the acute stage and limits conclusions about them. Besides COVID, the WA legislative changes surrounding consent had a significant impact on recruitment. Limited involvement of Aboriginal people in recruitment (logistical issues), poor systems for identification of Aboriginal patients in hospitals, and competing commitments of many hospital staff all influenced recruitment (all explored in the process evaluation companion paper) [28].
The stepped wedge design has inherent limitations in that changes occurring over time external to the trial itself may differentially influence outcomes between control and intervention periods. Although not all participants received the minimum number of ABIC visits, flexibility to varying needs and personalised care was needed. Multiple assessment tools, often inducing fatigue and reflecting the need for standardised, widely used assessments in RCTs, some tools were not culturally appropriate. Both contributed to missing outcome data and that the assessors collecting the outcome data were non‐Aboriginal could also have influenced results. Further qualitative feedback on the ABIC service (beyond the limited general survey) to assess participants' specific satisfaction with and perceptions of benefit from the intervention would have been useful. Future intervention studies could utilise a yarning framework in addition to culturally appropriate tools to capture quantitative outcome measures. The COVID‐19 context influenced availability of staff to attend the face‐to‐face cultural training and complete the online modules, both non‐compulsory. While the cultural training was positively received and the target numbers were reached, the numbers may have been too low for training to have affected participants' journeys and outcomes, particularly in large metropolitan hospitals where numbers and staff turnover are high.
Conclusion
5
The study was unable to definitively address the effect of this intervention on quality of life. The difference between control and intervention periods in compliance with MPC suggests that system‐level change is possible, with individual‐level change perhaps more challenging to determine. Despite challenges, HRW demonstrated that the intervention package was feasible and acceptable, and that a complex trial across multiple metropolitan and rural sites is possible in an Aboriginal health context. It has highlighted the importance of Aboriginal leadership, partnerships across sites, and community networks in following patients post‐discharge to enable the provision of comprehensive and culturally secure services.
Author Contributions
Elizabeth Armstrong: conceptualization; formal analysis; funding acquisition; investigation; methodology; supervision; writing – original draft preparation; writing – review and editing. Tapan Rai: conceptualization; formal analysis; funding acquisition; methodology; writing – original draft preparation; writing – review and editing. Judith Katzenellenbogen: conceptualization; funding acquisition; methodology; writing – review and editing. Sandra Thompson: conceptualization; funding acquisition; methodology; writing – review and editing. Meaghan McAllister: project administration; methodology; resources; writing – review and editing. Natalie Ciccone: conceptualization; funding acquisition; methodology; writing – review and editing. Deborah Hersh: conceptualization; funding acquisition; methodology; writing – review and editing. Leon Flicker: conceptualization; funding acquisition; methodology; writing – review and editing. Dominique Cadilhac: conceptualization; funding acquisition; methodology; writing – review and editing. Erin Godecke: conceptualization; funding acquisition; methodology; writing – review and editing. Graeme Hankey: conceptualization; funding acquisition; methodology; writing – review and editing. Neil Drew: conceptualization; funding acquisition; methodology; writing – review and editing. Colleen Hayward: conceptualization; funding acquisition; methodology; writing – review and editing. Deborah Woods: conceptualization; funding acquisition; methodology; writing – review and editing. Mel Robinson: methodology; writing – review and editing. Ivan Lin: conceptualization; funding acquisition; methodology; writing – review and editing. Sanita Kratina: data curation; methodology; resources; software; writing – review and editing. Jane White: data curation; methodology; software; writing – review and editing. Juli Coffin: conceptualization; funding acquisition; methodology; writing – review and editing.
Disclosure
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. H. Balabanski , K. Goldsmith , B. Giarola , et al., “Stroke Incidence and Subtypes in Aboriginal People in Remote Australia: A Healthcare Network Population‐Based Study,” BMJ Open 10, no. 10 (2020): e 039533.10.1136/bmjopen-2020-039533 PMC 754563333033097 · doi ↗ · pubmed ↗
- 2J. M. Katzenellenbogen , E. R. Atkins , S. C. Thompson , et al., “Missing Voices: Profile and Extent of Acquired Communication Disorders in Aboriginal and Non‐Aboriginal Adult Stroke Survivors in Western Australia Using Linked Administrative Records,” International Journal of Stroke 11, no. 1 (2016): 103–116.26763026 10.1177/1747493015607521 · doi ↗ · pubmed ↗
- 3J. M. Katzenellenbogen , E. Atkins , S. C. Thompson , et al., “Missing Voices: Profile, Extent, and 12‐Month Outcomes of Nonfatal Traumatic Brain Injury in Aboriginal and Non‐Aboriginal Adults in Western Australia Using Linked Administrative Records,” Journal of Head Trauma Rehabilitation 33, no. 6 (2018): 412–423.29601340 10.1097/HTR.0000000000000371 · doi ↗ · pubmed ↗
- 4E. Armstrong , J. Coffin , D. Hersh , et al., “‘You Felt Like a Prisoner in Your Own Self, Trapped’: The Experiences of Aboriginal People With Acquired Communication Disorders,” Disability and Rehabilitation 43, no. 13 (2021): 1903–1916.31692386 10.1080/09638288.2019.1686073 · doi ↗ · pubmed ↗
- 5E. Armstrong , J. Coffin , M. Mc Allister , et al., “‘I've Got to Row the Boat on My Own, More or Less’: Aboriginal Australian Experiences of Traumatic Brain Injury,” Brain Impairment 20 (2019): 120–136.
- 6I. Bohanna , M. S. Fitts , K. Bird , et al., “The Transition From Hospital to Home: Protocol for a Longitudinal Study of Australian Aboriginal and Torres Strait Islander Traumatic Brain Injury (TBI),” Brain Impairment 19, no. 3 (2018): 246–257.
- 7A. H. Balabanski , L. Nedkoff , A. Brown , et al., “Incidence of Stroke in the Aboriginal and Non‐Aboriginal Populations of Australia: A Data Linkage Study,” Stroke 54 (2023): 2050–2058.37325922 10.1161/STROKEAHA.122.041975 · doi ↗ · pubmed ↗
- 8A. Esterman , F. Thompson , M. Fitts , et al., “Incidence of Emergency Department Presentations for Traumatic Brain Injury in Indigenous and Non‐Indigenous Residents Aged 15–64 Over the 9‐Year Period 2007–2015 in North Queensland, Australia,” Injury Epidemiology 5, no. 1 (2018): 40.30417259 10.1186/s 40621-018-0172-9PMC 6230543 · doi ↗ · pubmed ↗