A rare complication of the hydatid cyst of the liver: A case report of Cysto-cutaneous fistula
Dorsaf Mouelhi, Ben lahouel Senda, Laila Jedidi, Mabrouk Aymen, Saidani Aya

TL;DR
This paper reports a rare case of a liver hydatid cyst forming a skin fistula in a 47-year-old woman, emphasizing the importance of early diagnosis and surgical treatment in endemic regions.
Contribution
The paper presents a rare clinical case of cysto-cutaneous fistula due to a hepatic hydatid cyst and highlights diagnostic and management challenges.
Findings
Cutaneous fistulization of a hepatic hydatid cyst is a rare complication often misdiagnosed as an abscess.
Complete surgical excision of the cyst and fistulous tract is essential for effective treatment.
Imaging, particularly CT scans, is crucial for diagnosis and surgical planning in such cases.
Abstract
Hepatic Hydatid cyst of the liver is a parasitic zoonotic illness caused by Echinococcus granulosus that remains endemic in regions where sheep farming is common, particularly in our country, Tunisia. While it is a benign disease, its natural evolution can be marked by life-threatening complications. Cysto-biliary communication is the most common and serious complication. Spontaneous cutaneous fistulization is an extremely rare complication. We report the case of a 47-year-old female who presented with a chronic discharging sinus in the left upper quadrant of the abdomen. Clinical examination revealed a cutaneous opening with clear fluid discharge and surrounding inflammation. Abdominal imaging identified two hepatic hydatid cysts: one located in the left lobe, which was fistulized to the skin, and another in the right lobe. Surgical exploration confirmed the fistulous tract between…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
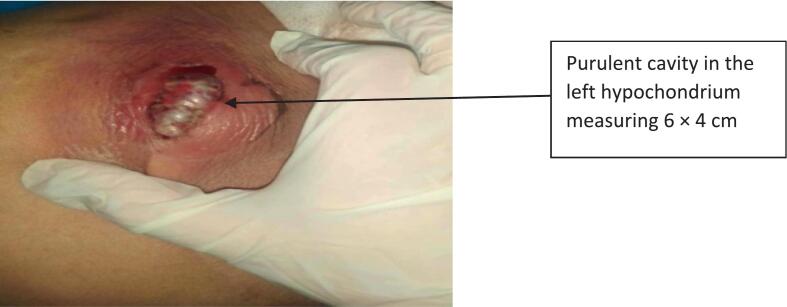 Figure 1
Figure 1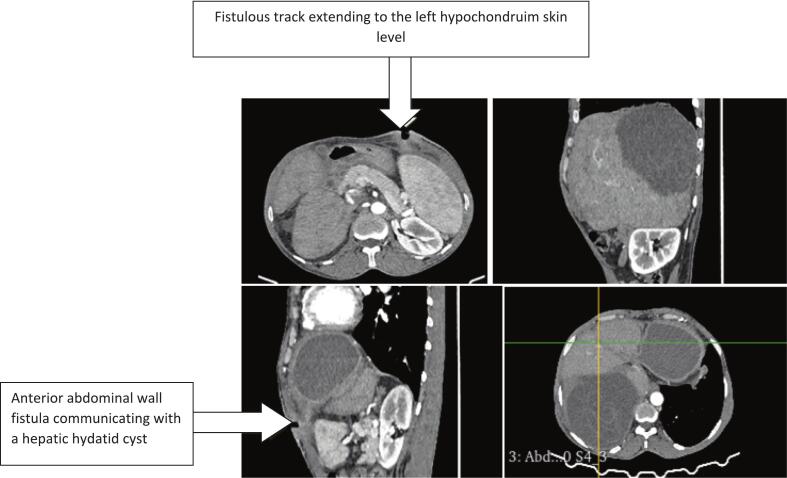 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Congenital Anomalies and Fetal Surgery · Urological Disorders and Treatments
The case report is reported in line with the SCARE criteria [1].
Introduction
1
Hydatid disease (HD) is caused by a parasite called Echinococcus granulosus. It is found in many parts of the world where sheep farming is common. These regions include the Mediterranean, the Middle East, South America, Central Asia, and sub-Saharan Africa. In North Africa, including Tunisia, the number of cases remains high, with reports ranging from 15 to 30 cases per 100,000 people each year. The liver is the most frequently affected organ [2]. While generally harmless, there is a risk of complications arising from various issues, particularly when it occurs in the bile duct [2]. A rare form of HD is when the disease affects the tissue under the skin, which then leads to the formation of skin fistulas. This phenomenon has only been observed in a limited number of cases, ranging from 0.1 % to 1.5 % [3]. In this paper, we present a rare case of a cysto-cutaneous fistula in a 47-year-old female patient treated in our department. This revealed a hydatid cyst in the left liver that had ruptured into the abdominal wall.
Case report
2
A 47-year-old female patient with no medical history underwent surgery for a hydatid cyst of the liver using a right subcostal incision fifteen years ago. She currently resides in a sheep-farming area and presented to our emergency department with upper right quadrant and epigastric pain, accompanied by vomiting, fever, and a cutaneous lesion with purulent discharge that appeared a week ago in the left hypochondrium (Fig. 1). During the physical examination, the patient was conscious but appeared generally unwell. She had a fever of 39 °C, but no signs of jaundice. The cardiovascular examination revealed no signs of tachycardia, with normal blood pressure (120/75 mmHg). The respiratory rate was found to be within normal parameters. A thorough abdominal examination revealed tenderness in the right hypochondrium. A tender mass was palpable in the left hypochondrium, and the examination of the lesion in the upper left quadrant revealed a fistula with purulent discharge. The rest of the examination revealed no further issues. Laboratory tests revealed an inflammatory biological syndrome characterized by elevated white blood cell counts (19,000 UI/ml) and C-reactive protein levels (153 mg/l), while liver function tests were found to be within normal parameters. An abdominal computed tomography (CT) scan revealed a 13-cm hydatid cyst in segments VII and VIII of the liver, along with a second, 7-cm multivesicular hydatid cyst in the left liver. The latter exhibited exophytic growth and had fistulized to the skin, accompanied by a heterogeneous subcutaneous fluid collection (Fig. 2). Due to limited access to advanced imaging modalities in our setting, as well as the absence of clinical or biological signs suggestive of cysto-biliary fistula, magnetic resonance cholangiopancreatography (MRCP) was not performed preoperatively. The diagnosis had already been established based on ultrasound and CT findings, which were considered sufficient for surgical planning. The hydatidosis serology was positive.Fig. 1. Subcutaneous abscess cavity.Fig. 1. Fig. 2CT scan: subcutaneous rupture of a hydatid cyst of the left liver.Fig. 2
The patient was diagnosed with a liver hydatid cyst complicated by fistulization to the abdominal wall and a subcutaneous abscess. The patient received a 12 mg/kg/day dosage of albendazole for 15 days in conjunction with antibiotic treatment. Then we decided to operate on the patient. She was placed in the supine position with a slight reverse Trendelenburg tilt, the left and right sides elevated to allow optimal exposure of the left liver lobe. She then underwent surgery via a bi-subcostal incision. Two large hydatid cysts were found in the liver. The largest cyst, measuring 12 cm, was located in segments VII and VIII. The second cyst, located in the left lobe of the liver, exhibited a fistulous tract extending to the skin surface. Intraoperative indocyanine green (ICG) fluorescent imaging was not used, as this technology is not available in our center. The procedure involved an open cyst evacuation, followed by a partial pericystectomy of both cysts.
A cholecystectomy was performed by the surgical team for an intraoperative cholangiogram, and a trancystic drain was used. The results revealed no dilation of the common bile duct and no evidence of a cysto-biliary fistula. The residual cystic cavity was then cleared of its contents and irrigated with hypertonic (20 %) saline as a scolicidal agent. The fistulous tract was excised en bloc, and the cavity was externally drained. Three drains were placed in the hepatic and subcutaneous residual cavities. A postoperative cholangiogram on the fifth day showed no signs of bile leakage. The patient was discharged on the seventh day after the removal of the intra-cavitary drainage. Following the operation, she was prescribed a dosage of 10 mg/kg/d of Albendazole for six months. Postoperative events were assessed using the Clavien-Dindo classification system. In this case, the patient had an uneventful recovery, which corresponds to a Grade I complication. The procedure was performed by a surgeon with extensive experience in managing cases of hepatic hydatid disease in endemic regions, specifically in Jendouba, a city in the northwestern part of Tunisia. The patient expressed confidence in the surgical team and was pleased with the smooth postoperative recovery. She reported a high level of satisfaction with the care received and expressed gratitude for the successful outcome and resolution of her symptoms. Following a review at the six-month mark, the clinical evolution was found to be favorable. A follow-up abdominal CT scan performed at six months showed no residual or recurrent hepatic cysts or collections. Hydatid serology was repeated at six months and showed a significant decline in antibody titers, suggesting a good treatment response (Table 1).Table 1. Clinical presentation.Table 1. EventDetailsPatient47-year-old femaleSurgery historyPrevious hepatic hydatid cyst surgery 15 years earlierClinical presentationPainful swelling with purulent cutaneous discharge in the left hypochondriumImagingCT scan: two hepatic hydatid cysts; left-sided cyst fistulized to the skinTreatmentInitial medical therapy, followed by: resection of cyst dome, fistula disconnection, and excision of fistulous tractPostoperative courseUneventful recovery; no complications or recurrence at 6-month follow-up
Discussion
3
Hydatid disease is a globally prevalent zoonotic infection caused by the larval form of the Echinococcus parasite. This issue continues to represent a notable public health concern in regions where the disease is endemic, with Tunisia being a prime example. While hydatid cysts can develop in any organ, the liver is by far the most frequently affected site. In most cases, hepatic hydatid cysts do not cause any symptoms; however, complications may result in the emergence of clinical symptoms. These may include secondary infection, anaphylactic reactions, compression of nearby structures, or rupture into the peritoneal cavity or biliary system. It should be noted that the most frequent complication is cyst rupture into the biliary tract [4]. In contrast, the extension of hepatic hydatid cysts into subcutaneous tissue with subsequent skin fistulization is extremely rare, occurring in only 0.1 % to 1.5 % of cases [3]. Following a thorough review of the literature on cutaneous involvement in hydatid disease (Table 2), we found 12 publications from 2015 to 2025. This type of complication is usually linked to cysts that are located in the front part of the body and exhibit exophytic growth patterns [5].Table 2. Details of cases from review of literature for cutaneous fistulization of hydatid cyst of the liver.Table 2. ReferenceYearCountrySexAgeCyst size (mm)Cyst locationsFistula opening/lesion locationTreatmentAlgutaini & Al-Wageeh2025YemenMale6Not specifiedLiver, abdominal wallEpigastric regionAlbendazole + surgical cystectomyRamraoui [9]2024MarocNot stated6887 × 69Right liver lobeRight hypochodruimSurgery + albendazoleMili [16]2023TunisiaMale1050Left liver lobeLeft hypochondriumAlbendazole + laparoscopic pericystectomy + tract drainageRamazan Orkun Önder [17]2022TurkeyFemale85Not statedSegments VI and VII of the liverNot statedA drainage catheter+medical treatmentSaif Ghabisha [10]2021IranFemale63Not statedHepatic (unspecified lobe)Abdominal wallLaparotomy + partial cystectomy + tract excisionB. Khan [7]2020United Arab EmiratesMale57120 × 150 abscess massMultiple hepatic lobesRight upper quadrant abdominal wallIncision & drainage + albendazoleCicero [12]2017ItalyMale68CE5 calcified cystSegment VI, right lobeRight flank/subcutaneous abscessPercutaneous drainage + surgical cystectomy + medical treatmentEl Khoury [18]2017LebanonFemale6855 × 80 × 56Segments V–VIII, right hepatic lobeRight breastAlbendazole + omentoplasty + cyst & tract drainageVirgilio [19]2015ItalyFemale55100Right lobe liverRight hypochodruimNon operative managementMandolkar [20]2015IndiaFemale25110 × 100Left lobe of liverLeft hypochondriumPericystectomy + fistula excision + albendazoleDaldoul [14]2015TunisiaFemale2350Right lobe of liverRight flankPericystectomy + fistula excisionAkay [21]2015TurkeyMale80100Right liver lobeRight hypochodruimDrainage
This rare complication results from a combination of two main factors: mechanical and inflammatory processes [3]. Infection of the cyst contents can trigger inflammation of the pericyst, promoting its adherence and eventual fusion with the abdominal wall. Conversely, the thick and sometimes calcified pericyst gradually erodes the abdominal wall, a process that is further facilitated by repetitive respiratory movements.
Hydatid disease progresses through several stages before leading to an external rupture through the abdominal wall. In Stage I, the lesion extends to the innermost muscle layers. Stage II involves penetration beyond the muscular layer into the subcutaneous tissues. Stage III is characterized by the cyst reaching the subcutaneous layer and forming a cutaneous fistula [6].
Although uncommon, cutaneous fistulization is a serious complication of hydatid disease. A diagnosis can be challenging in cases where there is no visible discharge of cystic fluid or daughter vesicles from the fistula's external opening, particularly in regions where hydatid disease is endemic [7]. Clinical suspicion remains the cornerstone for early diagnosis and management. Key diagnostic indicators include residency in an endemic area and a known history of hydatid disease. From a clinical perspective, patients frequently present with a painful, febrile mass in the right hypochondrium. The presence of hydatid fluid or daughter cysts emerging from the fistulous tract is a valuable diagnostic sign [8,9]. A combination of clinical examination, imaging, and serological testing greatly aids in confirming the diagnosis [10]. Furthermore, histopathological analysis of any discharge from the fistula can confirm the parasitic origin and detect secondary infection, if present [6]. Abdominal computed tomography (CT) is a detailed diagnostic tool that can provide valuable insights into the nature of hydatid cysts and their associated fistulas. It is one of the most commonly used imaging methods for identifying cutaneous involvement and locating lesions responsible for complications associated with hydatid disease [11]. CT scans are particularly valuable in patients with a history of hydatid cyst surgery, as they help distinguish between a recurrent hepatic cyst causing a cysto-cutaneous fistula (as in the case we report) and a parietal inoculation of the abdominal wall during prior surgical intervention.
Positive hydatid serology is a valuable complementary tool to imaging, particularly in cases where the diagnosis remains uncertain. Of the available diagnostic techniques, contrast-enhanced fistulography is particularly useful in evaluating cutaneous complications of hydatid disease. It provides precise information regarding the extent of the fistulous tract, the location and size of the involved lesion, and its anatomical relationship with the biliary tree [6].
It is essential that the presence of a cysto-biliary fistula is identified before the procedure, and this should be done using magnetic resonance cholangiography as a standard procedure [12]. When necessary, intra-operative cholangiography can be used as a complementary method to further delineate the biliary anatomy and confirm the presence of a fistulous connection [13].
Cutaneous fistulization is generally not sufficient to achieve complete healing, as it only permits partial drainage of the abscess and the hydatid cyst [14]. Therefore, surgical intervention remains necessary to ensure the complete elimination of all parasitic fragments. A 4-week course of Albendazole should be taken before surgery. The combination of surgical and anti-parasitic treatment has shown favorable outcomes in patients suitable for operative management [14,15]. The surgical approach typically involves cysto-parietal disconnection and the removal of any secondary abscess, followed by definitive treatment of the hydatid cyst, management of the residual cavity, and excision of the fistula tract. Albendazole therapy is strongly recommended to reduce the risk of recurrence [13].
In cases of chronic cutaneous discharge in the right or left upper quadrant, particularly in endemic areas, several differential diagnoses should be considered. These include pyogenic liver abscesses with spontaneous cutaneous drainage, tuberculous liver abscesses, infected hematomas, necrotic liver tumors, particularly when imaging is nonspecific or serology is inconclusive, thus delaying appropriate management. In high-risk cases of cutaneous fistulization due to hydatid disease, especially in endemic regions and among patients with a history of hepatic hydatid disease, early diagnosis and prevention of potentially dangerous interventions such as blind drainage or incomplete cyst excision are essential.
Conclusion
4
Hydatid disease is a parasitic infection caused by the parasite Echinococcus granulosus. While it is generally considered to be a harmless condition, it can potentially lead to more severe outcomes due to associated complications. Spontaneous cysto-cutaneous fistulization of the hydatid cyst is an exceptional complication of hydatid disease. Imaging plays a key role in facilitating positive diagnoses and effective postoperative monitoring. Surgical treatment involving the excision of the cyst and fistula tract, in combination with medical intervention, has proven to be an effective approach for the management of hydatid cysts that result in cutaneous fistulas.
CRediT authorship contribution statement
- Mouelhi Dorsaf: Data collection, manuscript writing.
- Laila Jedidi; Senda ben Lahouel and Aymen Mabrouk: Critical supervision, revising manuscript.
- Aya Saidani: Resources, visualization, redaction.
All authors agreed to the final manuscript.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval is exempt/waived at our institution.
Guarantor
Mouelhi Dorsaf.
Research registration number
Not applicable.
Provenance and peer review
Not commissioned, externally peer reviewed.
Funding
The study was not supported by any sponsor or funder.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kerwan A.Al-Jabir A.Mathew G.Sohrabi C.Rashid R.Revised Surgical C Ase R Eport (SCARE) guideline: an update for the age of Artificial Intelligence Prem. J. Sci.2025 Disponible sur:https://premierscience.com/pjs-25-932/(Internet, cité 13 août 2025)
- 2Dziri C.Haouet K.Fingerhut A.Zaouche A.Management of cystic echinococcosis complications and dissemination: where is the evidence?World J. Surg.336juin 2009126612731935032110.1007/s 00268-009-9982-9 · doi ↗ · pubmed ↗
- 3Selmi M.Kharrat M.M.Larbi N.Mosbah M.Ben Salah K.Kyste hydatique du foie fistulisé à la peau et ouvert dans les voies bilaires et les bronches Ann. Chir.1266 juill 20015955971148655110.1016/s 0003-3944(01)00559-4 · doi ↗ · pubmed ↗
- 4Kayaalp C.Bostanci B.Yol S.Akoglu M.Distribution of hydatid cysts into the liver with reference to cystobiliary communications and cavity-related complications Am. J. Surg.1852 févr 20031751791255945210.1016/s 0002-9610(02)01202-3 · doi ↗ · pubmed ↗
- 5Bouassida M.Sassi S.Mighri M.M.Laajili A.Chebbi F.Chtourou M.F.Les complications pariétales du kyste hydatique du foie. À propos de deux cas en Tunisie Bull. Soc. Pathol. Exot.1054 oct 20122592612308649510.1007/s 13149-012-0224-2 · doi ↗ · pubmed ↗
- 6Bahce Z.S.Akbulut S.Aday U.Demircan F.Senol A.Cutaneous fistulization of the hydatid disease: a PRISMA-compliant systematic review Medicine (Baltimore)9538 sept 2016 e 488910.1097/MD.0000000000004889 PMC 504490127661031 · doi ↗ · pubmed ↗
- 7B. Khan M.A.Abusharia M.I.Mousa H.M.Abu-Zidan F.M.Hepatic hydatid cyst presenting as a cutaneous fistula Turk. J. Emerg. Med.203juill 20201461483283273410.4103/2452-2473.290071 PMC 7416854 · doi ↗ · pubmed ↗
- 8Akbulut S.Parietal complication of the hydatid disease: comprehensive literature review Medicine (Baltimore)9721 mai 2018 e 1067110.1097/MD.0000000000010671 PMC 639298829794743 · doi ↗ · pubmed ↗