Cardiovascular disease and absenteeism in Dutch occupational health: a retrospective study in a regular working population
Ivo M van Dongen, Jobst Winter, Bart Aben, Gilbert W M Wijntjens, Ronak Delewi, Jan Siebers, Robin N Kok, Frederieke G Schaafsma

TL;DR
This study shows that cardiovascular disease is a major cause of long-term absenteeism and high costs for employers in the Netherlands.
Contribution
The study provides new empirical data on the impact of CVD on absenteeism and costs in a working population.
Findings
CVD is the primary cause of absenteeism in 3.2% of all cases.
The median absenteeism duration due to CVD is 119 working days.
The estimated cost to employers is €37,000 per employee affected by CVD.
Abstract
There is very limited data available on the impact of cardiovascular disease (CVD) on absenteeism occurrence, absenteeism duration, and the associated rough cost-estimate for employers. We extracted routinely collected absenteeism data for the years 2019–2022 from a database maintained by two large, nationally operating occupational health services (n = 443,740). All diagnoses and included sickness cases were recorded > 6 weeks of absenteeism. Descriptive statistics, including median values (IQR) and percentages, were calculated and compared using the Mann-Whitney U test and Pearson chi-square test. Subgroup comparisons were performed using the Kruskal-Wallis test. To analyse return-to-work over time, a Kaplan-Meier curve was constructed, and differences in return-to-work were assessed using the Log Rank (Mantel-Cox) test. CVD is the primary cause of absenteeism in 3.2% of all…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
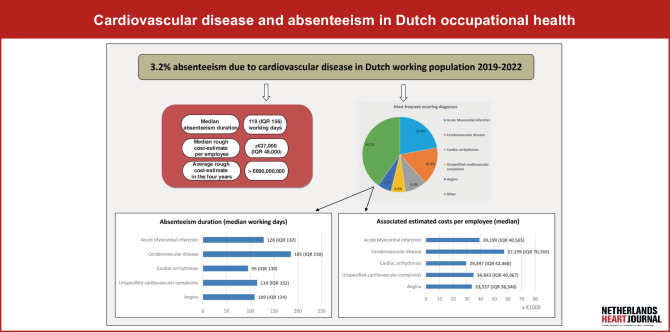 Figure 1
Figure 1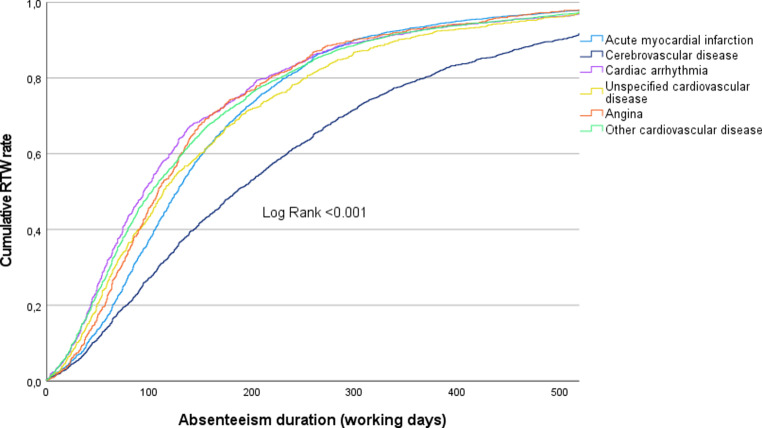 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsWorkplace Health and Well-being · Employment and Welfare Studies · Healthcare cost, quality, practices
Introduction
The impact of cardiovascular disease (CVD) on employment capabilities and its associated costs for businesses and society has been poorly investigated. CVD is the foremost cause of mortality globally, and it’s associated with high morbidity [1]. Among all types of CVD, ischemic heart disease (IHD), cerebrovascular disease, and peripheral arterial disease (PAD) are the most prevalent.
There is a lack of current data on the precise incidence of CVD-related absenteeism and the additional costs incurred by companies or society due to absenteeism caused by CVD. Previous research has shown that CVD significantly contributes to increased workplace absenteeism [2–7]. Currently, the only available data are on IHD specifically. In 2002, the average absenteeism duration after IHD was 189 days in the Netherlands, and globally the average absenteeism duration after myocardial infarction varied from 38 days to 177 days [8]. In a Swedish publication, covering the years 2006–2008, the adjusted mean absenteeism days were 83.9 (95% CI 80.6–86.5) during the first year after an IHD event, and after stroke these were 179.5 (95% CI 172.4–186.8) days [5]. The occurrence of IHD led to a six-fold increase in absenteeism days, and the occurrence of stroke led to a 14-fold increase compared to the absenteeism days prior to the event [5].
Therefore, following an acute cardiac event, return-to-work (RTW) represents a vital patient-reported outcome (PROM) of interdisciplinary disease management [4]. Cardiac rehabilitation (CR) supports patients in recovering and RTW after acute coronary events, particularly through a multidisciplinary approach that includes medical, physical, psychosocial, and vocational support [9]. Despite this, many working-age patients do not successfully reintegrate into employment after CR, leading to reduced quality of life and societal costs [9]. Importantly, studies also show that RTW is more influenced by other PROMs—such as expectations, anxiety, and quality of life—than by clinical measures. Other factors, such as comorbidities, low education, and negative beliefs, hinder RTW while endurance training, higher education, and perceived work stress can facilitate RTW [9, 10]. With an aging workforce and rising retirement age, the burden of CVD on society is expected to grow, making effective vocational reintegration increasingly important (Fig. 1).
Standard of care in absenteeism in the Netherlands
In the Netherlands, employees must report sickness to their employer when they are unable to work. If the absence is prolonged or expected to last more than a few weeks, the employee must consult an occupational health professional within the first 6 weeks. Employers are legally required to have a contract with such professionals to ensure access to occupational health services [11]. These professionals assess the cause of absenteeism, monitor recovery, and support RTW [11]. Employers must pay at least 70% of wages during the first two years of sick leave and may incur additional costs for absenteeism management and workplace adjustments. Wolvetang et al. have described the key legislation and procedures related to sick leave [11]; further background information on standard care in absenteeism is available as Electronic Supplementary Material (ESM).
Study objectives
The present exploratory study aims to investigate the incidence of CVD-related absenteeism, the duration of absenteeism, and the associated costs for employers. Additionally, the study will identify the most frequently occurring CVD diagnoses to determine which specific CVD patients could benefit from more work-focused in-hospital and outpatient treatment.
Methods
We extracted routinely collected absenteeism data from 2019–2022 from a database maintained by two large, nationally operating Dutch Occupational Health Services (OHSs; both are part of HumanTotalCare BV).
The Medical Research Ethics Committee of the Amsterdam UMC stated that the Dutch Medical Research Involving Human Subjects Act did not apply (reference number: 2024.0446).
Study population
In the Netherlands, occupational health physicians (OHPs) record cardiac symptoms and diseases using the Dutch ‘Classification for Occupational and Social Insurances (CAS)’, based on ICD-10 [12]. This study included employees aged 16 or older who were reported sick due to a cardiovascular CAS code (C-class) between 2019 and 2022 [12]. Only cases with sick leave lasting at least 6 weeks (up to a maximum of 2 years, as per Dutch law) were included.
Variables
Absenteeism duration, or time until RTW, was defined as the number of calendar days between the first day of sick leave and full return to work. Working days were calculated by multiplying total days by 5/7. To estimate employer costs, we used the friction method and hourly cost rates from Statistics Netherlands (CBS), which include wages, training, and social security contributions [11, 13–15]. In 2020, the cost per working day was € 38.11 × 8 h; in 2022 this was € 39.88 × 8 h [13–15]. We applied the 2020 rate to 2019–2021 and the 2022 rate to 2022. As data on overhead, exact wages, part-time work, or partial recovery were unavailable, cost estimates likely underestimate the true employer costs. All other variables were routinely collected during occupational healthcare and extracted anonymously from occupational healthcare medical records.
Further methodological details are provided in the ESM.
Data analysis
Descriptive statistics were reported as mean (SD), median (IQR), or percentages. For group comparisons, we used the Mann-Whitney U test or Pearson chi-square test; subgroup differences were analysed with the Kruskal-Wallis test. Kaplan-Meier curves illustrated RTW over time for the five most common causes of absenteeism, with differences tested via the Log Rank (Mantel-Cox) test. Employees lost to follow-up—due to contract termination, retirement, or resignation—were censored and considered sick until that point. All p-values were two-sided, with significance set at p < 0.05. Analyses were performed using IBM SPSS Statistics version 28.0.1.1.
Results
Participants and disease occurrence
During the period 2019 to 2022, a total of 443,740 absenteeism cases were registered in the database. This database represents approximately 28% of the total population of employees on sick leave in the Netherlands during this timeframe [16]. In this database, the two most frequently occurring absenteeism diagnosis groups were mental illness (± 22%) and disease of the musculoskeletal system (± 17%). Over the four years, 14,209 absenteeism cases (3.2%) were recorded with a CAS code of interest for this study.
Table 1 presents the baseline characteristics of the included absenteeism cases. The study population is in general representative of the Dutch occupational population. However, there is a relative overrepresentation of employees in the manufacturing and construction sectors and an underrepresentation of the human health and social work activities sector in our study population.Table 1. Baseline characteristics of employees included in the study (n = 14,209)Variablen% of totalSexFemale 356225.1Male10,64274.9Unknown 5 0.0Age class (in years)16–24 146 1.025–34 621 4.435–44 143710.145–54 455632.155+ 744952.4Company employee count0–50010,05970.8500+ 409428.8Unknown 56 0.4*Type of economic sector (top five)Manufacturing 265018.7Wholesale and retail trade; repair of motor vehicles and motorcycles 227016.0Construction 1139 8.0Transportation and storage 1025 7.2Consultancy, research and other specialized business services 997 7.0Other or unknown 612843.1Cardiovascular disease (highest to lowest prevalence)*Acute myocardial infarction 312822.0Cerebrovascular disease 230916.3Cardiac arrhythmia 1323 9.3Unspecified cardiovascular disease 886 6.2Angina 843 5.9Unspecified ischemic cardiac disease 816 5.7Unspecified cardiovascular complaints 758 5.3Hypertension 684 4.8Other cardiac disease 653 4.6Cardiac dysrhythmia 635 4.5Cardiac heart failure 440 3.1High blood pressure 398 2.8Chest pain 371 2.6Pulmonary vascular disease 283 2.0Congenital cardiovascular anomalies 166 1.2Other trauma to vascular system 133 0.9Cardiac conduction disorders 104 0.7Previous myocardial infarction 96 0.7Pulmonary heart failure 68 0.5Traumatic intracranial bleeding 42 0.3Hypotension 34 0.2Other neoplasma of cardiovascular system 28 0.2(Chronic) Rheumatic cardiac disease 11 0.1
The five most prevalent cardiovascular diseases were acute myocardial infarction (22.0%, n = 3128), cerebrovascular disease (16.3%, n = 2309), cardiac arrhythmia (9.3%, n = 1323), unspecified cardiovascular disease (6.2%, n = 886) and angina (5.9%, n = 843). An overview of the occurrence of all cardiovascular diseases is shown in Table 1.
Absenteeism duration
The median duration of absenteeism due to cardiovascular disease in the period from 2019 to 2022 for this population was 119 working days (IQR 156; Q1–Q3 62.9–218.6). Figure 2 illustrates the absenteeism duration for the five most prevalent cardiovascular diseases with durations censored at 521 working days (= two calendar years).Fig. 1. InfographicFig. 2The figure displays the absenteeism duration and the cumulative RTW rate per diagnosis of the top five most occurring diagnoses in the overall population (RTW return-to-work)
Overall, 81.8% (n = 11,628) of the study population had fully returned to work within one year. Table 2 presents the average absenteeism duration and RTW rates categorized by time intervals (< 6 months, 6–12 months, and 12–18 months) for all CVD cases combined and for the five most prevalent diagnoses.Table 2. Absenteeism duration and associated costs overall and per top five diagnosesAll cardiovascular diseaseAcute myocardial infarctionCerebrovascular diseaseCardiac arrhythmiasUnspecified cardiovascular complaintsAnginaP value**Absenteeism duration (median working days*) 119 (IQR 156) 128 (IQR 132) 185 (IQR 230) 95 (IQR 138) 114 (IQR 162) 109 (IQR 124)< 0.001Return to work (cumulative % of total)< 6 months 54.2 51.5 36.8 64.2 55.5 59.7< 0.0016–12 months 81.8 (+27.6) 85.6 (+34.1) 65.1 (+28.3) 86.2 (+22) 81.3 (+25.8) 86.9 (+27.2)< 0.00112–18 months 92 (+10.2) 94.6 (+9.0) 82.8 (+17.7) 93.8 (+7.6) 92.5 (+11.2) 94.1 (+7.2)< 0.001*Associated rough cost-estimate per employee (median €)36,803 (IQR 48,341)39,199 (IQR 40,565)57,199 (IQR 70,765)29,397 (IQR 42,460)34,843 (IQR 49,967)33,537 (IQR 38,546)< 0.001Comparison between the top five diagnoses
Absenteeism-related costs
The associated rough cost-estimate for CVD-related absenteeism in this population amounted to an excess of € 690 million over the four years. For every single employee with CVD, the median cost to employers mounts up to approximately € 37,000. Tab. 2 displays the average associated costs per case for all CVD cases combined and for the five most prevalent diagnoses.
Discussion
In this exploratory study, we used standard-of-care data from two major occupational health services in the Netherlands to examine absenteeism due to cardiovascular disease (CVD) within a large cohort of the Dutch working population from 2019 to 2022. We observed a 3.2% incidence of absenteeism due to CVD, a median absenteeism duration of 119 working days, and a minimum rough cost-estimate for employers of around € 37,000 per employee. Of all CVD diagnoses, cerebrovascular disease was found to be associated with the longest absenteeism duration. For reference, in the Netherlands two frequently occurring causes of absenteeism or work disability are stress-related illness (average absenteeism duration 101 working days; average cost to the employer of € 19,151 per employee [11]) and low back pain (median absenteeism duration 95 days; mean cost to the employer of € 15,350 per employee [17]).
In our study acute myocardial infarction (AMI) and cerebrovascular disease were the two most frequently occurring diagnoses, with an average absenteeism duration of 128 days and 185 days, respectively. These absenteeism durations are quite similar to earlier findings, thus even though medical care has evolved over time, AMI and cerebrovascular disease are still associated with a relatively long absenteeism duration. This highlights the critical importance of focusing rehabilitation efforts on achieving return-to-work (RTW) after AMI and cerebrovascular disease. Effective rehabilitation can help employees resume work, enhance their quality of life, and reduce absenteeism costs.
RTW rates within 12 months after acute coronary syndrome (ACS) range from 67–93%, with an average delay of 2–3 months. Kruse et al. reported 79% RTW after coronary heart disease (CHD) admissions versus 93% after other diagnoses [2]. In our study, approximately 86% of employees returned to work within 6–12 months following AMI. RTW outcomes after CVD are influenced by medical (e.g., ventricular function, ischemia, rhythm stability), occupational (e.g., physical demands, shift work, commuting), and psychosocial factors (e.g., depression, self-perceived health, cognitive impairments) [18, 19]. A multinational review identified six barriers (job strain, anxiety, depression, comorbidity, older age, low education) and four facilitators (job control, work ability, good perceived health, high socioeconomic status) to RTW after CVD [19]. Non-fatal CHD is associated with increased absenteeism, presenteeism, delayed RTW, early labour force exit, and unemployment, challenges that likely extend to AMI survivors, who also face risks such as reduced job responsibilities, part-time work, lower income, and dismissal [5, 19].
Cardiac rehabilitation (CR) uptake in the Netherlands is suboptimal. A nationwide cohort study analysing 106,212 patients with CVD between 2013 and 2019 reported an initial increase in CR participation from 28% in 2013 to 41% in 2016, after which rates stabilized [20]. Previously, RTW rates following CR have shown to be 65% at six months and 67% at twelve months following CR, with predictors including younger age, non-manual work, self-employment, higher quality of life, and favourable exercise ECG outcomes [21]. Although one Danish study indicated a lower probability of RTW at three months following CR, it demonstrated a higher probability at nine and twelve months [22]. In the Netherlands, CR programs are multidisciplinary, comprising exercise training, cardiovascular risk management, psychological support, and occupational counselling, aligned with national and European guidelines. Regarding neurorehabilitation, 86% of patients with acquired brain injury returned to work immediately after a four-month vocational rehabilitation program, with 64% remaining employed at long-term follow-up [23]. Dutch neurorehabilitation similarly integrates physical, cognitive, psychological, and vocational interventions to enhance functional recovery and work reintegration. Interestingly, Yokota et al. demonstrated in a small study population that cardiac rehabilitation following standardized in-hospital rehabilitation improved exercise tolerance and functional strength in patients recovering from cerebrovascular stroke [24].
Implications for clinical practice
Occupational health professionals play a key role in ensuring sustainable reintegration for employees recovering from significant health conditions such as CVD. Their responsibilities include helping employees regain optimal functioning, ideally returning to pre-CVD performance levels, or finding new roles when full recovery is not feasible. Effective reintegration requires enhanced collaboration among medical disciplines such as cardiologists, neurologists, rehabilitation physicians, and occupational health experts. An integrated approach focusing on rehabilitation participation and work-related factors can improve employees’ quality of life, reduce employer costs, and provide broader societal benefits, including higher tax revenues and reduced social security expenses [19]. Person-centred care and digital rehabilitation programs have been shown to improve return-to-work rates after ACS and assist professionals in maintaining progress while resuming work activities [19].
Conclusions
This study demonstrates that cardiovascular disease (CVD) is a primary cause of absenteeism in at least 3.2% of cases within the Dutch labour force. CVD is associated with relatively prolonged absenteeism and incurs substantial costs for employers. Additionally, acute myocardial infarction, cerebrovascular disease, cardiac arrhythmias, unspecified cardiovascular disease, and angina are the most frequently occurring diagnoses among this working population.
We advocate for a greater focus on work-related aspects in both in-hospital and outpatient treatments for CVD. To achieve this, it is essential that in-hospital and outpatient medical specialists collaborate more effectively with occupational health professionals. Furthermore, there is a pressing need for the development of more work-focused guidelines to better integrate occupational health considerations into cardiovascular care.
Limitations
This study, based on a day-to-day occupational healthcare database covering approximately 28% of Dutch employees with absenteeism, likely underestimates the true prevalence and impact of CVD due to delayed diagnosis registration, single-code recording, and overlap with mental health conditions. Extrapolation to the full workforce and to other countries requires caution given systemic differences. Additionally, absenteeism duration was censored for part of the cohort, presenteeism was not assessed, and the friction cost method used may underestimate the true economic burden, suggesting the actual impact of CVD is greater than reported. See the ESMfor a more detailed description of the limitations.
Supplementary Information
Data extraction
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Factsheet WHO on CVD in the world. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-. Accessed 30 Nov 2023.
- 2Virtanen M, Ervasti J, Mittendorfer-Rutz E, et al. Work disability before and after a major cardiovascular event: a ten-year study using nationwide medical and insurance registers. Sci Rep. 2017;7. 10.1038/s 41598-017-01216-210.1038/s 41598-017-01216-2PMC 543072128442715 · doi ↗ · pubmed ↗
- 3structuur arbeidskosten, -duur, bedrijfstak SBI 2008. 2020. https://opendata.cbs.nl/statline/#/CBS/nl/dataset/85291 NED/table?ts=1710407653021. Accessed Internet.
- 4Statline https://opendata.cbs.nl/statline/#/CBS/en/. Accessed 10 Oct 2024.