Noniatrogenic Urethral Trauma in Children: A Narrative Review
Rianne J.M. Lammers, Tudor Enache, Sebastien Faraj, Mieke Waterschoot, Sibel Tiryaki

TL;DR
This review finds that research on accidental urethral injuries in children is of low quality and inconsistent, offering recommendations to improve future studies.
Contribution
The paper provides structured recommendations to enhance the quality and consistency of future research on pediatric urethral trauma.
Findings
Most studies on pediatric urethral trauma are low-quality retrospective single-center cohorts.
The overall stricture rate across treatment modalities is approximately 20%.
Data on repeat surgery and quality of life outcomes are insufficient for firm conclusions.
Abstract
Current evidence on pediatric urethral trauma is fragmented, but clear opportunities exist to improve the quality and comparability of future research. We provide structured recommendations to guide that process. Pediatric urethral trauma is rare, and treatment recommendations are often extrapolated from evidence for adults. We conducted a systematic review of the literature to evaluate management strategies, outcomes, and the quality of reporting for pediatric urethral trauma. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and identified 31 relevant studies published since 1990. Studies were eligible for inclusions if they reported results for five or more patients with at least 3 mo of follow-up for noniatrogenic urethral trauma. Methodological quality was assessed using the Methodological Index for Nonrandomized Studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
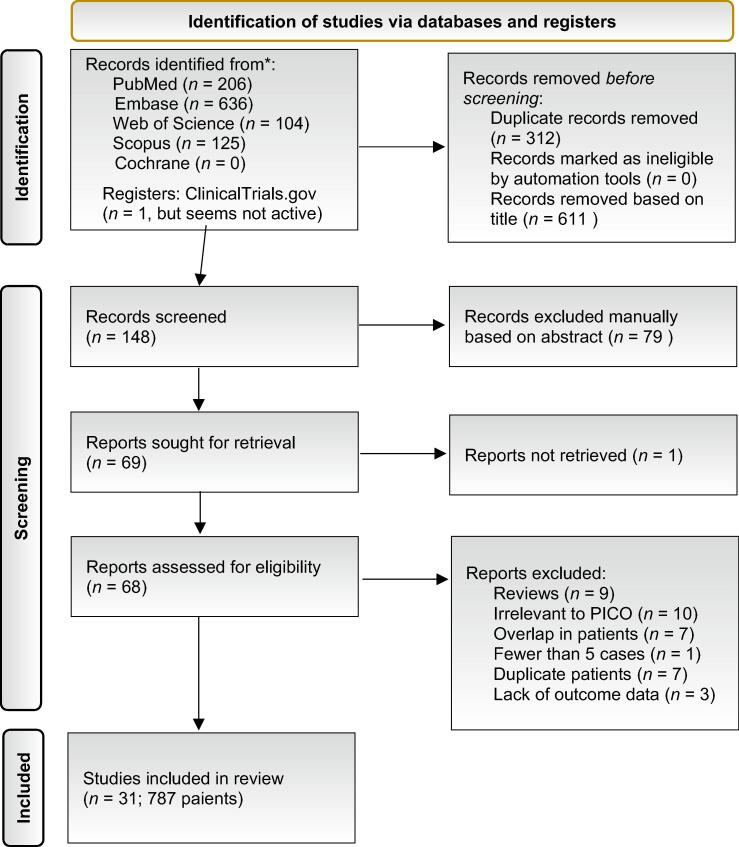 Figure 1
Figure 1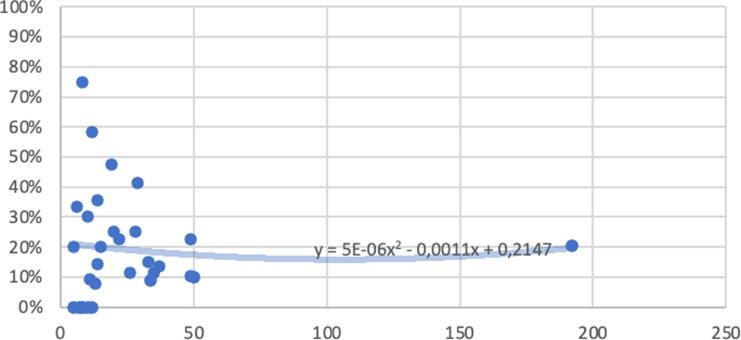 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Urinary Bladder and Prostate Research · Genital Health and Disease
Introduction
1
Urethral trauma among children is rare and accounts for just 3% of traumatic genitourinary injuries in this population [1,2].Treatment recommendations are mainly extrapolated from data for adults. The question is whether it is correct to extrapolate evidence for adults to children, as the latter have unique anatomic differences that need to be taken into account when considering treatment, such as more immature bones and a higher, more intra-abdominal bladder position. These lead to specific variations in urethral trauma in comparison to adults [2]. In addition, the trauma effect in children is different to that in adults: children experience more unstable pelvic fractures, leading to urethral displacement and bladder rupture [3]. Prepubertal girls are more prone to urethral trauma with pelvic fractures owing to the lack of estrogen-related protection [3]. Urethral trauma is a major cause of urethral strictures: 34% of pediatric urethral strictures have a traumatic etiology [1]. This situation highlights the need for a distinct approach to the management of urethral trauma in children and an evaluation of pediatric outcomes, which prompted us to conduct a systematic review.
Methods
2
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and conducted a review of the literature using the EMBASE, PubMed, Web of Science, and Scopus databases. The protocol was registered in the PROSPERO database (CRD42023378468).
The PICO (Population, Comparator, Intervention, Outcome) question was framed as follows:
- –Population: children with urethral trauma (boys and girls; anterior and posterior injury).
- –Intervention: delayed open reconstruction (gold standard in adults).
- –Comparators: early open reconstruction, conservative management, endoscopic management.
- –Outcomes:
- oPrimary: urinary continence, sexual function, stricture rate.
- oSecondary: need for repeat surgery and quality of life (QoL).
The optimal search strategy was identified by testing the ability to retrieve two key control studies [4,5]. The search string was “pediatric urethral trauma”, with the following limitations applied:
- –Child/age from birth up to 18 yr.
- –Only literature published from 1990 onwards (because of changes in guidelines and operation techniques).
- –Only articles in English, Dutch, German, France, Turkish, Russian, or Romanian (the languages spoken in our group).
- –Follow-up of at least 3 mo.
- –Exclusion of case series and studies with fewer than five cases.
- –Exclusion of hypospadias and iatrogenic causes of urethral trauma.
Full-text reading was carried out by two authors per article. One other author (R.J.M.L.) was the independent controller, and checked for reproduction and reliability. If there was a disagreement, a third independent author made the final decision. After group discussion, a data extraction form was set up. Two authors (M.W., S.F.) also checked unpublished data and ongoing studies. Owing to the limited quality of the literature available, a meta-analysis was not feasible; therefore, we present a narrative review.
Statistical analysis
2.1
Data are reported as the median or mean for continuous variable, and the frequency and percentage for categorical variables. Nonparametric tests (Mann-Whitney U test or Fisher’s exact test) were used for data analysis. A p value <0.05 was considered statistically significant.
Quality assessment
2.2
The Methodological Index for Nonrandomized Studies (MINORS) tool [6] was used to evaluate the quality of the studies. This tool gives a maximum of 16 points for noncomparative and 24 for comparative studies.
Results
3
We identified 1071 articles, of which 68 were considered eligible on the basis of their title and abstract. After applying the inclusion and exclusion criteria, 31 articles involving a total of 787 patients were included in the review [4,5,[7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35]]. Figure 1 shows the PRISMA flowchart.Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. PICO = Population, Intervention, Comparator, Outcome.
Quality assessment
3.1
No multicenter studies were identified. Only two articles were nonrandomized comparative studies [11,25]; the rest were cohort studies or case series. All studies but one [25] were retrospective. The mean MINORS score was 8 points (range 4–15; Supplementary Table 1). No relationship was found between the quality of the articles and outcomes.
Early versus late open reconstruction
3.2
A total of 30/31 articles addressed open reconstruction. One article exclusively reported on endoscopic realignment [28] according to a protocol that included delayed repair, which was not ultimately required. For the purpose of this review, we defined “early open reconstruction” as any open surgical approach performed immediately after trauma, as there is no clear definition in the literature. Early open reconstruction was the sole method in one study [18], 20 reported only on delayed repair [4,5,[7], [8], [9],[12], [13], [14], [15], [16], [17],19,20,24,27,[29], [30], [31], [32],35], eight compared early versus delayed open reconstruction [10,11,21,23,25,26,33,34], and one did not specify the timing of surgery [22].
Where data permitted stratification, subgroup analyses were conducted (boys vs girls; anterior vs posterior urethral injury).
Studies including both early and delayed open reconstruction
3.2.1
Of the eight articles evaluating both early and delayed open reconstruction, four included only boys [7,21,23,25], one focused exclusively on girls [26], and three included both sexes [10,11,34]. Among the studies involving boys, six specifically addressed posterior urethral trauma [10,11,21,23,25,33], while one reported on both anterior and posterior urethral trauma [34].
In total, 78 boys underwent early open surgical management, with techniques ranging from simple primary anastomosis to complex reconstruction. Delayed open reconstruction was reported for 56 patients, typically performed 1–6 mo after trauma [10,21,33]. In other studies, the timing was not specified.
With regard to outcomes, an overall repeat surgical procedure was needed in 57 patients (42% of the pooled cohort). These secondary procedures included endoscopic intervention (balloon dilation; urethrotomy) and repeat urethroplasty, with or without buccal mucosa. No further subgroup analysis was conducted.
Studies including only early open reconstruction
3.2.2
Gündoĝdu et al [18] reported results for 11 boys and one girl. In all cases, urethral realignment on a Foley catheter via an open abdominal approach was preferred. No repeat surgery was required.
Studies including only late open reconstruction
3.2.3
The 20 studies reporting on only late open reconstruction involved a total of 611, of whom only 3% were girls. The largest cohort was described by Sreeranga et al [32], with 192 patients (181 boys, 11 girls). Eleven studies reported on posterior urethral trauma [7,8,12,15,16,20,24,27,30,31,35], one addressed anterior urethral trauma [9], and eight reported data for both [4,5,13,14,17,19,29,32]. Table 1 provides an overview of the results for boys. Three studies reported results for only girls or data that allowed separate analysis by sex [9,12,32] (Table 2).Table 1. Overview of studies reporting on late open reconstruction in boysAuthorYearCountryTrauma locationPatientsTechnique and approach usedRepeat proceduresAbdalla [7]2008EgyptPosterior55 posterior parasagittal pararectal perineal approachNone reportedAggarwal [8]2011IndiaPosterior34Primary group: 10 perineal approach with iPBT, 13 abdominoperineal TPA1 complex Monti reconstruction, 1 sUTP, 1 UDL, 1 cystolithotomyRedo group: 1 pure perineal approach, 11 TPA, 7 sUTPBasiri [12]2002IranPosterior77 UTP via abdominal approach with CPDNone reportedChaudhari [13]2021IndiaBoth posterior and anterior1414 transperineal UTP2 UTPChukwubuike [14]2020NigeriaBoth posterior and anterior111 transperineal UTP1 UTPDas [15]2004IndiaPosterior10Urethral anastomosis: 4 transperineal approach, 6 transperineal TPA, 4 omental flap1 UDLEl-Sheikh [16]2008EgyptPosterior15Urethral reconstruction via perineal approach only1 DVIU, 2 UTP via APAGarg [17]2019IndiaPosterior and anterior33PUA: 27 perineal approach, 6 PBT; 4 Mitrofanoff, 1 Badenoch; 1 UTP via TPA + preputial flapNot specifically mentioned, but 1 Clavien-Dindo grade III complicationHafez [19]2005EgyptPosterior and anterior35Perineal approach via an inverted Y incision2 perineal UTP, 2 endoscopic urethrotomyKardar [20]1995Saudi ArabiaPosterior121 perineal approach, 11 APA, 4 cPBT, 7 pPBTNone reportedOrabi [24]2008EgyptPosterior5047 PUA, 3 sUTP; 43 perineal approach; 4 abdominal approach a; 40 no PBT, 3 iPBT, 4 TPA2 excision of urethral diverticulumPodesta [27]2015ArgentinaPosterior49Primary anastomosis: 28 perineal approach, 21 APA, 3 pPBT4 AMR via PPPE, 1 AMR with urethral rerouting, 1 internal urethrotomySetato [29]2021EthiopiaPosterior and anterior1919 pure perineal PUA without PBT4 UTP, 3 UDL, 2 suprapubic cystostomy and waiting for redo surgerySingh [30]2014IndiaPosterior37Urethral anastomosis: 29 pure preanal coronal approach, 8 preanal coronal + TPA2 UTP, 3 UDLSingla [31]2008IndiaPosterior28PUA: 27 perineal approach, 1 perineal + TPA4 DVIU, 2 graft UTP, 1 redo anastomosisSreeranga [32]2022IndiaPosterior and anterior181UTP: 160 perineal approach, 17 abdominal approach + PBT, 4 combined approach26 laser urethrotomy, 13 redo surgery=13Voelzke [4]2012USAAnterior and posteriorAnterior: 8 Posterior: 18Anterior: 5 primary UTP, 3 U-BMG Posterior: PUA in all patients; 12 perineal only, 5 perineal + pPBT, 1 APA3 DVIUWang [35]2021ChinaPosterior83 perineal, 4 perineal + iPBT, 1 transperineal with CDSNone reportedWaterloos [5]2018BelgiumPosterior and anterior1312 PUA, 1graft UTP; 12 perineal approach only, 1 pPBT1 redo via APAAMR = anastamotic repair; APA = abdominoperineal approach; CDS = corporeal dissection and separation; CPD = complete pubic disjunction; DVIU = direct-vision internal urethrotomy; ; PBT = pubectomy; cPBT = complete PBT; iPBT = inferior PBT; pPBT = partial PBT; PPPE = perineal approach with partial pubectomy exposure; PUA = primary urethral anastamosis; TPA = transpubic approach; sUTP = substitution UTP; U-BMG = urethroplasty with buccal mucosal graft; UDL = urethral dilatation; UTP = urethroplasty.aApproach not very clear for the sUTP cases.Table 2. Overview of surgical details for late open reconstruction in girlsStudyPatientsTechnique and approachAhmed [9]5Urethral reconstruction with flipped anterior bladder wallBasiri [12]3Urethroplasty with abdominal approach and complete pubic disjunctionSreeranga [32]11Meatoplasty (n = 2) Reconstruction via an abdominopelvic approach with partial pubectomy (n = 9)
The delay between trauma and definitive surgery was highly variable and was not mentioned in four studies [4,7,27,32]. In four studies the delay was at least 3 mo, but the maximum interval was not reported [5,16,29,35]. In just one study the delay was at least 6 mo [24]. The longest delay reported was 48 mo [8]. The initial management strategy showed great variability because some patients were treated in another center before referral. Nevertheless, initial treatment for most of the patients was placement of a suprapubic catheter.
A summary of the outcomes for early and late repairs is presented in Table 3. We analyzed data for 693 boys and 26 girls. Our aim was provide a comprehensive comparison by combining all cases reported to date; however, not all studies provided patient-level data.Table 3. Overview of studies concerning early and or late open surgeryStudyTimingPatientsContinence rate (%)Stricture rate (%)Redo surgeryAbdalla [7]aLate510020None reportedAggarwal [8]LatePrimary group239149% overall; 1 complex Monti reconstruction; 1 substitution urethroplasty, 1 UDL, 1 cystolithotomyRedo group127516Ahmed [9]Late5 (all girls)100020% overall; 1 augmentation cystoplasty + MitrofanoffAvanoglu [10]Early9662234% overall b; 4 reanastomosis, 2 balloon dilatation, 4 dilatation/endoscopic resectionLate45050Balkan [11]Early12100176 dilatation/urethrotomy, 1 redo urethroplastyLate888386 dilatation/urethrotomy, 2 redo urethroplastyBasiri [12]Late10 (7 boys, 3 girls)80 (100% for boys)0None reportedChaudhari [13]Late141001414% overall; 2 urethroplastyChukwubuike [14]Late1110099% overall; 1 urethroplastyDas [15]Late101003020% overall; 3 UDLEl-Sheikh [16]Late15NR2020% overall; 1 DVIU, 2 urethroplasty via APAGarg [17]Late339715Not specifically mentioned, but 1 Clavien-Dindo grade III complicationGündoğdu [18]Early127558None reportedHafez [19]Late351001111% overall; 2 perineal urethroplasty, 2 endoscopic urethrotomyKardar [20]Late12580No redo reportedNerli [21]Early5100402 IUT, 1 redo urethroplastyLate10100303 IUT, 2 redo urethroplastyOnen [23]Early8882540% overallbLate168125Orabi [24]Late501001012% overall; 2 excision of urethral diverticulumOtgun [25]Early1070NRData not clearLate1100Podesta [26]Early175b0b25% overallb; 2 vaginoplastyLate7Podesta [27]Late49821012% overall; 4 AMR via PPPE, 1 AMR with urethral rerouting, 1 IUTSetato [29]Late19NR4747% overall; 4 urethroplasty, 3 UDL, 2 SPC and waiting for redo surgerySingh [30]Late3710013.56% overall; 2 urethroplasty, 3 UDLSingla [31]Late281002525% overall; 4 DVIU, 2 graft urethroplasty, 1 redo anastomosisSreeranga [32]Late181 boys922222% overall; 26 laser urethrotomy, 13 redo surgery11 girls910None reportedTrachta [33]Early110005 reanastomosis. 1 endoscopic transurethral resectionLate75771Updahyaya [34]Early9783350% overall; 2 redo urethroplasty; 7 UDL; 1 awaiting redoLate58080Voelzke [4]Late26NR1212% overall; 3 DVIUWang [35]Late81000None reportedWaterloos [5]Late139281 redo via APAAMR = anastamotic repair; APA = abdominoperineal approach; DVIU = direct-vision internal urethrotomy; IUT = internal urethrotomy; NR = not reported; PPPE = perineal approach with partial pubectomy exposure; SPC = suprapubic cystostomy; UDL = urethral dilatation.aData for the pediatric group of patients were extracted.bNo separate data.
All female cases underwent delayed repair, which precluded any comparison by timing. Among the male cases, 54 underwent early and 639 underwent delayed repair.
Endoscopic management
3.3
Among all the studies reviewed (regardless of whether they were categorized as deferred management, immediate management, or combined approaches), 14 reported on endoscopic management and outcomes for urethral trauma in children [4,5,10,13,16,17,19,21,[26], [27], [28],32,34,35]. Of these, nine mentioned endoscopic management as failed attempts before referral to the center for final repair [4,5,13,16,17,19,27,32,35].
One study by Podesta and Jordan [26] was on urethral injuries due to pelvic fracture in girls. Three patients were treated with endoscopic realignment and cystostomy, and seven underwent delayed open surgery. The authors reported urethral obliteration for all patients treated endoscopically. The same group reported on male urethral trauma in other studies and did not use endoscopic management in those cases [10,21,28,34]. Table 4 includes a summary of data from these four studies.Table 4. Outcomes for cases with endoscopic managementStudyTrauma locationEM casesBasis for EM selectionTreatment detailsOutcomesAvanoglu [10]Posterior14SPEndoscopic catheter realignment with no anastomosis7 successful, 1 incontinent, 4 required TPU, 2 had no follow-upNerli [21]Posterior7Associated injuries + SPEndoscopic realignment (retrograde/antegrade)All voiding well, no incontinenceSanson [28]Anterior4/7Unclear4 immediate endoscopic realignment 7 endoscopic follow-up7 successfulUpadhyaya [34]Anterior6All patients with anterior traumaUC with endoscopy (7 d for short, 6 wk for long injuries)2 strictures (1 required multiple and 1 required few dilatations)EM = endoscopic management; SP = surgeon’s preference; TPU = transpubic urethroplasty; UC = urethral catheterization.
Urethral stricture
3.4
Among the 31 articles reviewed, only one [22] did not investigate stricture incidence during follow-up. The proportion of patients who experienced stricture was 20% in the early repair group, and 19% in the delayed repair group. The difference was not statistically significant (p = 0.107).
The primary methods for assessing postoperative stricture are summarized in Table 5. Evaluation of urethral stricture relied predominantly on imaging and noninvasive functional assessments. The methods most frequently reported were voiding cystourethrography or retrograde urethrography (22 studies) [4,5,8,12,[14], [15], [16], [17],19,20,23,[25], [26], [27],29,[31], [32], [33], [34]] and uroflowmetry combined with measurement of postvoid residual volume (PVR; 14 studies) [4,5,8,10,13,19,[23], [24], [25],28,[31], [32], [33],35]. Four studies used more invasive procedures: urodynamic studies (UDS) [25,30] in two and routine endoscopy [15,25] in twos. Direct voiding observation was used in one study [29].Table 5. Additional investigations used to evaluate stricturesEvaluation techniqueNumber of studiesVCU or retrograde urethrography22 [3,4,7,11,[13], [14], [15], [16], [17], [18], [19],22,[24], [25], [26],28,[30], [31], [32], [33]]Uroflowmetry with PVR measurement14 [3,4,7,9,12,18,[22], [23], [24],27,[30], [31], [32],34]Invasive urodynamics2 [24,29]Routine endoscopy2 [14,24]Voiding observation1 [28]PVR = postvoid residual volume; VCU = voiding cystourethrography.
The mean stricture rate across studies was 19% (range 0–80%). The variation in stricture rate did not appear to correlate with study size, as shown in Fig. 2, which provides the most visual representation of the results while remaining faithful to the reality of the highly variable findings across the studies.Fig. 2. Scatterplot showing the proportion of patients with stricture as a function of cohort size in terms of the number of patients. Each dot represents a specific cohort. The trend curve, calculated using quadratic polynomial regression, depicts the overall relationship between the proportion of strictures and the cohort size.
Urinary continence
3.5
Of the 31 studies, 29 measured postprocedural urinary continence [5,[7], [8], [9], [10], [11],[13], [14], [15],[17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35]]. The proportion of patients who were continent after treatment was 83% in the early repair group, and 84% in the delayed repair group. The difference was not statistically significant (p = 0.052)
The definition of “dry” and “wet” before and after surgery was inconsistent and not in accordance with the International Children’s Continence Society (ICCS) guidelines [36]. Only Kardar et al [20] defined “dry” as daytime continence, and “wet” as total incontinence, enuresis nocturna, or stress incontinence.
The methods used to determine continence varied. Overall, the continence rate varied from 58% to 100%. Among girls, the continence rate varied from 75% to 100% [9,22,26]. Concerning boys, Aggarwal et al [8], reported a decrease in continence from 91% (21/23) after primary urethroplasty to 75% (9/12) after redo urethroplasty, perhaps related to combined pelvic fracture. Stress incontinence was the most common form in this study. Kardar et al [20] reported a continence rate of 58% (7/12) after combined perineal and abdominal urethroplasty.
Sexual function
3.6
Of the 31 studies, 17 measured erectile function postoperatively [5,7,8,10,[13], [14], [15],20,21,[25], [26], [27],[31], [32], [33], [34]]. The methods used varied significantly, with many studies relying on subjective reports from parents or children rather than standardized clinical assessments. Sreeranga et al [32] found that the incidence of erectile dysfunction (ED) was 29% (18/63) after primary repair, with a 30% improvement during follow-up, and 42% after redo surgery. Good erectile function was reported in 63% and 42% of cases primary and redo, respectively, according to direct questioning of parents and children. Using the validated Urethral Stricture Surgery Patient-reported Outcome Measure (USS-PROM), Waterloos et al [5] identified ED in 33% (2/6) of cases. Onen et al., found with Using an unvalidated tool, Onene et al [23] found that the ED incidence rate after urethral reconstruction was 15% for type B and 29% for type C pelvic fracture. Data from the three studies reporting detailed ED outcomes are summarized in Table 6.Table 6. Erectile dysfunction after urethral trauma in children: assessment and outcomesStudyAssessment technique usedED outcomesSreeranga [32]Ask the parents and childPrimary repairED in 29% (30% of these improved during FU) Partial ED in 8% Good EF in 63% (16% of these developed partial ED during FU) Redo PFUI repairED in 42% (19% of these improved during FU) Partial ED in 16% Good EF in 42%Waterloos [5]USS-PROM2/6 boys evaluated reported EDOnen [23]Unvalidated questionnaireED after URC in 15% (4/27) of type B pelvic fracture cases and 29% (5/17) of type C pelvic fracture casesED = erectile dysfunction; EF = erectile function; FU = follow-up; PFUI = pelvic fracture urethral injury; URC = urethral reconstruction; USS-PROM = Urethral Stricture Surgery Patient-related Outcome Measure.
Quality of life
3.7
Only two studies mentioned systematic evaluation of the patient perspective using a survey that including questions on QoL [5,32]; one study used USS-PROMS [37], and one evaluated psychosexual outcomes [23]. However, only Onen et al [23] reported actual QoL outcomes: a psychiatric evaluation revealed psychiatric disorders in half of the patients and a lack of appropriate education during hospitalization. The number of urological procedures, the presence of long-term complications, and the number of hospitalizations were independent predictors for development of a psychological disease [23].
Follow-up
3.8
Follow-up ranged from 3 mo to 264 mo. The longest follow-up reported (up to 22 yr) was in the study by Podesta and Podesta [27]. Average, median, or mean follow-up duration could not be calculated as individual data were unavailable. Most studies mentioned follow-up extending to 5 yr after surgery, but unfortunately did not report outcomes at that time, raising questions about long-term results.
The nature of follow-up varied significantly across studies. Most described follow-up assessments that included a medical history, physical examination, and uroflowmetry ± PVR measurement in their methods section. However, only a few studies provided detailed uroflowmetry results, such as maximum flow velocity (Qmax) [7,13,19,21,25,28,33].
In some cases, video cystourethrography (VCUG) and/or a retrograde urethrogram (RUG) and/or cystoscopy were routine follow-up procedures, while in others these were performed only if stricture was suspected. UDS (or video UDS) was performed in a few studies, mainly in cases of urinary incontinence. Two studies performed UDS in all patients. Singh et al [30] found normal values in all except two cases: one had a high-pressure, low-capacity bladder, and the other had uninhibited detrusor contractions. Both patients were treated with anticholinergics. Otgun et al [25] compared 11 boys with posterior urethral trauma to 12 healthy control subjects and found significantly lower bladder capacity, compliance, and Qmax in the trauma group.
Discussion
4
Our aim was to provide insights into clinical treatment of urethral trauma in children, but data inconsistencies posed challenges. A classification scheme is also lacking. Classifications have been published by Goldman et al [38] and Moore et al [39], but these are not used in clinical practice. The guidelines for adults only use the anterior and posterior urethra for classification, as we did in the review. In this section we summarize key observations from the literature and guidance for future research.
Early versus late open reconstruction
4.1
No clear conclusions could be drawn regarding early versus late open reconstruction because of insufficient data, including the lack of a well-defined timeline for previous surgeries and inadequate reporting on techniques. Various surgical techniques were used among the studies, but often insufficient details were reported, and terms such as “operative urethral realignment” and “immediate operative urethral repair” were confusing. In studies discussing delayed open reconstruction [4,7,27,32], a definition of “delay” was frequently absent or inconsistent. If a late open reconstruction was chosen, placement of a suprapubic catheter at the time of the trauma was the usual approach. The delay until definitive surgery was highly variable (3–48 mo), with a delay of 3 mo often deemed acceptable without high-level evidence. Unfortunately, only one study provided an explanation [8], with the delay attributed to initial management performed elsewhere. Overall, early and late repairs appeared to result in similar rates of urinary continence and stricture formation, but conclusions are limited by incomplete data reporting.
Endoscopic management
4.2
The major issue for studies on endoscopic management is inconsistent outcome reporting and a lack of patient selection criteria. The data available suggest that endoscopic management might be suitable for some patients, but there is little information on patient selection, which was sometimes based on the surgeon’s preference [10,21]. Two studies favored endoscopic treatment for all anterior injuries [28,34], with one center avoiding this strategy for posterior cases [34]. Overall, endoscopic management was chosen by few centers and applied to a limited number of patients, with success mainly observed in male cases.
Urethral stricture
4.3
The methods for assessing and evaluating urethral stricture after surgery varied considerably across the studies. RUG or VCUG remained the preferred approach for visualizing the location and length of strictures, despite the radiation dose and invasiveness for children. However, these modalities are the most reliable for diagnosing recurrence. Invasive UDS appears to be underutilized, as only it was only performed in two studies [25,30]. UDS helps in distinguishing dysfunctional voiding from a true stricture, especially when using video UDS. Although this modality is invasive, it does not require general anesthesia (as cystoscopy does), but it might not be available in all clinics. By contrast, uroflowmetry with PVR measurement offers a simple, repeatable, and effective method for evaluation stricture occurrence in potty-trained children. The significant variation in stricture rates reported seemed to be independent of study size, suggesting that factors other than patient volume influenced these rates. Despite this variability, regression analysis for the overall trend revealed a consistent stricture rate of approximately 20% and a likelihood of convergence with increasing patient numbers.
Urinary continence
4.4
Regarding urinary continence, a major limitation is the lack of assessment and definition. Of the 31 studies included in the review, only one used a continence assessment tool [23], which highlights the need for more rigorous and uniform methods, such as validated questionnaires. The ICCS guidelines [36] delineate clear definitions for enuresis and incontinence, but these were rarely referenced, probably because many of the studies were published before the ICCS guidelines publication in 2016.
Urinary continence rates ranged from 58% to 100% following posterior urethral repair, and from 75% to 100% after for anterior urethral repair. These broad ranges suggest that trauma severity and individual patient characteristics play significant roles in outcomes. Numbers improved over the years, with a continence rate of 58% in 1995 [20] versus 92% in 2018 [5], suggesting positive evolution of surgical techniques.
Stress urinary incontinence was the most frequent type, but was often transient [22,27,30]. This can be explained by an improvement in the hypertrophic bladder muscle initially luxated by the urethral stricture and the proximity of the external sphincter mechanism to the surgical area.
Redo operations are associated with greater fibrosis and poor blood flow, which increase the risk of incontinence [8]. Despite these challenges, total incontinence was not observed after reconstruction.
Sexual function
4.5
ED following urethral trauma is underexplored because of the challenges in assessing sexual function in pediatric populations. Many affected boys are prepubescent, which limits the ability to assess erectile function. ED rates reported ranged from 0% to 46% [5,13,26,27,33]. The data may be biased, as boys with ED may be more likely to seek follow-up care, whereas those without ongoing problems are often lost to follow-up.
Hermosa et al [40] identified older age and urethral stricture length as potential risk factors for ED. Nontransecting urethroplasty techniques may reduce vascular damage and thus the risk of ED, but clinical evidence remains limited [41].
Waterloos et al [5] suggested that ED is more likely to attributable to the neurovascular damage caused by the trauma itself. Hermosa et al [40] also observed that ED following surgery is often transient, in agreement with findings reported by Sreeranga et al. [32].
Quality of life
4.6
The literature on pediatric urethral trauma lacks data on QoL. Only three studies mentioned QoL [5,23,32] and just two used a validated survey [5,32]. A major drawback is that the only validated survey is for individuals aged ≥16 yr. The USS-PROMS questionnaire, which was validated for adults in 2013 [37], does not address urinary incontinence or sexual function. These domains were added in the Dutch version by Verla et al [42]. There is no PROM for younger children.
Onen et al [23] highlighted disruption of education as another problem. Future studies should take this factor into consideration.
Follow-up
4.7
There is little consensus on follow-up duration or on what follow-up investigations are most relevant and necessary. Given that uroflowmetry with PVR measurement is a simple, noninvasive, and easily repeatable test, we believe that this should be a standard component of follow-up.
According to the European Association of Urology (EAU) guidelines on urethral strictures in adults, cystoscopy or RUG should be used to assess anatomic success after urethroplasty, as well as PROMs to assess subjective outcomes and validated questionnaires to evaluate sexual function [43]. As most recurrences occur within the first year, the EAU guidelines recommend at least 1 yr of follow-up, with tailoring of the protocol according to health costs and risks. No follow-up information is provided in other EAU guidelines (urological trauma, pediatric urology).
The American Urological Association (AUA) guidelines on urotrauma recommend monitoring for complications (stricture, ED, and urinary incontinence) for at least 1 yr, using uroflowmetry, RUG, cystoscopy, or a combination of these [44]. No specific strategy is recommended for tracking ED or incontinence. The AUA guidelines on urethral stricture advise monitoring for symptomatic recurrences, but no consensus has been reached on the optimal postoperative surveillance protocol.
Recommendations for further research
4.8
We propose several recommendations for future studies (Table 7), such as the development of PROMs for children with urethral trauma that include domains for sexual function and urinary continence. Parents should be counseled about the risk of ED and urinary incontinence, and encouraged to discuss these issues with their children at an age-appropriate time, seeking urological consultation if necessary. Greater awareness of the social impact of urethral trauma in children, including disruption of education, is needed.Table 7. Suggestions for reporting urethral trauma in childrenTopicRecommendationsStudy groupIn studies with a combined patient group, consider presenting results separately by subgroups:
- •Females, male posterior urethra, male anterior urethra
- •Previous interventions: number and type of interventions
- •Patients before versus after puberty Interventions
- •Define interventions in detail
- •Consider giving details about drainage/urethral catheterization method before and after surgery
- •Define the timing of surgery, and the interval between trauma and surgery for delayed surgery
- •Define the selection criteria when using more than one technique Outcome
- •Present outcome data regarding stricture, urinary continence, sexual function, and quality of life
- •Define the evaluation methods for all outcomes
- oSurveys, clinical assessment strategies, radiological techniques, uroflowmetry, endoscopy
- oConsider using validated surveys or defining objective criteria (eg, stricture length)
- oConsider using patient-related outcome measures
- •Define the timeline for outcome assessment
- •Continue long term follow-up to evaluate sexual function during puberty and adulthood
Conclusions
5
Our review addressing a rare condition offers a structured overview of the literature on traumatic urethral trauma in children, covering 31 studies and 787 patients. Most striking is the poor quality and inconsistency of the evidence. Open surgery is more common than endoscopic management, and the overall postoperative stricture rate is approximately 20%. Urinary continence and sexual function are well preserved, as postoperative incontinence and ED are usually short-lived and recover in the majority of the patients over time. QoL is under-reported because of a lack of validated questionnaires.
We provide a dedicated table of recommendations to improve future studies, including the use of standardized definitions, validated pediatric PROMs, and consistent long-term follow-up.
Author contributions: Rianne J.M. Lammers had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Lammers, Tiryaki.
Acquisition of data: Lammers, Enache, Faraj, Waterschoot, Tiryaki.
Analysis and interpretation of data: Lammers, Enache, Faraj, Waterschoot, Tiryaki.
Drafting of the manuscript: Lammers.
Critical revision of the manuscript for important intellectual content: Lammers, Enache, Faraj, Waterschoot, Tiryaki.
Statistical analysis: Lammers, Faraj, Tiryaki.
Obtaining funding: None.
Administrative, technical, or material support: Lammers, Enache, Faraj, Waterschoot, Tiryaki.
Supervision: Lammers, Tiryaki.
Other: None.
Financial disclosures: Rianne J.M. Lammers certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
Acknowledgments: We would like to thank Mirjam Harms and Vladimir Orlov for their help in the first stages of the literature search. We also thank Lisette ‘t Hoen for helping with the basic concept of the narrative review. We used AI (chat GPT) to improve the fluidity of certain parts of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vetterlein M.W.Weisbach L.Riechardt S.Fisch M.Anterior urethral strictures in children: disease etiology and comparative effectiveness of endoscopic treatment vs. open surgical reconstruction Front Pediatr 72019510.3389/fped.2019.0000530805317 PMC 6371027 · doi ↗ · pubmed ↗
- 2Radmayr C.Bogaert G.Bujons A.EAU guidelines on paediatric urology 2024 European Association of Urology Arnhem, The Netherlands
- 3Wein A.Kavoussi L.R.Novick A.C.Partin A.W.Peters C.A.Campbell-Walsh urologyed. 102012 Elsevier Philadelphia, PA
- 4Voelzke B.B.Breyer B.N.Mc Aninch J.W.Blunt pediatric anterior and posterior urethral trauma: 32-year experience and outcomes J Pediatr Urol 8201225826310.1016/j.jpurol.2011.05.01021664873 PMC 3565598 · doi ↗ · pubmed ↗
- 5Waterloos M.Verla W.Spinoit A.F.Urethroplasty for urethral injuries and trauma-related strictures in children and adolescents: a single-institution experience J Pediatr Urol 152019176.e 1176.e 710.1016/j.jpurol.2018.11.01430581060 · doi ↗ · pubmed ↗
- 6Slim K.Nini E.Forestier D.Kwiatkowski F.Panis Y.Chipponi J.Methodological Index for Non-randomized Studies (MINORS): development and validation of a new instrument ANZ J Surg 73200371271610.1046/j.1445-2197.2003.02748.x 12956787 · doi ↗ · pubmed ↗
- 7Abdalla M.A.A posterior sagittal pararectal approach for repair of posterior urethral distraction injuries Eur Urol 53200819119610.1016/j.eururo.2007.06.00817628324 · doi ↗ · pubmed ↗
- 8Aggarwal S.K.Sinha S.K.Kumar A.Pant N.Borkar N.K.Dhua A.Traumatic strictures of the posterior urethra in boys with special reference to recurrent strictures J Pediatr Urol 7201135636210.1016/j.jpurol.2011.03.00321527235 · doi ↗ · pubmed ↗