Measuring the continuation of antidepressant exposure prior to, during, and after pregnancy: A scoping review protocol
Lauren S. Tailor, Hilary K. Brown, Jessie Cunningham, Simone N. Vigod, Erzsébet Horváth-Puhó, Sonia M. Grandi, Xiaoqin Liu, Xiaoqin Liu, Xiaoqin Liu

TL;DR
This scoping review aims to summarize how antidepressant use has been measured before, during, and after pregnancy in existing studies.
Contribution
The study introduces a systematic protocol to evaluate how antidepressant continuation is measured in perinatal research.
Findings
The review will categorize studies based on timing, duration, and adherence to antidepressant use.
It will identify gaps in how exposure is ascertained in prior research.
Findings will inform a clearer definition of continued antidepressant exposure for future studies.
Abstract
The goal of this scoping review is to summarize how prior studies have measured antidepressant continuation/discontinuation prior to, during, and after pregnancy. Pregnant individuals and healthcare providers are faced with difficult decisions about whether to continue antidepressants in pregnancy due to the historical exclusion of pregnant women from clinical trials and the lack of rigorous evidence to support these decisions. Prior studies examining the effects of pre- and perinatal antidepressant use on perinatal outcomes using observational data have been inconsistent, primarily due to the binary (ever/never) categorization of exposure, which may not accurately reflect real-world use. The population for this review consists of pregnant individuals. The concept is the measurement of continued preconception, prenatal, and postpartum antidepressant use. We will include human studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
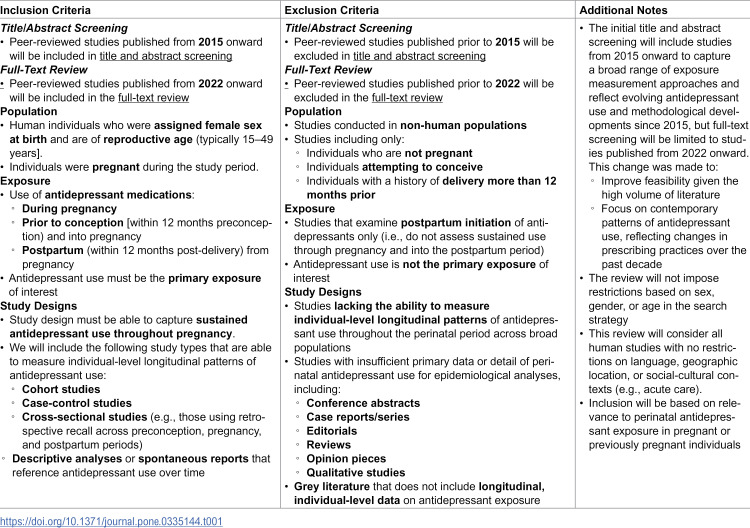 Figure 1
Figure 1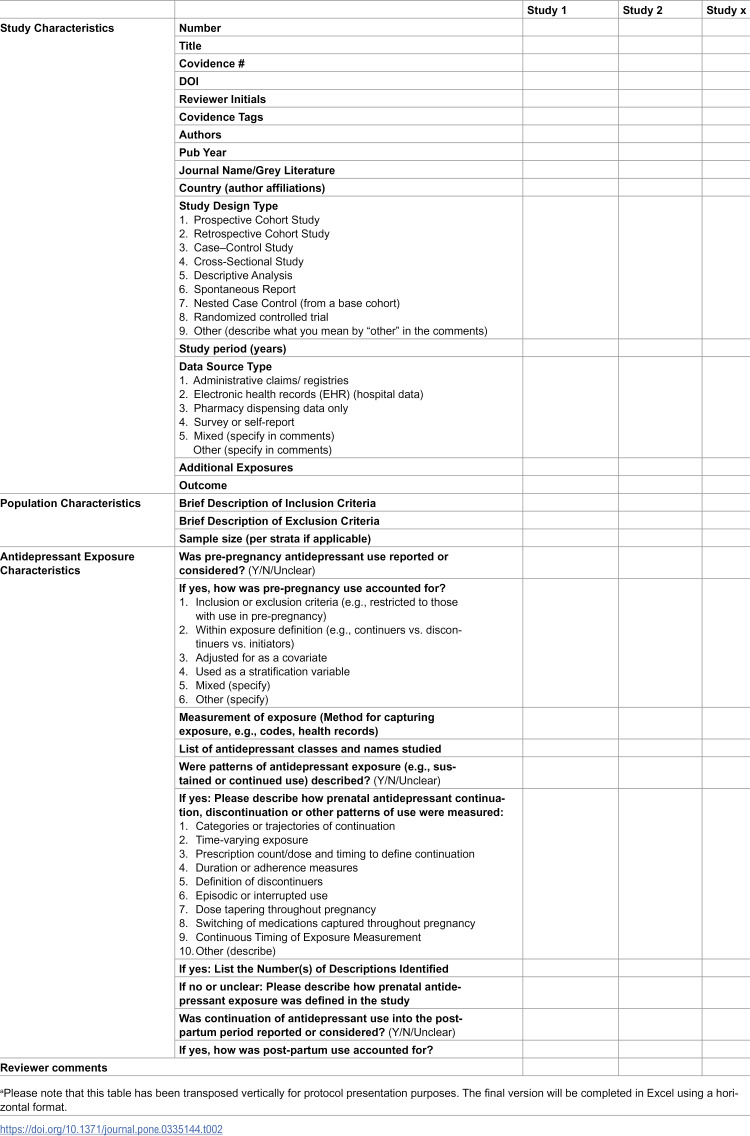 Figure 2
Figure 2- —http://dx.doi.org/10.13039/501100000024Canadian Institutes of Health Research
- —http://dx.doi.org/10.13039/501100000024Canadian Institutes of Health Research
- —Edwin S.H. Leong Centre for Healthy Children 2025 Studentship Award
- —http://dx.doi.org/10.13039/501100016197Leslie Dan Faculty of Pharmacy, University of Toronto
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Pregnancy and Medication Impact · Pregnancy and preeclampsia studies
Introduction
Mental health disorders, such as depression and anxiety, are highly prevalent in pregnancy, with approximately 20–25% of pregnant individuals experiencing symptoms of depression or anxiety [1–4]. If untreated, depression and anxiety can negatively impact maternal well-being and offspring health, emphasizing the need for appropriate treatment, such as antidepressant therapy [1–4]. Antidepressants are among the most commonly prescribed medications in pregnancy, with a global prevalence ranging from 3–8% [5, 6]. However, prenatal antidepressant use has been associated with an elevated risk of certain adverse maternal and fetal health outcomes, such as gestational diabetes and preterm birth [7–13]. Consequently, pregnant individuals and healthcare providers are faced with difficult decisions about whether to continue antidepressants when trying to conceive, during pregnancy, and post-partum (i.e., during breastfeeding) based on factors such as disease severity, potential risks, and patient and provider experience and preference [14–17]. These decisions are complicated by uncertainty surrounding the effect of continuing antidepressant use throughout the perinatal period (i.e., continuing throughout pregnancy vs. discontinuing) on maternal and offspring health, limiting evidence-based clinical decision-making. Therefore, there is a need to examine the effect of continuing antidepressants in pregnancy on maternal and offspring outcomes.
While clinicians often rely on randomized trials as the gold standard for estimating causal effects, these studies typically exclude pregnant or breastfeeding individuals due to ethical concerns over maternal and fetal safety and feasibility issues (e.g., limited pool of eligible/willing participants, rare exposures/outcomes, and challenges with long-term follow-up) [14-16, 18]. As such, healthcare providers and patients must frequently make treatment decisions based on post-marketing surveillance data, health registries, case reports, and observational studies using health administrative and claims databases [14, 19]. Importantly, prior observational studies commonly classify use of prenatal medications as “ever” vs. “never exposed” throughout pregnancy or by trimester, which does not accurately reflect real-world sustained use of medications and ignores important aspects, such as timing of initiation and discontinuation [15, 16, 20]. Considering the timing of medication initiation is crucial in studies examining medication use during pregnancy, as there are critical periods of fetal development when the fetus may be more vulnerable to the harmful effects of certain medications or exposures [21, 22]. For example, classifying antidepressant timing solely by trimester can lead to exposure misclassification, as it ignores sensitive time windows within each trimester; for instance, the embryonic heart undergoes major structural development between weeks 3–8 of gestation [23], so a general “first trimester” exposure categorization could obscure associations between antidepressant exposure during this time window and congenital heart defects [16]. While some studies report the duration of exposure (e.g., number of weeks or trimesters of use) or classify medication use based on dose (high, medium, low dose), there is a lack of standardization in how cumulative duration and dose-response are captured, and these approaches often do not adequately account for changes in medication exposure or dose over time [16]. As such, more granular definitions of real-world antidepressant exposure during pregnancy are needed, particularly since outcomes have periods of sensitivity to specific treatment exposures, meaning clinicians and patients may be likely to alter treatment regimens early in or before the perinatal period (e.g., they may decide to continue, modify, or discontinue therapy). Longitudinal measures of continuation or discontinuation of medication use that account for preconception patterns of antidepressant use are therefore necessary.
Research focused on the sustained use of antidepressants after pregnancy and into lactation is also limited [24], and improved methods of measuring the continuation of postpartum antidepressant use are needed. Moreover, the ascertainment of key characteristics of antidepressant use, such as dose, class, timing, duration, and indication for use, varies across studies, underscoring the need for a standardized approach. Establishing consistency in these measures is essential, as they can significantly influence clinicians’ and patients’ decisions on whether to continue or discontinue antidepressant treatment before, during, or after pregnancy, including during lactation (as this may impact the decision of formula vs. breastfeeding).
As such, this review aims to identify and summarize the extent to which prior studies of perinatal antidepressant exposure have accounted for or measured the continuation of antidepressant exposure prior to, during, and after pregnancy among pregnant individuals in all scoping review contexts (i.e., geographic, social, or cultural settings) [25]. A preliminary search of MEDLINE, Open Science Framework (OSF), the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis was conducted to identify current or underway systematic reviews or scoping reviews on the topic of measuring continued antidepressant exposure throughout the perinatal period, and none were identified. Scoping review methodology is more appropriate here than a systematic review or meta-analysis as the intent is to clarify key concepts/definitions in the literature, and identify and analyze knowledge gaps, as opposed to forming a conclusion around a prevalence, risk factor or effect size of an intervention [26].
Review question(s)
i. How have previous studies measured the continuation of antidepressant exposure a) prior to, b) during, and c) after pregnancy (i.e., binary exposures, sustained use, measurement of lactation)?ii. What specific characteristics have previous studies measured concerning continued antidepressant exposure prior to, during, and after pregnancy (e.g., indication, dose, duration, timing)?
Materials and methods
Ethics approval
This review is part of LT’s doctoral thesis, which has received ethics approval from the Research Ethics Boards of the University of Toronto (HPR-00055550-V0001.0000-O), Aarhus University (REB# 2016-051-000001/810), and the Hospital for Sick Children (REB# REB 1000080862).
Eligibility criteria
Table 1: Eligibility Criteria.
Participants
As described in Table 1, we will include studies examining human pregnant individuals who continue to use antidepressants throughout the perinatal period, defined as use during pregnancy as well prior to conception (within 12 months preconception) continuing into pregnancy and after pregnancy (continued use within 12 months post-delivery), with a focus on sustained use throughout pregnancy (i.e., not postpartum initiation of antidepressants). We will exclude studies that focus on non-human populations or only include individuals who are not pregnant, attempting to conceive, or have a history of delivery more than 1 year prior. We will not impose other population restrictions (i.e., we will include individuals with comorbidities or co-existing conditions) [27]. Concerning sex and gender, this review will focus on perinatal antidepressant exposure, meaning only conceiving, pregnant, or previously pregnant individuals of reproductive age (assigned female sex at birth, generally 15–49 years [28, 29]) will inherently be included, although we will not limit the search by sex, gender, or age.
Concept
The main concept of interest for this scoping review is how prior studies have measured and defined continued antidepressant use throughout the preconception, prenatal, and postpartum periods, for all antidepressant classes, particularly concerning continued use throughout the perinatal period and the categorization of continued antidepressant use (i.e., binary, categorical (i.e., ever, never, sometimes)). Since the focus of our concept is the measurement of continued antidepressant use during the perinatal period, we are also interested in specific factors that are measured in relation to antidepressant exposure, such as indication, dose, class, trimester/timing, and/or cumulative duration of use. Therefore, an additional element of our concept of interest will be the characteristics of antidepressant use.
Context
This review will consider all human studies with no restrictions on language or geographic location. As described by Peters et al., the context of a scoping review includes details on location, social-cultural factors, or sex-based factors [27]. We will not restrict based on location or social-cultural contexts (e.g., acute care).
Types of sources
As per Peters et al., reviews can limit study designs based on the research question and when the team believes certain designs are unlikely to contain relevant information [25]. Since we aim to summarize continued perinatal antidepressant exposure, we will include study designs that allow for the analysis of temporal assessment of exposure with longitudinal data prior to, during, or following a pregnancy. We will, therefore, limit our search to peer-reviewed studies that capture patterns or trends in exposure with the following study designs: cohort studies, cross-sectional studies (i.e., where women recall preconception, prenatal, and postpartum use), case-control studies, and descriptive analyses or spontaneous reports that reference use of medications over time. We will exclude studies that lack the ability to measure individual-level longitudinal patterns of antidepressant use throughout the perinatal period across broad populations, as well as those that have insufficient primary data or detail of use (e.g., conference abstracts, case reports/series, editorials, reviews, and opinion pieces). A search of the grey literature will be performed using the first five pages of Google, Google Scholar, and Canada’s Drug Agency Grey Matters tool (formerly the Canadian Agency for Drugs and Technologies in Health (CADTH) Grey Matters Guide) Advisories and Warnings section to examine surveillance data from pharmaceutical or public health agencies [30]. As with peer-reviewed studies, included grey literature must have longitudinal data of individual-level antidepressant exposure to be included.
Study design
The proposed scoping review will be conducted in accordance with the JBI methodology for scoping reviews [31] and the protocol will be reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for protocols (PRISMA-ScR) [27, 32]. As noted by Munn et al. and previously described, scoping reviews are indicated when researchers seek to clarify key concepts/definitions in the literature and identify and analyze knowledge gaps, making the scoping review format the most appropriate for this research question [26]. This protocol has been registered in OSF (https://osf.io/2ewpq).
Search strategy
The search strategy aims to locate published studies. A three-step search strategy will be used in this review as per the JBI Manual for Evidence Synthesis [33]. First, an initial limited search of MEDLINE (PubMed) will be conducted to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles and the index terms used to describe the articles will be used to develop a full search strategy for Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily; Ovid Embase Classic + Embase; Ovid APA PsycInfo; Ovid EBM Reviews Central Register of Clinical Trials; and Clarivate Web of Science Core Collection (see S1 File. Complete Literature Search Strategy). Grey literature sources will be identified using previously described methods. With guidance from an expert librarian (JC), the search strategy, including all identified keywords and index terms, will be adapted for each included database and/or information source. The reference lists of all included sources of evidence will be screened for additional studies.
While the initial abstract screening will include studies published from 2015 onward to capture a broad range of potentially relevant literature, the full-text review will be limited to studies published from 2022 to 2024. This decision was made to improve feasibility given the high volume of eligible studies and to ensure that the review reflects contemporary patterns of antidepressant use during pregnancy. Over the past two decades, prenatal antidepressant prescribing has shifted, with a decline in the use of older, less selective antidepressants and a rise in the use of more selective agents, such as selective serotonin reuptake inhibitors (SSRIs). Limiting the full-text review to more recent publications ensures a focus on research that aligns with current prescribing practices, safety profiles, and clinical guidelines, thereby increasing the relevance of our findings for contemporary clinical decision-making [34]. This timeframe limitation was chosen pragmatically to manage the volume of literature and ensure relevance to contemporary prescribing patterns, while still capturing a range of exposure measurement approaches. Non-English language articles will be translated when needed, and artificial intelligence software (e.g., Deep-L [35–37] and CUBBITT [37, 38] have been shown to be highly reliable, with CUBBIT exhibiting increased fluency) to translate non-English studies may be used in addition to human translators, as have been used in previous scoping reviews [39].
Study selection
Following the search, all identified citations will be collated and uploaded into Covidence screening software (Veritas Health Innovation, Melbourne, Australia), and duplicates will be removed. All identified titles/abstracts will be screened independently by at least two independent reviewers based on the inclusion criteria for the review. We will conduct a pilot test of 50 titles/abstracts and 10 full-text articles prior to conducting the official screening to ensure that the eligibility criteria are sufficient and clear, with a goal of 75% agreement [25]. The references of included studies will be scanned to identify studies not identified in the original search. All studies identified in the title/abstract screening stage that meet the inclusion criteria will proceed to full-text review. At the full-text review stage, we will apply more detailed eligibility criteria and extract relevant data. Reasons for the exclusion of full-text papers that do not meet the inclusion criteria will be recorded and reported in the scoping review. Any conflicts will be resolved through discussion or by a third independent reviewer. Search results and the study inclusion process will be reported in full in the final scoping review and presented in a PRISMA flow diagram [40].
Data extraction
Relevant information from the studies, including year of publication, country, design, objectives, study population, definition and measurement of continued pre- and perinatal antidepressant use, indication, method of ascertainment of indication, and outcomes examined, will be extracted by two independent reviewers using a data extraction tool developed by the reviewers. Any conflicts will be resolved through discussion or by a third independent reviewer. A risk of bias assessment will not be conducted as per scoping review guidelines [25]. The draft data extraction tool (refer to Table 2) will be modified and revised as necessary during the data extraction process, and all modifications will be detailed in the full scoping review. If appropriate, the authors of included papers will be contacted to request missing or additional data, where required.
Table 2: Draft data extraction instrumenta.
Since this study is a scoping review, all data underlying the findings will be derived from published, peer-reviewed articles or grey literature that are already available in the public domain. A complete list of included studies will be provided as a supplementary file with the final manuscript. The extracted data will also be made available as supplementary tables at the time of publication.
Data analysis and presentation
We will use descriptive statistics to summarize the characteristics of included studies (e.g., the number and proportion of studies reporting specific medication classes/types). A summary of the characteristics of antidepressant use (i.e., dose, class, trimester/timing, and duration) will also be displayed in tables. To ascertain how continued antidepressant use has been captured, we will first report the number of studies that consider versus do not consider antidepressant continuation during pregnancy and then will categorize studies based on the robustness of their measurement of continued antidepressant use (considering factors such as timing, duration, adherence, exposure ascertainment, etc.). Study details will be presented as tables or figures (e.g., word heat maps, waffle charts) as described by Pollock et al [41] where appropriate. Tabular or diagrammatic data will be accompanied by a narrative summary to illustrate key findings.
Scoping review timeline
As this is a scoping review of the available literature, no participant recruitment is involved. Title and abstract screening have been completed as of June 18, 2025. Full-text screening has been completed as of July 7, 2025. Data extraction is underway and expected to be completed by October 2025. We anticipate that results will be available by December 2025.
Discussion
This protocol provides an overview of the methods for conducting a scoping review to summarize how prior studies have measured continued and sustained antidepressant exposure prior to, during, and after pregnancy. This review will identify key methodological strengths, limitations, and gaps in the literature, ultimately informing a clear definition of continued antidepressant exposure to be used in future studies. Establishing a clear and consistent definition of sustained chronic medication use, such as antidepressant use, in pregnancy is critical for improving comparability across studies, enhancing the validity of findings, and guiding clinical and policy decision-making regarding perinatal antidepressant use. The results from this review will be disseminated widely through conference presentations (e.g., The European Perinatal and Paediatric Epidemiology Conference) and at least one peer-reviewed journal publication.
Supporting information
S1 FileComplete Literature Search Strategy.(DOCX)
S2 FileChecklist- PRISMA-P 2015 Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bedaso A, Adams J, Peng W, Sibbritt D. The association between social support and antenatal depressive and anxiety symptoms among Australian women. BMC Pregnancy Childbirth. 2021;21(1):708. doi: 10.1186/s 12884-021-04188-4 34686140 PMC 8532351 · doi ↗ · pubmed ↗
- 2Dadi AF, Miller ER, Bisetegn TA, Mwanri L. Global burden of antenatal depression and its association with adverse birth outcomes: an umbrella review. BMC Public Health. 2020;20(1):173. doi: 10.1186/s 12889-020-8293-9 32019560 PMC 7001252 · doi ↗ · pubmed ↗
- 3Bérard A, Gorgui J, Tchuente V. The COVID-19 Pandemic Impacted Maternal Mental Health Differently Depending on Pregnancy Status and Trimester of Gestation. IJERPH. 2022; 19(5).10.3390/ijerph 19052926 PMC 891061435270623 · doi ↗ · pubmed ↗
- 4Trinh NTH, Munk-Olsen T, Wray NR, Bergink V, Nordeng HME, Lupattelli A, et al. Timing of Antidepressant Discontinuation During Pregnancy and Postpartum Psychiatric Outcomes in Denmark and Norway. JAMA Psychiatry. 2023;80(5):441–50. doi: 10.1001/jamapsychiatry.2023.0041 36884236 PMC 9996461 · doi ↗ · pubmed ↗
- 5Molenaar NM, Bais B, Lambregtse-van den Berg MP, Mulder CL, Howell EA, Fox NS, et al. The international prevalence of antidepressant use before, during, and after pregnancy: A systematic review and meta-analysis of timing, type of prescriptions and geographical variability. J Affect Disord. 2020;264:82–9. doi: 10.1016/j.jad.2019.12.014 31846905 · doi ↗ · pubmed ↗
- 6Ashley JM, Harper BD, Arms-Chavez CJ, Lo Bello SG. Estimated prevalence of antenatal depression in the US population. Arch Womens Ment Health. 2016;19(2):395–400. doi: 10.1007/s 00737-015-0593-1 26687691 · doi ↗ · pubmed ↗
- 7Abosi O, Lopes S, Schmitz S, Fiedorowicz JG. Cardiometabolic effects of psychotropic medications. 2018;36(1).10.1515/hmbci-2017-0065 PMC 681851829320364 · doi ↗ · pubmed ↗
- 8Alonso-Pedrero L, Bes-Rastrollo M, Marti A. Effects of antidepressant and antipsychotic use on weight gain: A systematic review. Obes Rev. 2019;20(12):1680–90. doi: 10.1111/obr.12934 31524318 · doi ↗ · pubmed ↗