Right focal atrial tachycardia following closure of patent foramen ovale with an amplatzer septal occluder device: case report
Ahmed Makni, Jerome Bouet, Sophia Mzoughi, Jerome Taieb

TL;DR
A rare case of right atrial tachycardia occurred years after a patent foramen ovale closure and was successfully treated with radiofrequency ablation.
Contribution
This is the first reported case of late-onset right focal atrial tachycardia following PFO closure with an Amplatzer device.
Findings
Late-onset right focal atrial tachycardia can occur after PFO closure with an Amplatzer device.
Radiofrequency ablation at the device scar site successfully terminated the tachycardia with no recurrence.
Device-related arrhythmias can be safely and effectively treated with ablation.
Abstract
Transcatheter closure of patent foramen ovale (PFO) is increasingly performed after cryptogenic stroke, but it may predispose to atrial arrhythmias. We report a rare case of late-onset right focal atrial tachycardia following PFO closure with an Amplatzer septal occluder device. A 76-year-old man with no prior arrhythmia history underwent percutaneous PFO closure with a 25 mm Amplatzer device after a cryptogenic stroke. Three years later, he presented with symptomatic palpitations. Electrocardiography showed a focal atrial tachycardia. Electrophysiologic study and 3D mapping revealed a right atrial tachycardia originating at the site of the Amplatzer device scar. Radiofrequency ablation at this site successfully terminated the tachycardia, with no recurrence during follow-up. This case illustrates the potential for late-onset right atrial tachycardia due to scarring and altered…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
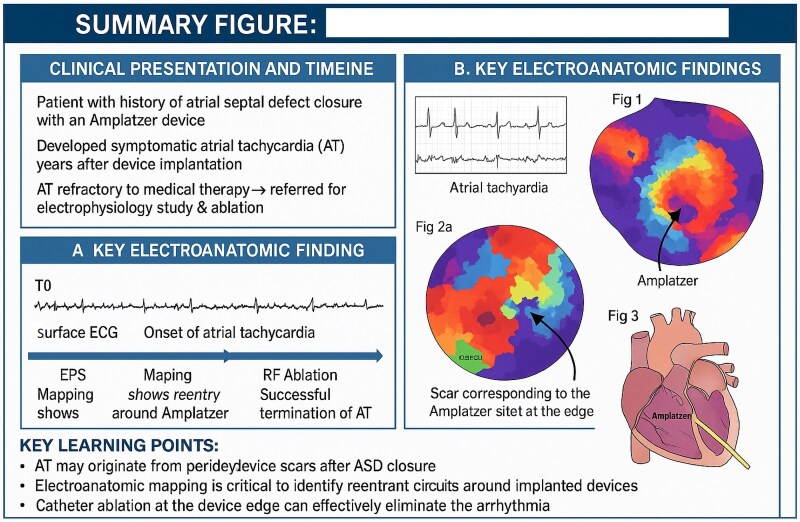 Figure 1
Figure 1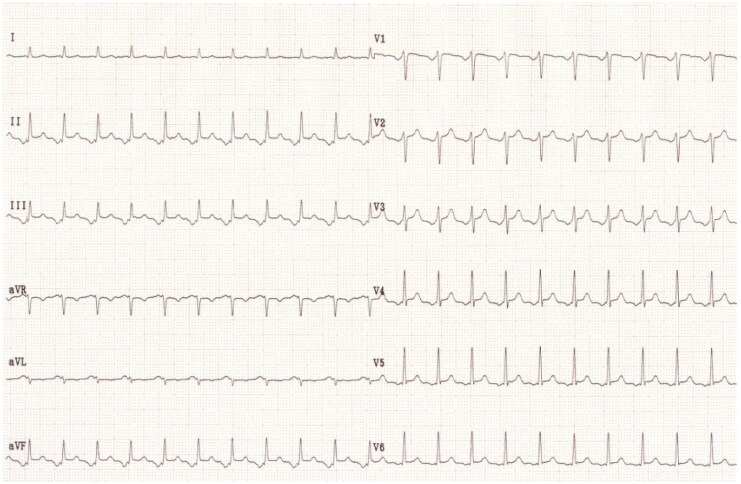 Figure 1
Figure 1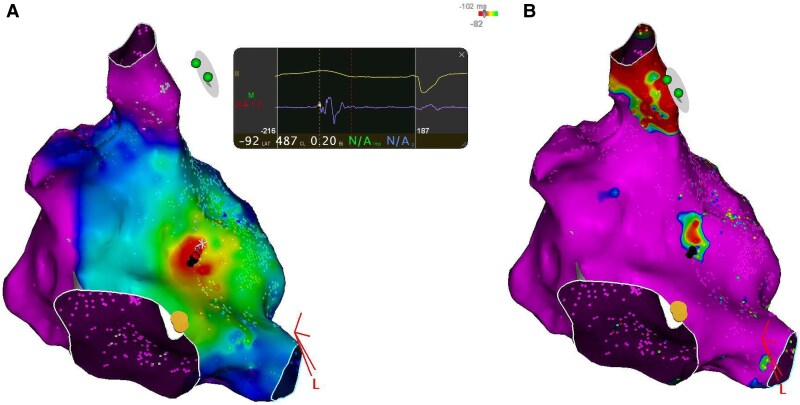 Figure 2
Figure 2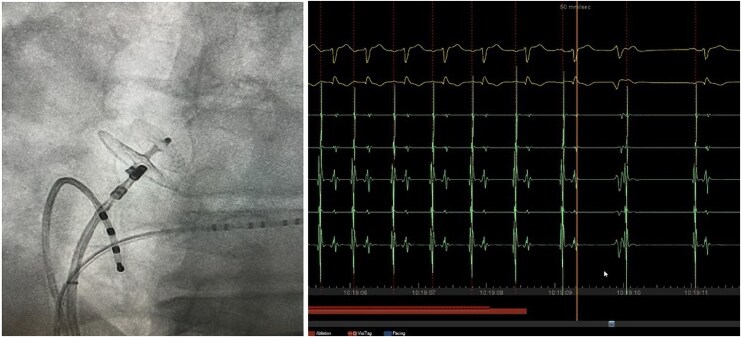 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Atrial Fibrillation Management and Outcomes · Cardiac tumors and thrombi
Introduction
An increasing number of patients have undergone transcatheter device closure of patent foramen ovale (PFO). We report the case of a 76-year-old man who developed right focal atrial tachycardia following PFO closure with an Amplatzer septal occluder device.
Summary figure
**
Case presentation
A 76-year-old man underwent a catheter closure of the PFO with a 25-millimetre Amplatzer septal occluder device after a cryptogenic stroke. The indication for closure was a cryptogenic ischaemic stroke with no other identifiable cause after thorough evaluation. Echocardiography revealed a large right-to-left shunt at rest associated with an atrial septal aneurysm, considered high-risk features for paradoxical embolism. After multidisciplinary discussion, percutaneous PFO closure was proposed to prevent recurrence. There was no history of arrhythmias before the device closure.
Three years later, he presented with symptomatic palpitations, and an electrocardiogram indicated focal atrial tachycardia (Figure 1). Electrophysiologic maneuvers were performed to differentiate the mechanism of supraventricular tachycardia and to exclude alternative diagnoses, including atrioventricular reentrant tachycardia. 3 D Mapping revealed a right atrial tachycardia at the level of the Amplatzer prosthesis (Figure 2) Three-dimensional electroanatomic mapping was performed using the CARTO® 3 system (Biosense Webster, Diamond Bar, CA, USA). At the successful ablation site, the unipolar electrogram showed a QS morphology, consistent with a focal activation pattern. Coronary sinus activation progressing from proximal to distal. Radiofrequency ablation of this focal right atrial tachycardia was successfully performed the earliest activation was recorded 28 ms prior to the onset of the P-wave on surface ECG. Entrainment maneuvers excluded macro-reentry, and the activation map showed a centrifugal pattern consistent with a focal origin. The mechanism was therefore confirmed as focal tachycardia in the electrophysiology laboratory. (Figure 3). No recurrence was observed during follow-up
Surface ECG showing atrial tachycardia.
(A) Activation map demonstrating early depolarization on the right side of the Amplatzer device. (B) Bipolar voltage map showing scar corresponding to the Amplatzer site, with low voltage zones and earliest activation at the edge.
Catheter ablation at the edge of the Amplatzer device successfully terminating atrial tachycardia.
Discussion
PFO closure has been linked to a higher incidence of atrial arrythmia: 6% symptomatic AF in Close study,^1^ and 20% asymptomatic supraventricular tachycardia.^2^
Arrhythmias may be induced by these devices due to atrial scarring and sluggish conduction.^3^
Ablation of Atrial fibrillation on left atrium through Amplatzer has been described.^2^
Zaho reported a case of septal left atrial flutter after implantation of atrial septal occluder.^4^
In this case, the atrial tachycardia emerges from the right septum on the precise site of amplatzer scar which appears on activation map and voltage map (Figure 2A and B).
We hypothesize that the progressive endothelialisation of the septal occluder device could explain the site of microreentry and the 3 years delay of occurrence.
Interestingly a single application could stop the tachycardia which confirm that right septum scar and cicatrization is the exclusive mechanism
To the best of our knowledge, this is the first report of late-onset right atrial tachycardia occurring after PFO closure.
Conclusion
This case highlights the possibility of right atrial tachycardia secondary to device closure of PFO and successful ablation.
Lead author biography
Dr. Ahmed Makni is a cardiologist affiliated with the Centre Hospitalier du Pays d'Aix in Aix-en-Provence, France.
Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. This report was prepared in compliance with the Committee on Publication Ethics guidelines.
Funding: This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mas JL, Derumeaux G, Guillon B, Massardier E, Hosseini H, Mechtouff L, et al Patent foramen ovale closure or anticoagulation vs. antiplatelets after stroke. N Engl J Med 2017;377:1011–1021.28902593 10.1056/NEJ Moa 1705915 · doi ↗ · pubmed ↗
- 2Guedeney P, Laredo M, Zeitouni M, Hauguel-Moreau M, Wallet T, Elegamandji B, et al Supraventricular arrhythmia following patent foramen ovale percutaneous closure. JACC Cardiovasc Interv 2022;15:2315–2322.36008269 10.1016/j.jcin.2022.07.044 · doi ↗ · pubmed ↗
- 3Zaker-Shahrak R, Fuhrer J, Meier B. Transseptal puncture for catheter ablation of atrial fibrillation after device closure of patent foramen ovale. Cathet Cardio Intervent 2008;71:551–552.10.1002/ccd.2136318307237 · doi ↗ · pubmed ↗
- 4Zhao A, Karsenty C, Ladouceur M. Left atrial flutter after implantation of atrial septal occluder. Europace 2018;20:1597.29860385 10.1093/europace/euy 115 · doi ↗ · pubmed ↗