Descriptive study of cholera-related deaths in communities during Zambia’s 2023–2024 outbreak: key insights
Oliver Mweso, Agatha Shula, Cephas Sialubanje, Stephen Longa Chanda, Thelma Shinjeka, Kelvin Mwangilwa, Lusungu Chirwa, Danny Kabwe, Jonathan Mwanza, Nyuma Mbewe, Sombo Fwoloshi, Nyambe Sinyange, Muzala Kapina, Azmach Gebregiorgis, Otipo Shikanga, Moses Mwale, Muyereka Nyirenda

TL;DR
This study analyzed cholera-related deaths in Zambian communities during 2023–2024 to identify key factors contributing to mortality.
Contribution
The study provides new insights into community-level cholera mortality drivers, including gender, age, and comorbidities.
Findings
Most cholera deaths occurred in males aged 35–49 years.
Over half of deaths happened on arrival at healthcare facilities due to delays.
Comorbidities like HIV/AIDS and hypertension were present in 23% of cases.
Abstract
The study sought to understand the characteristics of community deaths due to cholera in Zambia. We sought to examine the drivers of mortality from cholera among communities in Zambia’s 2023–2024 outbreak. This is a descriptive study of the characteristics of community deaths due to cholera in three provinces in Zambia. Routine surveillance data collected between 14 October 2023 and 16 April 2024, comprising a national line list of cholera deaths, were used for this study. 178 participants were included in the study and completed it. All community deaths on the line list were eligible for inclusion. This comprised: deceased individuals whose death was associated with cholera or who met the national cholera case definition (suspected or confirmed); death occurring in the community, en route or on arrival to a health facility prior to admission; and death must have occurred between 14…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
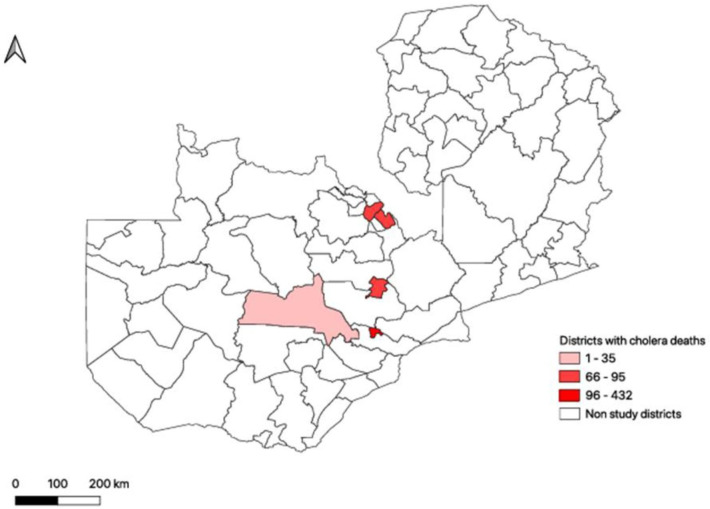 Figure 1
Figure 1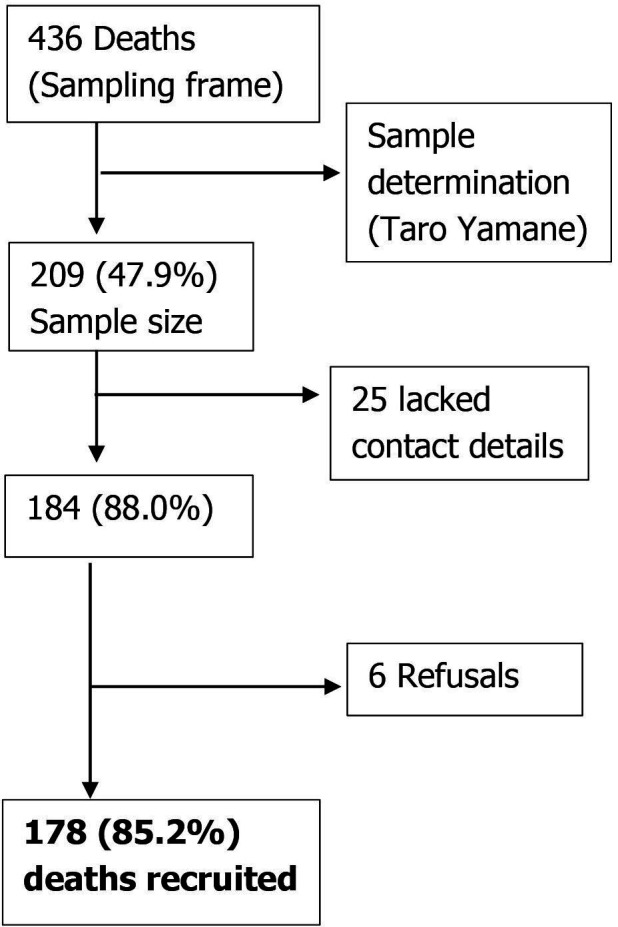 Figure 2
Figure 2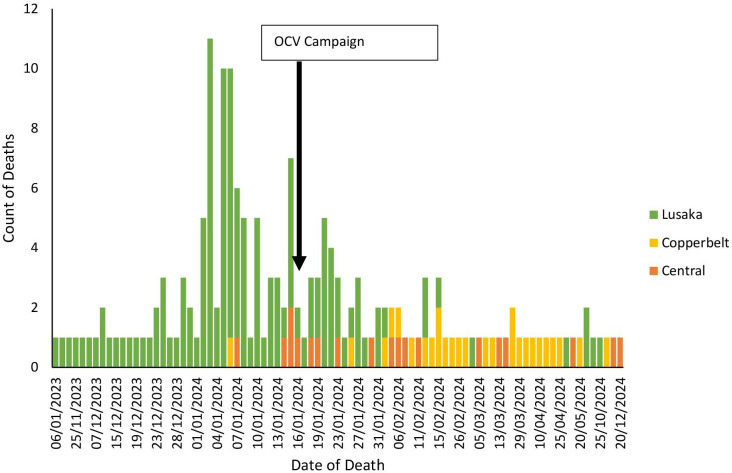 Figure 3
Figure 3| Characteristic | N | % |
|---|---|---|
| Age group (years) | ||
| 0–4 | 29 | 16.3 |
| 5–14 | 23 | 12.9 |
| 15–24 | 13 | 7.3 |
| 25–34 | 36 | 20.2 |
| 35–49 | 40 | 22.5 |
| ≥50 | 37 | 20.8 |
| Sex | ||
| Male | 110 | 61.8 |
| Female | 68 | 38.2 |
| Educational status | ||
| No formal education | 44 | 24.7 |
| Primary education | 68 | 38.2 |
| Secondary education | 52 | 29.2 |
| Tertiary education | 7 | 3.9 |
| Don't know | 7 | 3.9 |
| Marital status | ||
| Single | 86 | 48.3 |
| Married/cohabiting | 62 | 34.8 |
| Widowed | 16 | 9.0 |
| Divorced | 10 | 5.6 |
| Separated | 4 | 2.2 |
| Family monthly income | ||
| 0–99 Kwacha | 63 | 35.4 |
| 100–499 Kwacha | 33 | 18.5 |
| 500–999 Kwacha | 39 | 21.9 |
| 1000–4999 Kwacha | 39 | 21.9 |
| 5000–10 000 Kwacha | 1 | 0.6 |
| Prefer not to say | 3 | 1.7 |
| Household size | ||
| 1 | 7 | 3.9 |
| 2 | 25 | 14.0 |
| 3 | 17 | 9.6 |
| 4 | 33 | 18.5 |
| 5 | 33 | 18.5 |
| 6 | 15 | 8.4 |
| 7 | 25 | 14.0 |
| 8 | 8 | 4.5 |
| >8 | 15 | 8.4 |
| Characteristic | N | % |
|---|---|---|
| Place of death | ||
| Upon arrival at health facility | 91 | 51.1 |
| Home | 52 | 29.2 |
| In Transit (home to facility) | 14 | 7.9 |
| Other (specify) | 13 | 7.3 |
| In Transit (facility to facility) | 6 | 3.4 |
| Relatives' home | 2 | 1.1 |
| Time of death | ||
| Morning | 83 | 46.6 |
| Night | 35 | 19.7 |
| Afternoon | 32 | 18.0 |
| Evening | 26 | 14.6 |
| Unknown | 2 | 1.1 |
| Symptoms reported | ||
| Vomiting | 161 | 90.6 |
| Leg cramps | 85 | 47.8 |
| Fever | 78 | 43.8 |
| Headache | 48 | 27.0 |
| Comorbid conditions | ||
| None | 127 | 71.3 |
| Yes | 41 | 23.0 |
| Don't know | 10 | 5.6 |
| Types of comorbidities (n=41) | ||
| HIV/AIDS | 14 | 34.2 |
| Hypertension | 9 | 22.0 |
| Others (specify) | 8 | 19.5 |
| Diabetes mellitus | 3 | 7.3 |
| Heart disease | 2 | 4.9 |
| Malaria | 2 | 4.9 |
| Tuberculosis | 2 | 4.9 |
| Hypertension and HIV/AIDS | 1 | 2.4 |
| Alcohol consumption | ||
| Yes | 76 | 42.7 |
| No | 102 | 57.3 |
| Consuming alcohol vs stopped consuming alcohol (n=76) | ||
| Yes | 43 | 56.6 |
| No | 23 | 30.2 |
| Don’t know | 10 | 13.2 |
| Alcohol withdrawal vs no alcohol withdrawal (n=43) | ||
| Yes | 14 | 32.6 |
| No | 29 | 67.4 |
| Characteristic | N | % |
|---|---|---|
| Vaccinated in 2021 OCV Campaign | ||
| Yes | 27 | 15.2 |
| No | 116 | 65.2 |
| Don't know | 35 | 19.6 |
| Vaccinated in 2024 OCV Campaign | ||
| Yes | 13 | 7.3 |
| No | 153 | 86.0 |
| Don't know | 12 | 6.7 |
| Sought care for AWD | ||
| Yes | 117 | 65.7 |
| No | 60 | 33.7 |
| Don't know | 1 | 0.6 |
| Considerations before seeking care (n=230 responses) | ||
| No issues | 37.7 | |
| Financial constraints to support care | 27.0 | |
| Lack of/difficulties accessing transport | 19.7 | |
| Lack of family support | 7.6 | |
| Fear of outcome at the facility | 2.4 | |
| Stigma by the community for having Cholera | 2.8 | |
| Lack of awareness of AWD risks | 2.8 | |
| Lack of community support | 1.0 | |
| Time to seek care (n=117) | ||
| Less than 30 min | 6 | 5.1 |
| 30 min to 1 hour | 15 | 12.8 |
| 1 to 6 hours | 42 | 35.9 |
| 6 to 24 hours | 41 | 35.0 |
| 24 to 48 hours | 8 | 6.8 |
| 2 to 5 days | 5 | 4.3 |
| First point of care (n=117) | ||
| Primary health facility | 60 | 51.3 |
| First-level hospital | 47 | 40.2 |
| Retail pharmacy | 3 | 2.6 |
| Oral rehydration point | 2 | 1.7 |
| Private facility | 2 | 1.7 |
| Other | 1 | 0.9 |
| None | 2 | 1.7 |
| Received oral rehydration solution (ORS) at home | ||
| Yes | 75 | 42.13% |
| No | 100 | 56.18% |
| Don’t know | 3 | 1.69% |
| How long did it take to initiate ORS? (n=75) | ||
| Within 30 min to 6 hours | 58 | 37.91% |
| 6 hours to 12 hours | 25 | 16.34% |
| 12 hours to 1 day | 7 | 4.58% |
| More than 2 days | 2 | 1.31% |
| 1 day to 2 days | 5 | 3.27% |
| Don’t know | 56 | 36.60% |
| Characteristic | N | % |
|---|---|---|
| Transport modality | ||
| Private vehicle | 33 | 28.2 |
| Walking | 21 | 17.9 |
| Public vehicle | 13 | 11.1 |
| Ambulance | 5 | 4.3 |
| Wheelbarrow | 2 | 1.7 |
| Not reported | 43 | 36.8 |
| Medication taken | ||
| Yes | 35 | 19.7 |
| No | 132 | 74.2 |
| Don’t know | 11 | 6.2 |
| Type of medication (n=35) | ||
| Antibiotics | 12 | 34.3 |
| Painkillers | 9 | 25.7 |
| Antibiotics and painkillers | 4 | 11.4 |
| Other (specify) | 4 | 11.4 |
| Don't know | 4 | 11.4 |
| Painkillers and others | 1 | 2.9 |
| Traditional medication | 1 | 2.9 |
- —http://dx.doi.org/10.13039/100009099Irish Aid
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVibrio bacteria research studies · Blood donation and transfusion practices · Child Nutrition and Water Access
Introduction
Cholera is an acute watery diarrhoeal (AWD) disease caused by ingestion of food or water contaminated with the toxigenic strains of Vibrio cholerae serogroups O1 or O139.1 Clinical disease is characterised by acute non-bloody watery diarrhoea, severe dehydration and may be accompanied by vomiting.1 2 It affects both children and adults and can cause death within hours if left untreated.2 Access to safe water, improved sanitation, hygiene promotion, timely and appropriate clinical case management, and oral cholera vaccines (OCVs) are some of the effective control strategies.2 Treatment involves, among others: administration of oral rehydration solutions (ORSs), intravenous fluids and/or antibiotics depending on the severity of the disease.1 2 The case fatality rate (CFR) for untreated cholera can reach as high as 30%–50%, but with timely rehydration therapy, it can be reduced to as low as 1%.3
Globally, cholera is still a major health challenge with an estimated 2.86 million cases and 95 000 deaths annually.4 Sub-Saharan African countries bear a disproportionate burden.5 Regrettably, the year 2024 witnessed a threatening re-emergence of cholera across the world, with significant outbreaks reported in more than 25 countries. Sub-Saharan Africa recorded the highest number with over 14 countries, including Burundi, Cameroon, Comoros, the Democratic Republic of the Congo, Ethiopia, Kenya, Malawi, Mozambique, Nigeria, South Africa, Tanzania, Uganda, Zambia and Zimbabwe.6
Zambia reported the first cholera outbreak during 1977–1978 with subsequent outbreaks in 1993, 1999, 2003–2004, 2005–2006, 2010, 2017–2018 and 2023–2024.7 The 2023–2024 outbreak was the largest cholera outbreak in history with clinical cases reaching a peak between October 2023 and April 2024.8 9 As of 16April 2024, a total of 22 922 cholera cases and 734 deaths were reported with a CFR of 3.2% and 436 community deaths, three times higher than the WHO’s recommended threshold of less than 1%.10 The majority of the reported deaths occurred in the community. Strikingly, Lusaka district was the most affected province, accounting for approximately 85% of all cholera deaths, 59% of which occurred in the community.9 Similar trends were observed on the Copperbelt and Central provinces. Persistent and continuous outbreaks of cholera have far-reaching adverse outcomes including diversion of developmental funds, ability to access medical care for the affected individual, threatening the economies of affected communities and ultimately contributing to the cycle of poverty.11 12
Given the high incidence of clinical cases and community deaths observed during the outbreak, there is a need to refine public health strategies aimed at averting future outbreaks and reducing community cholera-related mortalities. The present study sought to describe the socioeconomic, environmental and healthcare-related factors associated with the 2023–2024 cholera outbreak. Understanding these factors is crucial for developing policies aimed at protecting at-risk communities against cholera.
Methods
Study design
The study was a descriptive design using mortality data from the 2023–2024 cholera outbreak. We reviewed routine surveillance data from the Ministry of Health (MoH) compiled surveillance line list from 14 October 2023 to 16 April 2024, which included cholera deaths.
Study sites
The study was conducted in Lusaka, Central and Copperbelt Provinces, focusing on districts that reported the highest number of cholera-related community deaths. These districts included Kanyama, Matero, Munali, Mandevu and Chawama subdistricts of Lusaka province; Kabwe and Mumbwa districts of Central province; and Ndola and Kitwe districts of Copperbelt Province. The districts that were targeted for sampling are shown in figure 1.
Location of districts that were targeted for sampling of cholera-related community deaths in Zambia’s 2023–2024 outbreak.
Study population
Study participants included both suspected and confirmed cholera deaths who died in the community, en route or on arrival to a healthcare facility prior to admission, with dates of onset of symptoms or notification between 14 October 2023 and 16 April 2024. The study protocol (available on request) defined suspected cholera death as any deceased person who had AWD (non-bloody liquid stools that may contain mucus) lasting 7 days or less and had at least three or more loose stools within a 24-hour period; whereas, a confirmed cholera death was any deceased person with Vibrio cholerae O1 or O139 strains identified by culture/isoagglutination or PCR test.1 2
Sample size calculation
The study used the MoH surveillance line list as a sampling frame and calculated the sample size using a finite population formula .13 The formula is n=N/(1+Ne^2^), where n is the sample size, N is the population size, and e is the margin of error.
Assuming a 5% margin of error, with a total number of community deaths from the line list (N=436), the estimated minimum sample size of 209 was calculated.
Selection of deaths
A random sampling technique was used to select community deaths that were recorded on the MoH surveillance line list. Selection was done using a random number generator.14 Thereafter, the selected deaths were then followed up in their respective localities based on their contact details provided on the line list.
Inclusion criteria
Must have been on the MoH surveillance line list.Deceased individuals whose death was associated with cholera or who met the national cholera case definition (suspected or confirmed) occurring in the community, en route or on arrival to a health facility prior to admission.Must have died between 14 October 2023 and 16 April 2024.
Exclusion criteria
Deceased individuals whose family members could not be traced or did not consent to participate in the interview.Deceased individuals who did not reside in a cholera outbreak district.
Data collection and analysis
The data collection team comprised health facility surveillance officers, mortality surveillance officers and trained volunteers. Prior to data collection, the team was trained and equipped on the content of the questionnaire, interview techniques, ethical considerations and the use of electronic devices for data collection.
Data were collected using a structured questionnaire (available in the online supplemental materials). The questionnaire comprised various sections and covered demographic information, clinical symptoms, healthcare-seeking behaviours and environmental factors. Data were collected from relatives or close friends of the deceased cases who had known or interacted with the deceased for at least 7 days prior to their death.
To ensure efficient and accurate data entry, data collection was performed electronically using tablets and smartphones equipped with Kobo Collect software.15 Descriptive analyses were performed and presented using frequencies and percentages.
Patient and public involvement
Participants were not involved in the setting of research priorities, defining research questions and outcome measures, providing input into study design and conduct, dissemination of results and evaluation of studies.
Results
Participant recruitment algorithm
A total of 436 community deaths due to cholera were recorded on the national line list. Using a random number generator, 209 deaths were selected as the sample size. Of these, 25 lacked contact details and could not be followed up, while interviews for six deaths were declined by the relatives. Figure 2 shows the recruitment algorithm of the deceased. A comprehensive analysis was conducted on 178 cholera-related community deaths. The findings are presented under the following categories: demographic characteristics, environmental characteristics, clinical characteristics, vaccination and care-seeking behaviour, patterns in care-seeking behaviour, medication and treatment.
Recruitment flow diagram for cholera-related deaths in communities during Zambia’s 2023–2024 outbreak.
Demographic characteristics
The majority of deaths were in Lusaka province, with a peak incidence in early January 2024. The distribution of cholera-related community deaths over time in the Copperbelt and Central province was uniform (figure 3).
Distribution over time of cholera-related deaths among the three provinces in Zambia’s 2023–2024 outbreak. OCV, oral cholera vaccines.
Males accounted for a higher proportion of deaths (61.8%) compared with females (38.2%). The largest proportions of deaths were among individuals aged 35–49 years (22.5%) and 25–34 years (20.2%); 20.8% were aged above 50 years, 16.3% were in the youngest age group (0–4 years) and 7.3% were in the age group 15–24 years. Approximately 38.2% had completed primary education, 29.2% had secondary education, 24.7% had no formal education and 3.9% had tertiary education. Nearly half (48.3%) of the deceased were single, while 34.8% were married or cohabiting. Family monthly income predominantly fell below 500 Kwacha (US3.6) and 18.5% earned between 100 and 499 Kwacha (US18). Household sizes varied, with households of four or five members being the most common, each constituting 18.5%. Table 1 shows the demographic and socioeconomic characteristics of the deceased.
Environmental and clinical characteristics
Table 2 presents the environmental context of the deaths, and the clinical symptoms reported. Most deaths occurred on arrival at the healthcare facility prior to admission (51.1%) or at home (29.2%). Death during transit from home to a facility accounted for 7.9%, and 3.4% occurred while transferring between facilities. Most deaths occurred in the morning (46.6%); almost one-fifth (18.0%) occurred during the afternoon. Most (90.6%) cases presented with vomiting. Additional symptoms included leg cramps (52.3%), fever (43.4%) and headache (27.2%). Further, comorbid conditions were reported in 23.0% of cases, with HIV/AIDS being the most common (34.2%), followed by hypertension (22.0%).
Vaccination and care-seeking behaviour
Only 15.2% of participants had been vaccinated during the 2021 OCV campaign, 7.3% had received the 2024 OCV. The majority (65.2%) reported no vaccination history for cholera. Regarding care-seeking behaviour, 65.7% of participants sought care for AWD), while 33.7% did not. Barriers to seeking care included, among others, financial constraints (27.0%), transport difficulties (19.7%), stigma from the community for having cholera (2.8%), lack of awareness of AWD risks (2.8%) and lack of community support (1%). Vaccination status and care-seeking behaviours are summarised in table 3.
Patterns in care-seeking behaviour and medication
Most of the deaths had not received ORS while at home (56.2%), with the majority (37.9%) initiating it within 30 min to 6 hours of symptom onset. Among those who sought care, the majority visited primary health facilities (PHFs) (51.3%) or first-level hospitals (40.2%). Delays in seeking care were notable, with only 5.1% accessing care within 30 min of symptom onset and 35.9% within 1–6 hours. Transportation to healthcare facilities was a challenge, notably en route among those who sought care. Private vehicles were the most used modality (28.2%), followed by walking (17.9%). Use of public vehicles (11.1%) and ambulances (4.3%) was limited. Furthermore, 36.8% of cases did not report a transport modality. Only 19.7% of participants who sought care reported taking medication for AWD, excluding ORS from the analysis. Antibiotics (31.4%) and painkillers (22.9%) were the most common treatments. Details on transportation used to reach health facilities and medication administered are provided in table 4.
Discussion
The findings of this study highlight critical gaps and patterns in cholera-related mortality during the 2023–2024 outbreak in Zambia underscoring the complex challenges of managing cholera in resource-constrained settings. Overall, the study provided insights into demographic trends, environmental factors, clinical characteristics and care-seeking behaviour.
Most cholera-related deaths occurred among males, with the highest mortality observed in the economically active age group. This is consistent with a previous study conducted in Zimbabwe that demonstrated that the male sex was more vulnerable to community cholera death than the female sex.16 It has been postulated that the higher community deaths among males compared with females in Zambia may be associated in general with poor health-seeking behaviour among men.17 This pattern underscores the broader socioeconomic impact of cholera, particularly on households reliant on individuals in this age range for income generation. Furthermore, the proportion of deaths among children under the age of 5 reflects the increased vulnerability of this age group to diarrhoeal diseases, consistent with findings from other cholera-endemic regions.41820 For example, in 2015, Ali* et al* estimated that cholera on average kills 91 000 people annually in endemic countries, with more than half of these being children under the age of 5.4 More recently, a study conducted in Bangladesh demonstrated the critical role of nutritional supplementation for children in the face of a cholera outbreak as malnourished children had fatal outcomes.20 This finding is in line with the present study which has shown that most cholera-related deaths were reported from households with smaller incomes. This highlights the importance of the relationship between nutrition and childhood mortalities.21 22 In contrast, limited educational attainment among the deceased, with having no formal education, may reflect a lack of awareness and understanding of the importance of adhering to preventive measures and the importance of seeking early care.17 23 The distribution of deaths across larger households, particularly those with five or more members, which make up over 45% of cases, raises concern about the potential for intrahousehold transmission and clusters of fatalities within families during the outbreak. These findings underscore the importance of targeted household-level interventions, including health education, rapid response teams and preventive measures (eg, household disinfection and contact vaccination) to break chains of transmission and prevent multiple deaths within the same family unit.11 12
The high proportion of deaths occurring at healthcare facilities on arrival suggests critical delays in both care-seeking and transport processes. This points to the patients either hesitating to seek medical care or encountering challenges in getting emergency transport services to a medical facility, resulting in undesired health outcomes, including death.24 25 Poor health-seeking behaviour could have been as a result of the cholera patients attempting to self-medicate or seek help away from conventional facilities as observed in other studies.26 27 Moreover, nearly 30% of deaths occurred at home. This further highlights the barriers to accessing healthcare services, including small household incomes, transportation challenges and the stigma associated with cholera.28 29 A substantial proportion of the deceased (over 60%) sought care at PHFs, indicating a general recognition within communities of the need for medical attention. However, the high proportion of deaths, despite contact with health services, further highlights potential challenges in both access to and quality of care.28 29
One plausible explanation is the severity of illness at presentation. Delays in seeking care due to financial constraints, lack of transport or low risk perception may have led patients to arrive at facilities in critical condition, with advanced dehydration or hypovolaemic shock, thus limiting the effectiveness of available interventions.8 24 27 Additionally, nearly 38% of patients received ORS within 6 hours of symptom onset, while 31% were administered antibiotics, pointing to variability in the timeliness and completeness of clinical response.
Importantly, these outcomes must also be interpreted in the context of health system strain. The large-scale nature of the outbreak likely overwhelmed PHFs, leading to bottlenecks in service delivery. Limited staffing, supply shortages, high patient volumes and logistical constraints may have impaired the system’s ability to provide rapid, standardised cholera care. Even when clinical protocols exist, their execution can falter under pressure, particularly in resource-limited settings.9 27
In addition, morning was the most common time of death, potentially reflecting the accumulation of untreated symptoms overnight, which could be addressed by strengthening community systems to access health services such as transport facilities and oral rehydration points (ORPs) which should be operated on a 24-hour basis.24 30 The delays in health-seeking likely contributed to the observed high mortality rates. Cholera requires rapid rehydration therapy to prevent fatal outcomes.1 Reliance on private vehicles and walking further highlights the limited availability of emergency transport services to resource-limited households. Promotion of the availability of emergency transport services within the community could mitigate these delays in care-seeking and response times.28 30
With regard to the clinical presentation of cholera, atypical symptoms including leg cramps, fever and headache were reported. This is in line with a study conducted by Mutale et al that reported atypical symptoms of cholera among the decedents they studied.17 The authors observed vulnerability of comorbidities including HIV/AIDS and hypertension to death, highlighting the health risks faced by individuals with pre-existing conditions during cholera outbreaks. This is in line with a recent study that established that patients with pre-existing conditions such as HIV and TB were more vulnerable to cholera and had poor outcomes.8 This finding emphasises the need for targeted interventions to address these vulnerabilities.17 Such interventions could include integrating cholera care into routine health services for people living with chronic illnesses.
Vaccination coverage was alarmingly low among the sample, with only 7.3% of participants vaccinated during the 2024 OCV campaign. The 2024 OCV campaign, conducted only in Lusaka district in January, had limited national coverage, with most cholera-related community deaths occurring before and during the campaign. However, low vaccination coverage reflects missed opportunities for preventive healthcare and suggests a need for established routine vaccinations prior to and during cholera seasons to underserved communities. The finding also highlights the need for focused community-based risk communication and community engagement, awareness campaigns and logistical planning to improve vaccination uptake in high-risk populations.25 30
Delayed health-seeking behaviour has been explored in other infectious disease outbreaks in our setting; hence, remedial factors have wider implications for improving patient outcomes.31 32 Future research could explore best practices to counter systemic barriers to care. These could include reducing distances to the facilities and aiding preference for self-treatments such as ORS in the community and placement of ORPs or Case Area Targeted Interventions to help reduce the number of community deaths. The Global Task Force on Cholera Control (GTFCC) recommends the prioritisation of community-driven approaches in cholera response strategies, as long-term success in reducing cholera’s impact relies on collaboration and effective use of community resources.33 Our study of community deaths during a cholera outbreak builds on the body of knowledge advocating for the decentralisation of care to break systemic barriers to treatment during an outbreak.
Implications for public health
The study’s findings emphasise the need for integrated strategies to address cholera-related mortality. Public health efforts should prioritise:
Strengthening community-based risk communication and community engagement to promote early care-seeking and dispel stigma.Enhancing primary healthcare infrastructure, including the availability of 24-hour services and emergency transport systems.Strengthening both the surge capacity and the routine readiness of front-line health facilities in cholera-prone areas.Enhancing early detection and referral mechanisms, decentralising case management and ensuring prepositioned supplies can reduce preventable mortality.Addressing socioeconomic barriers, such as financial constraints, through subsidies or community-based support systems.Expanding vaccination campaigns and ensuring equitable access to key populations.
Limitations
While this study provides valuable insights, it is limited in its study design as it relied on retrospective data, which may be subject to recall bias. It is not possible to draw causal inference because of the study design. More studies with a prospective and analytical design are needed to draw causal inference.
The original survey sample included 209 individuals identified from the national cholera line list. However, the final analytic sample was reduced to 178 due to operational constraints; specifically, 25 entries lacked adequate contact information to enable follow-up, and 6 individuals declined participation. As these exclusions occurred prior to data collection and were unrelated to participant characteristics or outcomes, the potential for systematic bias is limited. Nevertheless, the absence of follow-up for some cases, particularly those without contact details, could under-represent individuals from marginalised or transient populations who may face greater barriers to care. Given the randomised nature of the original sample, the analytical cohort is still likely to reflect the broader population of interest, though some caution is warranted when generalising findings to all cholera-related deaths during the outbreak.
Conclusions
Our study showed that delayed health-seeking behaviour, systemic barriers to accessing healthcare and low vaccination coverages contributed to the high cholera mortality rates in the 2023–2024 outbreak in Zambia. These findings highlight the crucial need for a multisectoral approach in addressing social determinants of health, improving vaccination coverage, establishing integrated community systems and structures to ease access to healthcare and investing in healthcare infrastructure. By prioritising the highlighted public health interventions and systemic reforms, the country can reduce cholera-related mortality and make communities more resilient against future cholera outbreaks and other public health threats.
Supplementary material
10.1136/bmjopen-2025-102709online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Montero DA Vidal RM Velasco J et al Vibrio cholerae, classification, pathogenesis, immune response, and trends in vaccine development Front Med (Lausanne)202310115575110.3389/fmed.2023.115575137215733 PMC 10196187 · doi ↗ · pubmed ↗
- 2Kanungo S Azman AS Ramamurthy T et al Cholera Lancet 202239914294010.1016/S 0140-6736(22)00330-035397865 · doi ↗ · pubmed ↗
- 3Kuna A Gajewski M Cholera - the new strike of an old foe Int Marit Health 201768163710.5603/IMH.2017.002928952662 · doi ↗ · pubmed ↗
- 4Ali M Nelson AR Lopez AL et al Updated global burden of cholera in endemic countries P Lo S Negl Trop Dis 20159 e 000383210.1371/journal.pntd.000383226043000 PMC 4455997 · doi ↗ · pubmed ↗
- 5Narkevich MI Onischenko GG Lomov JM et al The seventh pandemic of cholera in the USSR, 1961-89Bull World Health Organ 199371189968490982 PMC 2393457 · pubmed ↗
- 6Amisu BO Okesanya OJ Adigun OA et al Cholera resurgence in Africa: assessing progress, challenges, and public health response towards the 2030 global elimination target Infez Med 2024321485610.53854/liim-3202-438827826 PMC 11142410 · doi ↗ · pubmed ↗
- 7Gulumbe BHH Chishimba K Shehu A et al Zambia’s battle against cholera outbreaks and the path to public health resilience: a narrative review J Water Health 20242222577510.2166/wh.2024.09439733354 · doi ↗ · pubmed ↗
- 8Mbewe N Mwangilwa K Tembo J et al Survival analysis of patients with cholera admitted to treatment centres in Lusaka, Zambia Lancet Infect Dis 202424 e 473410.1016/S 1473-3099(24)00361-X 38878786 · doi ↗ · pubmed ↗