A Walk to Remember: Anesthetic Management of a Supercentenarian with Hip Fracture and Review of Literature
Kartik Sonawane, Payal Gursahani, Palanichamy Gurumoorthi, Jagannathan Balavenkatasubramanian

TL;DR
This paper presents the successful anesthetic management of a 111-year-old man undergoing hip fracture surgery and reviews strategies for treating supercentenarians.
Contribution
The paper provides a rare case report and literature review on anesthetic techniques for supercentenarians undergoing surgery.
Findings
A combined spinal-epidural anesthesia with ultra-low-dose bupivacaine was safely used in a 111-year-old patient.
Multimodal pain management and proactive hemodynamic optimization enabled early mobilization and discharge.
The case highlights that age alone should not prevent surgery if guided by physiological assessment and evidence-based techniques.
Abstract
The steadily increasing global life expectancy has led to an unprecedented rise in the number of centenarians and supercentenarians (over 110 years) presenting for surgical procedures. While this demographic shift is a triumph of modern medicine, it also poses unique perioperative challenges. Such populations represent an extreme physiological spectrum, characterized by limited organ reserve, altered pharmacokinetics, and unpredictable responses to anesthetic agents. Yet, they often present with urgent surgical conditions such as hip fractures, where timely intervention is critical to preserve function and independence. The anesthetic management of such patients requires a meticulous, physiology-driven strategy that balances efficacy with safety while facilitating early mobilization to maintain independence. We report the anesthetic management of a 111-year-old man, the oldest trauma…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
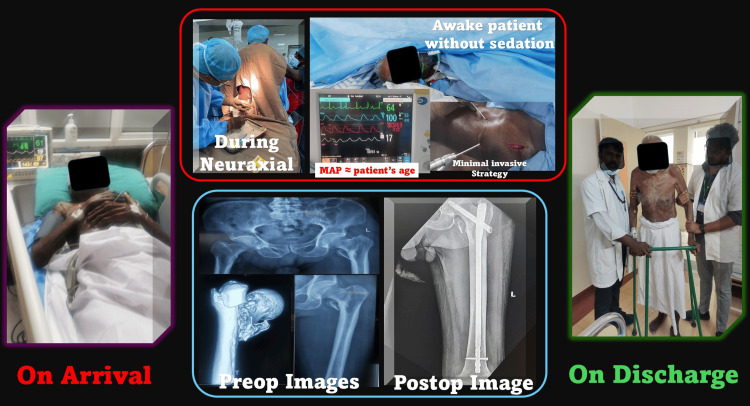 Figure 1
Figure 1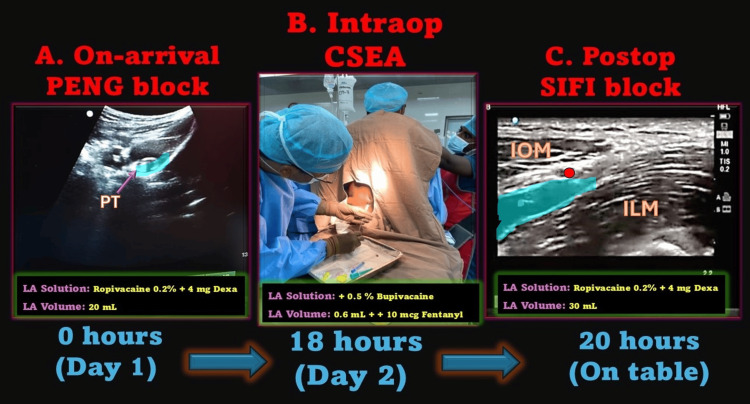 Figure 2
Figure 2| Age Group | Spinal Anesthesia Volume (0.5% Heavy Bupivacaine) | Adjuvants (Optional) | Key Notes |
| <60 years | 2.5-3.0 mL | Fentanyl 20-25 µg or morphine 100-150 µg | Standard dosing, adequate CSF volume, healthy reserve, higher tolerance, and ERAS considerations apply |
| 60-70 years | 2.2-2.5 mL | Fentanyl 15-20 µg | ↓ CSF volume begins with moderate sensitivity, and the dose should be adjusted downward for smaller stature |
| 70-80 years | 1.8-2.2 mL | Fentanyl 10-15 µg | More pronounced CSF volume decline, physiological changes, ↑ cephalad spread risk, and increased hemodynamic variability |
| 80-90 years | 1.2-1.8 mL | Fentanyl ≤10 µg | Very high sensitivity, titrate carefully, and consider CSEA if surgery may be prolonged |
| 90-100 years | 0.8-1.2 mL | Fentanyl ≤10 µg | Maximum caution, ↓ CSF volume, ↓ cardiovascular reserve, safest with CSEA/CSA for titration, and exaggerated sensitivity to LAs |
| 100-110 years | 0.6-0.8 mL | Fentanyl ≤10 µg | Ultra-low dosing is essential, and CSEA/CSA for supplementation is recommended |
| >110 years | 0.4-0.6 mL | Fentanyl ≤10 µg | Supercentenarians require extreme titration, with proactive vasopressor infusion mandatory |
| Step | Protocol Element | Details/Our Practice |
| 1. On-arrival analgesia | Peripheral nerve block | USG-guided PENG block with 20 mL 0.25% ropivacaine → pain relief, positioning, and ↓ opioid use |
| 2. Preoperative preparation | Focused optimization | Minimal but targeted laboratory tests, hydration correction, and HDU monitoring; avoid unnecessary delays |
| 3. Choice of neuraxial anesthesia | Combined spinal-epidural (preferred) | Intrathecal doses of 0.6-1.0 mL of 0.5% heavy bupivacaine (age-stratified); epidural catheter for titration |
| Continuous spinal (alternative) | Microcatheter with fractionated dosing (0.2-0.4 mL increments) and precise titration in frail/high-risk patients | |
| Epidural alone (selective) | If spinal is contraindicated, slow titration, mainly for analgesic role | |
| 4. Hemodynamic management | Vasopressor strategy | Prophylactic norepinephrine infusion (1-2 mL/hour; 8 mg/50 mL dilution) started at spinal injection; avoid fluid overload |
| 5. Intraoperative analgesia | Epidural supplementation | Incremental 3-5 mL 0.25% bupivacaine/lignocaine as required |
| 6. Postoperative analgesia | Regional blocks | SIFI block with 25-30 mL 0.25% ropivacaine; no opioids used |
| 7. ERAS principles | Early recovery strategy | Active warming, multimodal non-opioid analgesia, physiotherapy from POD 2-3, and ambulation by POD 3 |
| 8. Discharge plan | Enhanced recovery | Target discharge at POD 5-7; follow-up for functional independence |
| System | Age-Related Changes | Impact on Neuraxial Anesthesia | Clinical Implications/Modifications |
| Central nervous system | ↓ Neuronal reserve, ↑ sensitivity to local anesthetics, ↓ CSF volume, and altered CSF dynamics | Greater cephalad spread of intrathecal drugs and ↑ risk of high spinal | Use lower intrathecal doses (0.6-1.0 mL of heavy bupivacaine), favoring titratable techniques (CSEA and CSA) |
| Spinal anatomy | Spinal stenosis, calcification, scoliosis, and ↓ intervertebral space | Technical difficulty with needle placement and unpredictable spread | Use ultrasound guidance when needed and consider CSEA/CSA to titrate |
| Cardiovascular | Arterial stiffness, ↓ baroreceptor sensitivity, diastolic dysfunction, and ↓ β-receptor responsiveness | Severe hypotension after sympathectomy and poor compensation | Initiate prophylactic norepinephrine infusion, restrict fluids, and maintain MAP near baseline |
| Respiratory | ↓ Elastic recoil, ↓ vital capacity, ↑ closing volume, and ↑ risk of atelectasis | Reduced reserve for sedation or GA and prone to hypoxemia if oversedated | Prefer RA over GA, avoid deep sedation, and use opioid-sparing analgesia |
| Renal | ↓ GFR, ↓ renal perfusion, and altered drug clearance | Prolonged action of anesthetics and opioids | Avoid nephrotoxic drugs, titrate doses, and maintain renal perfusion with stable MAP |
| Hepatic | ↓ Hepatic mass and blood flow and ↓ phase I metabolism | Reduced clearance of amide local anesthetics and sedatives | Reduce cumulative dosing and avoid long-acting systemic sedatives |
| Musculoskeletal | Osteoporosis and fragile positioning | Pain during neuraxial positioning | Use pre-procedural nerve blocks (e.g., PENG) to aid positioning |
| Cognitive | Baseline cognitive decline and vulnerability to delirium | Risk of postoperative cognitive dysfunction (POCD) and delirium | Avoid benzodiazepines, minimize opioids, and prefer RA + multimodal non-opioid analgesia |
| Thermoregulatory | ↓ Shivering threshold and ↓ temperature control | Increased hypothermia risk intraoperatively | Use active warming to maintain normothermia and prevent complications |
| Age Group | Study/Author (Year) | Anesthesia Type(s) Compared | Key Findings |
| Octogenarians (80-89) | Koval et al. (1999) [ | Spinal versus GA | No difference in one-year mortality (~25%) or morbidity, as noted in an older study |
| Errando et al. (2014) [ | Low-dose spinal | Ultra-low dose (1.5-2 mL bupivacaine) is effective with minimal hypotension; safe for frail elderly | |
| Van Waesberghe et al. (2017) [ | Neuraxial anesthesia (NA) versus GA | NA is associated with lower thromboembolism and shorter hospital stays, as shown in a meta-analysis of over 20 studies | |
| Brox et al. (2016) [ | NA versus GA | Similar mortality; no specific recommendation for type | |
| Kowark et al. (2019) [ | Spinal versus GA | NA reduced postoperative complications (e.g., pneumonia) by 20% in a cohort of >10,000 patients | |
| Neuman et al. (2021) [ | Spinal versus GA | No superiority of spinal over GA for survival or delirium, similar 60-day mortality (~8%), and cognitive outcomes | |
| Cheung et al. (2023) [ | Neuraxial versus GA | NA reduced pulmonary complications and mortality (OR: 0.75); improved recovery in a large meta-analysis of RCTs | |
| Chowdary et al. (2023) [ | Spinal versus GA | NA linked to fewer postoperative complications (e.g., infections), retrospective cohort | |
| Sameer et al. (2023) [ | Multimodal RA + ERAS | ERAS with RA reduced the length of stay by two days and mortality by 15%, in a prospective cohort | |
| Noji et al. (2024) [ | Spinal versus GA | No difference in psoas muscle loss postoperatively; both are safe | |
| Li et al. (2025) [ | GA versus RA | RA improved pain control and reduced opioids in a cohort study | |
| Nonagenarians (90-99) | Döhler et al. (1999) [ | CSA in high-comorbidity elderly | Safe in 154 cases is >80, low complication rate with titration |
| Minville et al. (2006) [ | Low-dose spinal versus CSA | CSA superior for titration, reduced hypotension, and RCT in the elderly is >80 | |
| Rabinowitz et al. (2007) [ | Paramedian versus midline approaches of CSA | Paramedian CSA is associated with an increased success rate | |
| Minville et al. (2008) [ | Three techniques (including NA/GA) | NA minimized hypotension versus GA and elderly femoral neck fractures | |
| Acharya et al. (2022) [ | Peripheral blocks + NA | Effective in a nonagenarian with coagulopathy; case report | |
| Wang et al. (2022) [ | Surgical fixation outcomes | RA is preferred for reduced mortality in nonagenarians | |
| Fan et al. (2024) [ | GA versus spinal | No difference in delirium incidence, meta-analysis | |
| Centenarians (100-109) | Imbelloni et al. (2014) [ | NA for hip surgery | Successful in a 107-year-old; low-dose spinal safe |
| Cevik (2016) [ | Spinal with 8 mg LA | The 90-minute surgery without hemodynamic incompetence resulted in stable outcomes | |
| Dick et al. (2017) [ | Various (mostly RA) | RA safe; improved care in the database era but high mortality (~40%) | |
| Beathe and Memtsoudis (2020) [ | Spinal with 2.5 mL LA | COVID-19-positive with stable hemodynamics with no postoperative complications | |
| Irianto et al. (2021) [ | Regional (epidural) for hemiarthroplasty | Successful in a 100-year-old with fractures and stable outcomes | |
| Ledford et al. (2021) [ | Adjunct VR + NA | Safe in centenarian hip arthroplasty and reduced sedation needs | |
| Abelleyra et al. (2023) [ | Various (RA preferred) | RA associated with better functional recovery; systematic review and meta-analysis | |
| Jang et al. (2023) [ | Cohort study | RA reduced mortality risk factors in multicenter data | |
| Supercentenarians (≥110) | Tosun et al. (2015) [ | Unilateral spinal | Successful in supercentenarian, ultra-low dose |
| Sharma et al. (2020) [ | Small gut obstruction for emergency laparoscopy | Short-acting anesthetic drugs in titrated quantities, better and faster recovery | |
| Wu et al. (2020) [ | RA for arthroplasty | Walked out postoperatively at 111; emphasizes RA feasibility |
| Technique | Drug and Dose | Rationale | Clinical Notes |
| Single-shot spinal anesthesia | 0.6-1.0 mL of 0.5% heavy bupivacaine (with/without opioid adjuvant such as fentanyl 10-15 µg) | Reduced CSF volume in elderly → ↑ cephalad spread; avoids high spinal | Use the lower end (0.6-0.8 mL) in centenarians/supercentenarians/frail ASA IV-V; the higher end (~1.0 mL) for robust elderly |
| Combined spinal-epidural anesthesia (CSEA) | Intrathecal: 0.6-0.8 mL of 0.5% heavy bupivacaine + epidural catheter for titration with 3-5 mL 0.25% bupivacaine/lignocaine as needed | Provides rapid onset with a safety net of epidural supplementation | Preferred in centenarians; allows tailored duration and hemodynamic stability |
| Continuous spinal anesthesia (CSA) | Initial 0.2-0.4 mL of 0.5% isobaric/low-dose heavy bupivacaine; repeat 0.2-0.3 mL increments every 15-20 minutes via microcatheter | Fine titration → hemodynamic stability and prolonged anesthesia | Useful for frail/high-risk elderly and prolonged or unpredictable surgery |
| Epidural alone | 3-5 mL aliquots of 0.25% bupivacaine/lidocaine every 10-15 minutes until the desired level | Slow onset and titratable block | Reserved when spinal is contraindicated (e.g., anticoagulation and severe spinal deformity) |
| Adjuvants (optional) | Fentanyl 10-15 µg intrathecal or dexmedetomidine 5-10 µg epidural | Enhances block quality and prolongs analgesia | Use cautiously; avoid systemic opioids; minimize sedation |
| Parameter | General Anesthesia (GA) | Neuraxial Anesthesia (NA) | GA + Regional Blocks (Hybrid) | Clinical Take-Home |
| Airway and respiratory | Requires airway instrumentation; ↑ risk of aspiration, pneumonia, and atelectasis | Preserves spontaneous breathing; avoids airway manipulation | Airway secured but blocks reduce opioid need → partial respiratory protection | NA safest; GA + RA better than GA alone |
| Hemodynamics | Induction → myocardial depression and vasodilation; fluctuations common | Sympathectomy-induced hypotension; manageable with low-dose NA + vasopressors | GA effects + reduced surgical stress from blocks; still less stable than NA alone | Proactive vasopressor support is crucial |
| Cognition (delirium/POCD) | Higher risk due to sedatives, opioids, and polypharmacy | Lower risk if opioid/benzodiazepine sparing | Reduced opioids versus GA alone but GA-related delirium risk persists | NA superior; GA + RA intermediate |
| Analgesia | Systemic opioids required; short duration | Provides surgical anesthesia + extended analgesia (especially CSEA/CSA + PNBs) | Blocks (PENG/SIFI) provide strong postoperative analgesia; opioid-sparing | NA and GA + RA > GA alone |
| Mobility and ERAS | Delayed mobilization due to opioids and sedation | Facilitates early mobilization; aligns with ERAS | Blocks support early mobility despite GA use | NA most ERAS-friendly; GA + RA acceptable alternative |
| Technical aspects | Widely familiar; fast induction | Technically demanding in scoliosis/calcified spine | Combines the familiarity of GA with the analgesic benefits of blocks | GA + RA is the “middle ground” where NA is not feasible |
| Complications | Aspiration, pneumonia, and myocardial ischemia | Hypotension, rare PDPH, and high spinal with overdose | GA-related complications + rare block-related risks | NA has fewer complications overall |
| Mortality and outcomes | Similar 30-day mortality but ↑ morbidity and delayed functional recovery | Better functional outcomes and lower morbidity | Comparable to NA in pain outcomes; not superior in cognition or pulmonary | Functionally: NA > GA + RA > GA |
| Phase | Intervention | Details | Rationale/Reference |
| Preoperative | Multidisciplinary assessment | Frailty scoring (e.g., Fried 3/5), optimize nutrition, and correct anemia | Tailored to supercentenarian frailty |
| Intraoperative | Neuraxial anesthesia (CSEA) | Ultra-low dose (0.6 mL 0.5% bupivacaine) and PENG/SIFI blocks | Minimizes hemodynamic instability and opioid use |
| Hemodynamic support | Proactive norepinephrine (0.05 µg/kg/minute) and invasive monitoring | Prevents hypotension and ensures stability | |
| Normothermia maintenance | Forced-air warming (36.5°C-37°C) | Reduces complications | |
| Postoperative | Multimodal analgesia | SIFI block (30 mL 0.2% ropivacaine) and no opioids | Preserves cognition and reduces delirium |
| Early mobilization | Physiotherapy by day 1 and ambulation by day 3 | Enhances recovery and reduces immobility risks | |
| Nutritional support | Early oral intake post-surgery | Addresses malnutrition and supports healing |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Hip and Femur Fractures · Anesthesia and Pain Management
Introduction
The global population is undergoing a profound demographic shift, with centenarians, particularly supercentenarians (aged 110 years or older), emerging as the fastest-growing age group [1]. United Nations projections estimate that by 2050, over 3.7 million individuals will be aged 100 years or older [1]. This longevity is driven by advances in nutrition, vaccination, the control of infectious and chronic diseases, and innovations in surgical and intensive care [2,3]. However, increased life expectancy is accompanied by a rise in age-related conditions such as osteoporosis, frailty, and fragility fractures, posing significant challenges for anesthesiologists in perioperative settings [4,5].
Hip fractures are among the most severe injuries in older adults, associated with the loss of independence, extended hospitalization, and elevated mortality [6,7]. The one-year mortality rate following hip fracture surgery in octogenarians and nonagenarians ranges from 20% to 30%, with even higher risks in centenarians [6,8-10]. Timely surgical fixation, multimodal analgesia (MMA), and early mobilization are crucial for optimizing outcomes; however, anesthetic management is pivotal in determining perioperative success in this vulnerable population [11,12].
Supercentenarians present unique anesthetic challenges due to age-related physiological changes that alter pharmacokinetics and pharmacodynamics [13,14]. Reduced cardiovascular reserve, driven by arterial stiffness and impaired baroreflex sensitivity, limits tolerance to hemodynamic shifts [15,16]. Respiratory function declines with decreased chest wall compliance and vital capacity, increasing risks during sedation or general anesthesia (GA) [17,18]. Impaired renal and hepatic clearance prolongs drug half-lives, heightening toxicity risks [13,19]. The central nervous system’s increased sensitivity to sedatives and local anesthetics necessitates precise dosing to avoid complications [14,20]. These factors demand an ultracautious, physiology-driven, and titratable anesthetic strategy.
Over the past two decades, regional anesthesia (RA) techniques, such as low-dose spinal anesthesia, combined spinal-epidural anesthesia (CSEA), and continuous spinal anesthesia (CSA), have gained prominence for hip fracture surgery in older adults due to their ability to minimize hemodynamic instability [21,22]. When paired with peripheral nerve blocks, such as the fascia iliaca or pericapsular nerve group (PENG) block, these techniques enhance analgesia, reduce opioid use, preserve cognitive function, and support enhanced recovery pathways [23-25]. Although centenarian- and supercentenarian-specific literature is limited to case reports and small series, these consistently affirm the safety and efficacy of titrated, protocol-driven RA [26,27].
We report the successful anesthetic management of a 111-year-old man, the oldest trauma surgery patient at our institution, who underwent closed reduction and internal fixation of an intertrochanteric femur fracture. This case highlights core principles of geriatric anesthesia: individualized dosing, proactive hemodynamic support, opioid-sparing MMA, and adherence to enhanced recovery after surgery (ERAS) protocols. Ultimately, it reflects not just the science of anesthesia but the art of giving a supercentenarian the dignity of mobility, a walk to remember. We also contextualize this experience within a review of the literature to provide educational value and practical insights for clinicians faced with similar scenarios.
Case presentation
Patient presentation
A 111-year-old man presented to our institution’s emergency department following a low-energy fall at home, resulting in an intertrochanteric femur fracture confirmed by X-ray (Figure 1). His medical history included hypertension (controlled with amlodipine 5 mg daily), mild cognitive impairment, and no documented cardiac or pulmonary disease. Preoperative assessment revealed a frail phenotype (Fried frailty score: 3/5) but preserved organ function: blood pressure, 143/69 mmHg; heart rate, 61 beats per minute (bpm); oxygen saturation, 97% on room air; and normal renal (creatinine: 1.0 mg/dL) and hepatic function (normal liver enzymes). Lumbar spine imaging confirmed the preservation of intervertebral spaces, facilitating the option of neuraxial anesthesia. His American Society of Anesthesiologists (ASA) classification was III, and he expressed a strong desire to regain mobility to maintain independence.
Perioperative course of a 111-year-old centenarian undergoing hip fracture fixation under regional anesthesia.The sequence of clinical images depicts the patient’s journey from admission to discharge. On arrival, the patient was monitored and stabilized before surgery. Intraoperative images show the administration of combined spinal-epidural anesthesia with stable hemodynamics, and the patient remained awake without sedation, maintained with a minimal invasive strategy. Preoperative radiographs confirmed an intertrochanteric femur fracture, and postoperative radiographs demonstrated successful fixation with intramedullary nailing. The final image shows the patient mobilized with support at discharge on postoperative day 7, highlighting functional recovery.MAP, mean arterial pressure; Preop, preoperative; Postop, postoperativeSource: this figure was created by the first author, KS.
Given the patient’s age and frailty, a multidisciplinary team comprising an anesthesiologist, orthopedician, geriatrician, and critical care specialist convened to formulate a perioperative strategy. A consensus favored a physiology-driven approach incorporating RA as an adjunct to MMA, titrated neuraxial dosing according to our institutional age-dose protocol (Table 1), supported by a perioperative care pathway that emphasizes proactive hemodynamic monitoring and early mobilization within an ERAS framework.
Preoperative analgesia
Upon arrival, an ultrasound-guided PENG block was performed using 20 mL of 0.2% ropivacaine and 4 mg of dexamethasone (Figure 2A). This block provided immediate and sustained analgesia, obviating systemic opioid use and ensuring pain-free rest overnight. Importantly, it eliminated the need for a “positioning block” before neuraxial anesthesia on the next day, a major advantage in elderly patients with hip fracture, where pain often hinders safe positioning.
Perioperative regional anesthesia strategy in a 111-year-old supercentenarian.(A) On arrival, an ultrasound-guided pericapsular nerve group (PENG) block was performed using 20 mL of 0.2% ropivacaine with 4 mg dexamethasone, providing effective preoperative analgesia. The blue area shows local anesthetic spread under the psoas tendon (PT). (B) Intraoperatively, combined spinal-epidural anesthesia (CSEA) was administered with 0.6 mL of 0.5% hyperbaric bupivacaine and 10 µg fentanyl, achieving adequate surgical anesthesia while maintaining hemodynamic stability. (C) At the conclusion of surgery, a postoperative supra-inguinal fascia iliaca (SIFI) block was performed using 30 mL of 0.2% ropivacaine with 4 mg dexamethasone to ensure prolonged analgesia and facilitate early mobilization. The blue area denotes local anesthetic spread between the internal oblique (IOM) and iliacus muscle (ILM), under the fascia iliaca, located below the deep circumflex iliac artery (shown as a red circle).LA, local anesthetic; Dexa, dexamethasone; Intraop, intraoperative; Postop, postoperativeSource: this figure was created by the first author, KS.
Intraoperative management
Inside the operating room, standard ASA monitoring (electrocardiogram, pulse oximetry, and capnography) was instituted. Invasive arterial blood pressure monitoring was established for beat-to-beat assessment, considering the patient’s extreme age and limited physiological reserve. Ultrasound examination revealed markedly sclerotic arterial walls, a reflection of vascular ageing, yet cannulation was achieved without difficulty. Considering the patient’s extreme age and the nature of surgery, additional measures included the use of a body warmer and fluid warmer to prevent perioperative hypothermia.
CSEA was administered in the sitting position at the L3-L4 interspace, using 0.6 mL of 0.5% hyperbaric bupivacaine and 10 µg of fentanyl intrathecally, followed by epidural catheter placement (Figures 1, 2B). A block height of T12 was achieved, and 30 minutes later, an epidural top-up of 6 mL 0.5% bupivacaine extended surgical anesthesia seamlessly. Hemodynamic stability was proactively maintained with a continuous low-dose norepinephrine infusion (1 mL/hour), titrated to maintain mean arterial pressure (MAP) close to baseline (“MAP ≈ patient’s age” principle) (Figure 1). Invasive arterial monitoring ensured real-time hemodynamic assessment, and forced-air warming maintained normothermia (36.5°C-37°C). Total blood loss was approximately 250 mL, managed with one unit of leukodepleted packed red blood cells and 1 L of crystalloids. Oxygen was delivered at 4 L/minute via a Hudson mask, ensuring adequate oxygenation without the need for intraoperative sedation. Urine output remained satisfactory throughout, reflecting stable renal perfusion.
Postoperative course
At the conclusion of surgery, the epidural catheter was removed, and a supra-inguinal fascia iliaca (SIFI) block was performed using 30 mL of 0.2% ropivacaine with 4 mg dexamethasone to provide extended postoperative analgesia (Figure 2C). The patient was monitored in the high-dependency unit for 24 hours before transfer to the ward. Pain control was excellent without the use of systemic opioids, preserving cognitive clarity and respiratory function. Early physiotherapy was initiated per our institutional ERAS protocol (Table 2). The patient was mobilized with assistance on postoperative day 3. He was discharged home in stable condition on postoperative day 7, marking a successful recovery in one of the oldest trauma patients reported to date. No delirium or complications were noted at 30-day follow-up. Written informed consent was obtained from the patient’s legally authorized representative for the publication of this case report and any accompanying images. Patient anonymity has been preserved, and no identifying information has been disclosed.
Discussion
The anesthetic management of supercentenarians requires a nuanced balance of clinical precision and individualized care. While chronological age is a marker, frailty, physiological reserve, and comorbidities are the primary drivers of perioperative risk [4,5]. Our 111-year-old patient’s preserved organ function enabled an RA-based approach, but the extreme age necessitated a conservative, physiology-driven strategy guided by institutional protocols [2]. Age-related physiological changes, such as altered pharmacokinetics and heightened neural sensitivity, amplify the challenges of anesthesia in supercentenarians (Table 3).
Review of literature
To contextualize our approach, it is important to review the available evidence on anesthesia in the very elderly, including octogenarians, nonagenarians, centenarians, and supercentenarians. The perioperative management of elderly patients undergoing hip fracture surgery has been extensively studied in octogenarians, less so in nonagenarians, and only rarely in centenarians and supercentenarians [10,28]. The literature highlights a progressive shift in anesthetic techniques with advancing age, emphasizing dose reduction, multimodal analgesia (MMA), and proactive hemodynamic support as critical strategies for optimizing outcomes [2,29].
Octogenarians (80-89 Years)
This age group dominates the geriatric anesthesia literature, with large cohort studies and randomized trials showing that neuraxial anesthesia, particularly spinal anesthesia or CSEA, reduces postoperative pulmonary complications, thromboembolism, and mortality compared to GA [7,8,21,30-35]. Intrathecal doses of 1.5-2.0 mL of 0.5% hyperbaric bupivacaine are typically sufficient, providing effective anesthesia while minimizing hemodynamic instability [32]. ERAS protocols, including early mobilization and opioid-sparing analgesia, significantly reduce hospital length of stay and mortality in this cohort [12,36-38]. However, prevalent comorbidities such as heart failure and chronic obstructive pulmonary disease necessitate rigorous preoperative optimization and intraoperative monitoring [10,29]. Moreover, RA improves pain control, reducing opioid requirements compared to GA, thereby decreasing delirium and other opioid-related complications [39].
Nonagenarians (90-99 Years)
Studies in this age group are less abundant, primarily consisting of retrospective series and case reports that confirm the feasibility of RA [5,40]. Ultra-low intrathecal doses (1.0-1.5 mL of 0.5% bupivacaine) and CSA are effective, allowing for the precise titration of block height to minimize hemodynamic fluctuations [22,41-43]. The heightened risk of postoperative delirium in nonagenarians underscores the value of opioid-sparing MMA and early mobilization to preserve cognitive function [9,44-46].
Centenarians (100-109 Years)
Evidence is limited to case reports and small series yet consistently supports RA’s safety [6,26-28,47-51]. A 100-year-old COVID-19-positive patient underwent hip hemiarthroplasty with 2.5 mL of 0.5% preservative-free bupivacaine, maintaining stable hemodynamics without complications [49]. Another had hip fracture surgery with 8 mg (1.6 mL) of 0.5% hyperbaric bupivacaine, achieving stable outcomes and discharge on day 7 [50]. A third 100-year-old received spinal anesthesia with a virtual reality adjunct for hip arthroplasty, avoiding delirium [51]. Combined neuraxial and peripheral nerve block strategies are frequently advocated to reduce systemic drug exposure and enhance recovery [40,52].
Supercentenarians (≥110 Years)
Reports are exceedingly rare but demonstrate RA’s feasibility [53-55]. To date, there are no large series. A supercentenarian received unilateral spinal anesthesia with norepinephrine support for surgery, demonstrating feasibility at extreme age [54]. Another 111-year-old woman underwent hip arthroplasty with low-dose spinal anesthesia [55]. These cases suggest that, with careful protocolization, surgery remains viable even at extreme ages [31,53]. Our case of a 111-year-old trauma patient thus represents one of the very few documented experiences of anesthesia in this demographic.
Summary
Table 4 summarizes key reports across these age groups, demonstrating the consistent safety and efficacy of RA in the very elderly. Across the eighth to eleventh decades, the literature consistently supports the following: (1) RA’s superiority over GA in reducing pulmonary complications, delirium, and recovery time [7,8,21]; (2) the progressive dose reduction of intrathecal bupivacaine, from ~2 mL in octogenarians to <1 mL in centenarians [32,43]; (3) CSA and CSEA’s role in providing hemodynamic stability through titration [22,41]; and (4) peripheral nerve blocks and ERAS protocols’ efficacy in minimizing opioids and enhancing recovery [36,40,45].
Building upon these prior findings, our case demonstrates how these principles can be safely adapted to the supercentenarian population through protocolized, physiology-based perioperative management.
RA versus GA in supercentenarians
Neuraxial anesthesia, particularly CSEA, is consistently reported as the preferred approach for patients over 90 years of age due to its favorable safety profile [5,8]. Compared to GA, RA reduces postoperative delirium, pulmonary complications, and recovery time in centenarians and supercentenarians [21,9]. Studies highlight GA’s association with increased postoperative cognitive dysfunction and prolonged ventilation in the ultra-elderly [30,56]. RA, by contrast, minimizes systemic drug exposure, preserves respiratory function, and facilitates early mobilization [13,21]. Our use of CSEA provided rapid spinal onset and epidural flexibility, accommodating variable surgical durations while maintaining hemodynamic stability [22,42]. Combined with peripheral nerve blocks, this approach underscores RA’s superiority for hip fracture surgery in supercentenarians [40,57].
Ultra-low-dose intrathecal anesthesia: A cornerstone of safety
Neuraxial dosing in supercentenarians requires extreme caution due to reduced cerebrospinal fluid (CSF) volume and increased neural sensitivity, which narrows the therapeutic window [13,2]. Standard doses of 2.5-3.0 mL of 0.5% hyperbaric bupivacaine, used in younger adults, risk profound hypotension or high spinal block [32]. Our decision to use ultra-low intrathecal dosing was consistent with our institutional neuraxial protocol (Table 5), which was specifically designed for the ultra-elderly. Our protocol recommends 0.6 mL for patients over 110 years, as outlined in Table 1. Such age-related progressive dose reduction mitigates risks of cardiovascular collapse [43]. This “less is more” approach prevents catastrophic complications such as profound hypotension or high spinal block. The epidural component of CSEA allowed for intraoperative titration, thereby enhancing safety in this population [22].
Perioperative monitoring and thermal management
Meticulous monitoring is critical in supercentenarian anesthesia [29]. Invasive arterial pressure monitoring enables real-time hemodynamic assessment and proactive vasopressor titration, reducing risks of myocardial ischemia and renal dysfunction, making invasive monitoring a cornerstone of safety rather than a luxury [58,59]. Hypothermia, prevalent due to impaired thermoregulation, exacerbates coagulopathy and delays drug metabolism [60,61]. Forced-air warmers and fluid warmers, used in our case, align with best practices for maintaining normothermia and supporting hemodynamic stability [62,63].
Hemodynamic management: Proactivity over reactivity
Hypotension is the most feared complication of neuraxial anesthesia in centenarians/supercentenarians, potentially causing myocardial ischemia or cerebral hypoperfusion [43,59]. Proactive low-dose norepinephrine infusions, as used in our case, stabilize MAP and reduce delirium risk compared to reactive bolus therapy [64,65]. This approach reflects a shift toward preemptive hemodynamic management in frail patients [66,67]. Low-dose norepinephrine infusion stabilizes mean arterial pressure, preserves cerebral oxygenation, and reduces the incidence of delirium [64,65]. In our case, initiating norepinephrine at induction resulted in a stable intraoperative course with minimal fluctuations. This aligns with the emerging consensus that hemodynamic management in frail elderly patients should shift from “chasing drops in pressure” to “preempting instability.”
Role of peripheral nerve blocks in a multimodal strategy
Peripheral nerve blocks are increasingly recognized as essential adjuncts in the perioperative care of elderly patients with hip fractures [23,24]. By targeting the articular branches of the hip capsule, the PENG block provides profound analgesia with minimal motor involvement, making it superior to traditional femoral or fascia iliaca blocks for positioning and comfort [25]. In our case, the PENG block facilitated pain-free positioning for neuraxial placement and avoided the need for systemic opioids. The SIFI block extended postoperative pain control in our case, reducing opioid use and preserving cognitive function [57]. Meta-analyses confirm that multimodal RA reduces pulmonary complications, thromboembolism, and delirium, all of which are disproportionately fatal in older adults [45,46]. A comparative perspective of GA, RA, and hybrid techniques is summarized in Table 6, underscoring the superiority of regional strategies for pulmonary, cognitive, and recovery outcomes.
Enhanced recovery and functional outcomes
Our patient’s mobilization by postoperative day 3 and discharge by day 7 highlight the efficacy of ERAS protocols [36]. Immobility is a key mortality predictor post-hip fracture, with early ambulation reducing pneumonia, deep vein thrombosis, and sarcopenia while promoting psychological well-being [68,69]. Our ERAS approach, integrating opioid-sparing analgesia, normothermia, and physiotherapy, proved effective even at 111 years [12,37,38]. The efficacy of our supercentenarian-specific ERAS pathway (Table 7), which facilitates early mobilization and discharge, is supported by Zhu et al. (2021), who demonstrated reduced complications and shorter hospital stays in elderly patients with intertrochanteric fractures using an ERAS protocol [70]. This case validates the concept that ERAS principles are not only feasible but indispensable in such age groups.
Comparison with reported cases
Reports on centenarians and supercentenarians are scarce, but they consistently support RA for its safety and efficacy [10,26-28,48,50,52-55]. These reports highlight the role of ultra-low-dose RA in minimizing hemodynamic instability and delirium. Unlike these isolated cases, our comprehensive approach, integrating CSEA, PENG, and SIFI blocks, as well as proactive norepinephrine infusion and ERAS protocols, offers a reproducible template for supercentenarian trauma surgery. Our case, therefore, contributes to the novelty of the field, as it demonstrates how a structured, physiology-based strategy can yield successful outcomes in a supercentenarian trauma patient, providing a template for reproducibility rather than an isolated anecdote.
Broader ethical and clinical implications
A frequently asked question is whether surgery in centenarians/supercentenarians is justified. Critics argue that the risks outweigh the benefits, while proponents emphasize the quality of life and independence [71]. Literature increasingly supports the latter, showing that the surgical fixation of fractures in centenarians offers superior survival, pain control, and functional recovery compared to conservative management [9,47]. Respecting physiology over chronology is key, as it aligns interventions with patient goals [2]. Our patient’s recovery at 111 years demonstrates that protocol-driven anesthesia can restore mobility and the quality of life, challenging age-based biases [55,72]. Our patient’s recovery reinforces a critical principle: chronological age should never be the sole determinant of care.
Strengths and limitations
The major strength of this report lies in its novelty. To our knowledge, this is among the very few documented cases of hip fracture fixation in a supercentenarian above 110 years, managed with a structured, protocol-based perioperative pathway. Unlike most reports that describe isolated anesthetic techniques, this case integrates ultra-low intrathecal dosing, CSEA flexibility, proactive norepinephrine support, and multimodal regional blocks within an ERAS framework. This holistic, physiology-driven approach not only ensured intraoperative stability but also translated into early ambulation and discharge, providing a model of care that is reproducible across centers.
However, certain limitations must be acknowledged. Being a single case report, its findings cannot be generalized across all supercentenarians, who may present with greater frailty or significant comorbidities. Additionally, although outcomes were favorable, long-term follow-up beyond discharge was not available, which limited our ability to comment on sustained functional recovery. Finally, the absence of a comparator group (such as GA or conservative management) precludes definitive conclusions regarding the superiority of one technique over another. Nonetheless, the case highlights practical strategies, educational insights, and institutional protocols that may serve as a valuable reference point for anesthesiologists confronted with similar ultra-elderly patients worldwide.
Conclusions
The successful anesthetic management of a 111-year-old supercentenarian redefines the boundaries of surgical feasibility in extreme age. A physiology-guided, protocol-driven approach, anchored in ultra-low intrathecal dosing, proactive norepinephrine-supported hemodynamic stabilization, and multimodal regional analgesia using PENG and SIFI blocks, ensured intraoperative stability, preserved cognition, and enabled early mobilization. Across literature from octogenarians to supercentenarians, regional anesthesia consistently demonstrates superiority over general anesthesia by reducing pulmonary complications and delirium and promoting functional recovery. This case reinforces that frailty and physiology, not chronology, must guide anesthetic decisions.
Three pillars underpin success in this demographic: titratable neuraxial safety (CSEA/CSA), opioid-free empowerment through peripheral blocks, and motion-driven recovery under ERAS principles. Ultimately, anesthesia for the ultra-elderly transcends survival; it is an art of restoration. This was not merely a procedure but a walk to remember, a testament that, with evidence-based precision and reverence for physiology, even supercentenarians can reclaim independence and dignity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World’s centenarian population projected to grow eightfold by 2050 Published April 21 10 2025 1] A.Geiger 2016 https://www.pewresearch.org/short-reads/2016/04/21/worlds-centenarian-population-projected-to-grow-eightfold-by-2050/
- 2Anaesthetic considerations in nonagenarians and centenarians Curr Opin Anaesthesiol Irwin MG Ip KY Hui YM 7767823220193146469610.1097/ACO.0000000000000793 · doi ↗ · pubmed ↗
- 3Aging biology and geriatric clinical pharmacology Pharmacol Rev Mc Lean AJ Le Couteur DG 1631845620041516992610.1124/pr.56.2.4 · doi ↗ · pubmed ↗
- 4Fragility fractures: risk factors and management in the elderly Medicina (Kaunas) Migliorini F Giorgino R Hildebrand F 11195720213468415610.3390/medicina 57101119 PMC 8538459 · doi ↗ · pubmed ↗
- 5An overview of osteoporosis and frailty in the elderly BMC Musculoskelet Disord Li G Thabane L Papaioannou A Ioannidis G Levine MA Adachi JD 461820172812598210.1186/s 12891-017-1403-x PMC 5270357 · doi ↗ · pubmed ↗
- 6Changing trends in the mortality rate at 1-year post hip fracture - a systematic review World J Orthop Downey C Kelly M Quinlan JF 1661751020193091879910.5312/wjo.v 10.i 3.166PMC 6428998 · doi ↗ · pubmed ↗
- 7Comparative efficacy of neuraxial and general anesthesia for hip fracture surgery: a meta-analysis of randomized clinical trials BMC Anesthesiol Zheng X Tan Y Gao Y Liu Z 1622020203260559110.1186/s 12871-020-01074-y PMC 7325684 · doi ↗ · pubmed ↗
- 8Spinal anesthesia or general anesthesia for hip surgery in older adults N Engl J Med Neuman MD Feng R Carson JL 2025203538520213462378810.1056/NEJ Moa 2113514 · doi ↗ · pubmed ↗