Infective Endocarditis and Antimicrobial Timing: A Case for Delay?
Elisavet Stavropoulou, Bruno Ledergerber, Nicolas Fourré, Virgile Zimmermann, Jana Epprecht, Nicoleta Ianculescu, Pierre Monney, Georgios Tzimas, Michelle Frank, Laurence Senn, Lars Niclauss, Matthias Kirsch, Mathias Van Hemelrijck, Omer Dzemali, Benoit Guery, Barbara Hasse

TL;DR
This study finds that delaying antibiotics in stable patients with suspected heart infection does not worsen outcomes.
Contribution
Shows deferring antimicrobial treatment in stable infective endocarditis patients does not increase mortality.
Findings
No difference in 30-day mortality between immediate and deferred treatment groups.
Deferred treatment did not increase risk of embolic events or new infections in confirmed IE cases.
Abstract
In patients with suspected infective endocarditis (IE), current guidelines recommend prompt initiation of empiric antimicrobial treatment after obtaining blood cultures. However, the clinical benefit of immediate treatment in hemodynamically stable patients remains uncertain. This study assessed the impact of deferring antimicrobial treatment in patients with suspected IE. We conducted a multicenter cohort study of adult patients with bacteremia and clinical suspicion of IE from 2 university hospitals (2015–24). Patients presenting with sepsis, intensive care unit admission, neutropenia, or a clearly identifiably focus other than IE were excluded. All cases were adjudicated by a dedicated Endocarditis Team as either IE or not IE. The primary outcome for all episodes was 30-day mortality; for confirmed IE cases, the composite outcome included 30-day mortality, new embolic events, or new…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
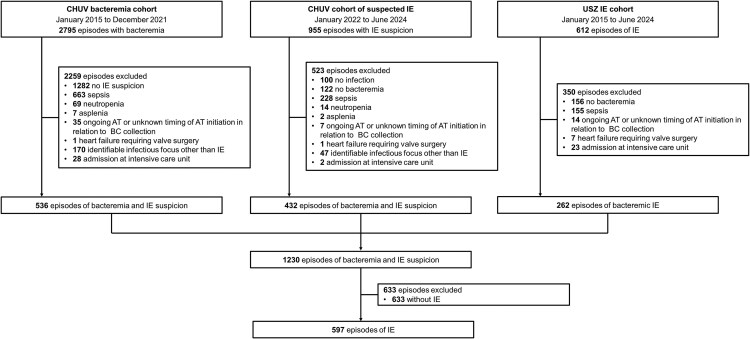 Figure 1
Figure 1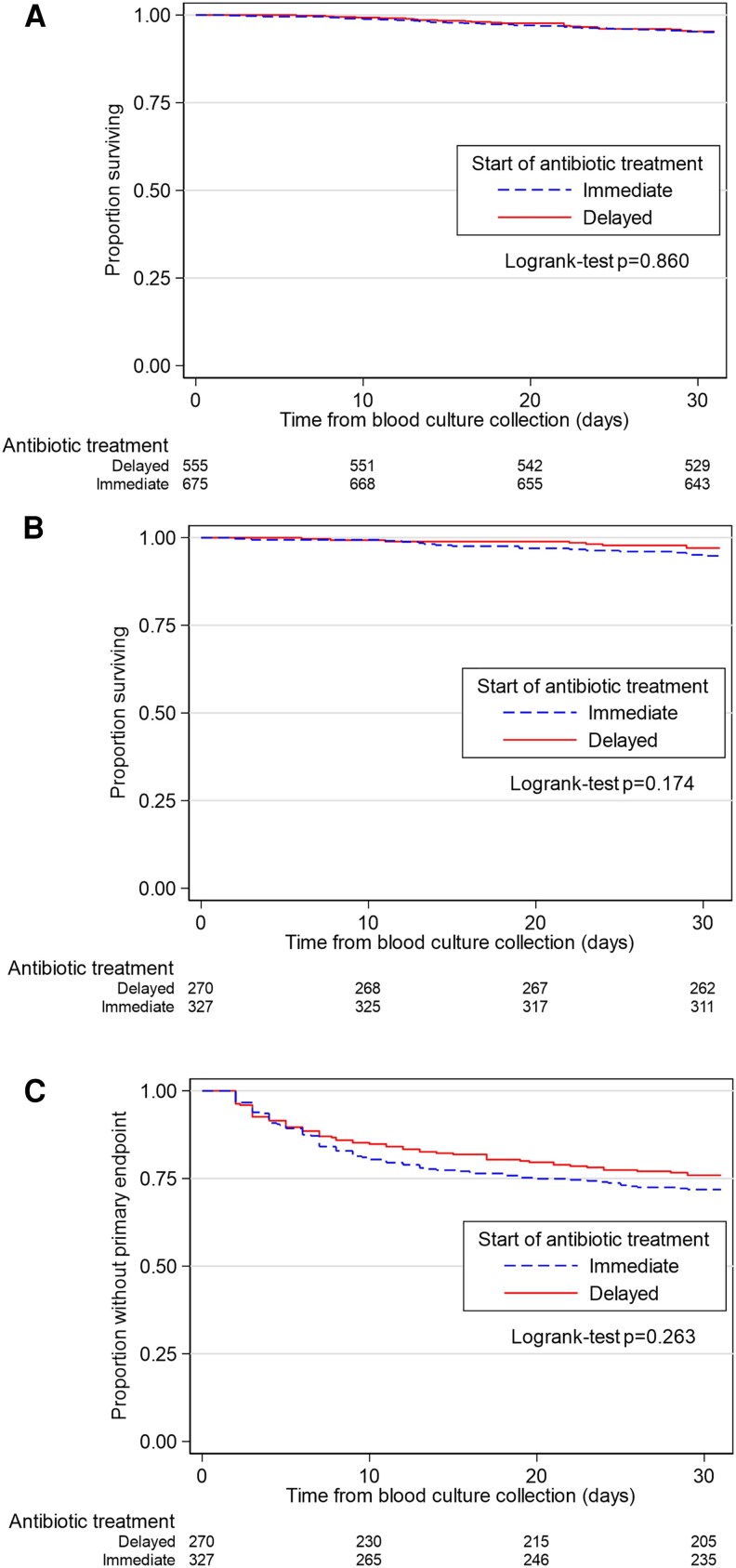 Figure 2
Figure 2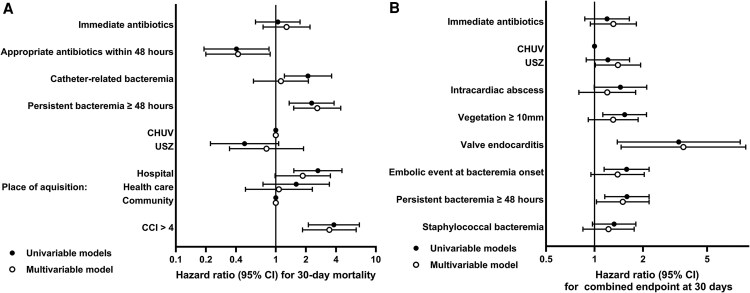 Figure 3
Figure 3| Group D (n = 555) | Group I (n = 675) |
| |
|---|---|---|---|
| Demographics | |||
| Male sex, n (%) | 399 (72) | 481 (71) | .849 |
| Age (years), median (IQR) | 65 (53–76) | 68 (52–78) | .101 |
| Age >60 y, n (%) | 350 (63) | 440 (65) | .473 |
| Co-morbidities | |||
| Diabetes mellitus, n (%) | 122 (22) | 158 (23) | .585 |
| Obesity (body mass index ≥30 kg/m2), n (%) | 99 (18) | 137 (20) | .308 |
| Chronic kidney disease (moderate or severe), n (%) | 130 (23) | 173 (26) | .388 |
| Malignancy (solid organ or hematologic), n (%) | 98 (18) | 111 (16) | .594 |
| Immunosuppression, n (%) | 67 (12) | 83 (12) | .930 |
| Chronic obstructive pulmonary disease, n (%) | 67 (12) | 68 (10) | .273 |
| Cirrhosis, n (%) | 65 (12) | 68 (10) | .358 |
| Congestive heart failure, n (%) | 79 (14) | 70 (10) | .043 |
| Intravenous drug use, n (%) | 53 (10) | 42 (6) | .032 |
| Prior infective endocarditis, n (%) | 42 (8) | 45 (7) | .577 |
| Surgical prosthetic valve or TAVI, n (%) | 95 (17) | 119 (18) | .821 |
| Cardiac implantable electronic device, n (%) | 72 (13) | 93 (14) | .737 |
| Charlson Comorbidity Index (points), median (IQR) | 4 (1–6) | 4 (1–6) | .101 |
| Charlson Comorbidity Index >4 points, n (%) | 238 (43) | 305 (45) | .420 |
| Hospital | .001 | ||
| Lausanne University Hospital, n (%) | 412 (74) | 555 (82) | |
| University Hospital Zurich, n (%) | 143 (26) | 120 (18) | |
| Setting of bacteremia onset | .036 | ||
| Community, n (%) | 316 (57) | 425 (63) | |
| Healthcare-associated, n (%) | 78 (14) | 97 (14) | |
| Nosocomial, n (%) | 161 (29) | 153 (23) | |
| Microbiological data | |||
| Three or more positive blood culture sets, n (%) | 83 (15) | 116 (17) | .312 |
| Pathogens | |||
| | 205 (37) | 295 (44) | .017 |
| Coagulase-negative staphylococci, n (%) | 65 (12) | 52 (8) | .019 |
| Streptococci, n (%) | 132 (24) | 186 (28) | .150 |
| Enterococci, n (%) | 115 (21) | 88 (13) | <.001 |
| Other Gram-positive, n (%) | 18 (3) | 28 (4) | .452 |
| HACEK, n (%) | 8 (1) | 17 (3) | .225 |
| Gram-negative other than HACEK, n (%) | 36 (7) | 47 (7) | .820 |
| Polymicrobial bacteremia, n (%) | 37 (7) | 48 (7) | .822 |
| Infection data at bacteremia onset | |||
| Fever, n (%) | 436 (79) | 548 (81) | .725 |
| Temperature (°C), median (IQR) | 38.3 (37.4–38.9) | 38.5 (37.8–39.0) | .001 |
| Embolic events, n (%) | 86 (16) | 111 (16) | .696 |
| Cerebral embolic events, n (%) | 42 (8) | 47 (7) | .740 |
| Laboratory values at bacteremia onset | |||
| White blood cells (×109/L), median (IQR) | 10.2 (7.2–13.2) | 10.5 (7.7–14.0) | .081 |
| C-reactive protein (mg/l), median (IQR) | 93 (48–170) | 115 (58–213) | .001 |
| Focus of infection | |||
| Infective endocarditis, n (%) | 270 (49) | 327 (48) | .954 |
| Catheter-related, n (%) | 114 (21) | 117 (17) | .164 |
| Bone and joint infection, n (%) | 110 (20) | 168 (25) | .040 |
| Other focus, n (%) | 95 (17) | 81 (12) | .011 |
| Unknown focus, n (%) | 37 (7) | 68 (10) | .040 |
| Management | |||
| Source control | .469 | ||
| Not warranted, n (%) | 304 (55) | 346 (51) | |
| Warranted and performed within 48 h, n (%) | 129 (23) | 170 (25) | |
| Warranted and not performed within 48 h, n (%) | 122 (22) | 159 (24) | |
| Antimicrobial treatment | |||
| Appropriate antimicrobial treatment within 48 h, n (%) | 501 (90) | 653 (97) | <.001 |
| Timing of antimicrobial treatment initiation | <.001 | ||
| Within 24 h, n (%) | 405 (73) | 675 (100) | |
| Within 24–48 h, n (%) | 110 (20) | 0 (0) | |
| Within 48–72 h, n (%) | 40 (7) | 0 (0) | |
| Outcomes | |||
| Persistent bacteremia for at least 48 h from first positive blood culture, n (%) | 156 (28) | 147 (22) | .011 |
| Persistent bacteremia for at least 48 h from antimicrobial treatment onset, n (%) | 106 (19) | 147 (22) | .257 |
| Bone and joint infection within 30 d, n (%) | 7 (1) | 11 (2) | .641 |
| Death within 15 d, n (%) | 9 (2) | 15 (2) | .537 |
| Death within 30 d, n (%) | 26 (5) | 33 (5) | .894 |
| Death within 90 d, n (%) | 64 (12) | 65 (101) | .322 |
- —Swiss National Science Foundation10.13039/501100001711
- —Swiss Heart Foundation10.13039/501100004362
- —Vaudois Foundation for Interventional Cardiology
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management
Infective endocarditis (IE) is associated with high morbidity and mortality [1, 2]. European and American guidelines recommend promptly initiating empirical antimicrobial treatment (AT) in all patients with suspected IE after obtaining 3 sets of blood cultures (BC), regardless of the severity of infection [3, 4]. This recommendation is largely based on studies from other clinical contexts showing an association between early appropriate AT and improved survival [5]. Indeed, delaying AT beyond 4–8 hours in lower respiratory tract, urinary tract, or abdominal infections delays has been linked to poorer outcomes [6]. However, these conclusions are primarily drawn from retrospective studies, whereas prospective studies have not consistently confirmed this association [6]. Furthermore, the impact of delayed AT appears to be influenced by disease severity and is typically driven by patients presenting with sepsis or septic shock [5, 7, 8].
A key concern with immediate AT in suspected IE is the high misdiagnosis rate; only 1 in 4 patients initially suspected of having IE is ultimately diagnosed with the disease, while the others are ruled out, and some of them have no infectious etiology at all [9]. Moreover, empirical AT regimens tend to be broader than targeted therapies, thereby increasing the risk of antimicrobial resistance [6]. Although the timely administration of appropriate AT is well-established as critical in cases of bacteremia or suspected IE, the evidence supporting this approach in patients with mild to moderate illnesses is limited [1, 5, 8, 10–15].
The Working Party of the British Society for Antimicrobial Chemotherapy recommends withholding antimicrobial AT in clinically stable patients with suspected IE until BC results become available [16].
Given the lack of evidence demonstrating improved outcomes from early empirical AT in clinically stable patients, this study aims to evaluate the impact of delaying AT on survival among patients with suspected and confirmed IE.
MATERIALS AND METHODS
Study Design and Setting
This retrospective was study conducted between January 2015 and June 2024 at 2 Swiss tertiary care centers: Lausanne University Hospital (CHUV) and University Hospital Zurich (USZ). It included patients from 3 distinct cohorts:
CHUV retrospective bacteremia cohort (January 2015–December 2021)CHUV prospective cohort of patients with suspected IE (January 2022–June 2024)USZ endocarditis cohort (January 2015–June 2024), including retrospectively enrolled patients from 2015–2017 and prospectively enrolled patients from 2018 onward).
Suspicion of IE for all cohorts was defined as the combination of BC collection and echocardiography performed specifically to investigate IE. The study was approved by the relevant Swiss ethics committees (CER-VD 2021-02516, CER-VD 2017-02137, KEK-2014-0461; BASEC-2017-01140).
Participants
Inclusion criteria were adult patients (≥18 years old), confirmed bacteremia, clinical suspicion of IE, and no documented objection to the use of their data. Exclusion criteria included: presence of sepsis, meningitis, neutropenia, asplenia, heart failure requiring valve surgery, clearly identifiable infectious focus other than IE, ongoing AT or unknown timing of AT initiation in relation to BC collection, or admission to an intensive care unit within 24 hours of bacteremia.
Data on demographics, clinical characteristics, imaging, microbiology, laboratory values, surgical interventions, and pathology were manually retrieved from patient's electronic health records. All data were reviewed by infectious diseases (ID) consultants. In both institutions, ID consultation was mandatory for patients with suspected IE, and follow-up BC were routinely obtained until bloodstream sterilization was confirmed. Since January 2018, the diagnosis of IE has been established by the respective institutional Endocarditis Teams (ET). For cases prior to 2018, IE adjudication was performed by 2 experienced clinicians from each center (CHUV: M. P. O., P. M.; USZ: B. H., M. F.), all of whom have been members of their institution's ET since January 2018. The site of infection other than IE was determined by the ID consultant based on an integrated assessment of clinical presentation, imaging, microbiological data, and surgical findings.
Variables and Definitions
The date of collection of the first positive BC was defined as the onset of infection. A new episode was included if more than 30 days had passed since the completion of AT for the initial bacteremia. Classification of bacteremia cases as community-acquired, healthcare-associated, or nosocomial was based on the criteria established by Friedman et al [17]. Episodes were stratified into 2 groups: Group I included episodes who received empiric AT immediately after BC collection, whereas Group D comprised those in whom AT was deferred until preliminary BC results were available, defined as species identification by matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) or, if inconclusive, the Gram stain result. Appropriate treatment was defined as the administration of at least 1 antimicrobial agent to which the isolated pathogens were susceptible in vitro.
Narrow-spectrum AT were defined as follows: flucloxacillin or cefazolin for monomicrobial methicillin-susceptible Staphylococcus aureus (MSSA) bacteremia; penicillin or amoxicillin for monomicrobial penicillin-susceptible streptococcal bacteremia; and amoxicillin for monomicrobial amoxicillin-susceptible Enterococcus faecalis bacteremia. The time from AT initiation to narrow-spectrum therapy was defined as the duration of broad-spectrum use.
Major embolic events included peripheral arterial embolism, septic pulmonary emboli, cerebral, ocular hepatic, renal or splenic emboli, mycotic aneurysm, Janeway lesions or nail bed hemorrhage. New bone and joint infections (BJI) included septic arthritis, acute osteomyelitis (vertebral or non-vertebral), or orthopedic implant-associated infections, with symptom onset occurring at least 24 hours after first blood culture. The date of the new BJI was defined as the date of symptom specific to that infection. Persistent bacteremia was defined as the presence of at least 1 positive BC for the same pathogen at 48 hours or more after the initial culture.
Statistical Methods
Statistical analyses included the use of chi-square or Fisher's exact test for categorical variables and the Mann–Whitney U test for continuous variables, as appropriate. Kaplan–Meier survival curves and log-rank tests were used to evaluate 30-day mortality in all suspected or confirmed IE episodes, and the 30-day composite primary outcome (mortality, new embolic event, or new bone/joint infection) in patients with suspected or confirmed IE.
To further assess the association between AT timing and 30-day mortality, we performed univariable and multivariable Cox proportional hazards regression analyses in patients with suspected and proven IE, respectively. We also evaluated the association between AT timing and the composite primary outcome among patients with proven IE. Models were adjusted for repeated episodes within individual patients using robust standard errors. Interaction terms and potential effect modifiers were tested to explore whether the association between AT timing and outcomes differed across clinically relevant subgroups. In a sensitivity analysis, we applied inverse probability weights (IPW) for receiving immediate versus delayed AT based on logistic regression analyses using information available at admission (sex, age, comorbidities, Charlson Comorbidity Index, institution, setting of bacteremia onset, fever, temperature, embolic events at bacteremia onset, white blood cells and C-reactive protein). We conducted data analyses using Stata 19.0 SE (StataCorp, College Station, TX, USA).
RESULTS
Among the 4362 episodes, 2702 involved bacteremia and suspected IE (Figure 1). Of these, 1230 of episodes met the inclusion criteria, corresponding to 1152 individual patients (Figure 1). S. aureus was the most frequently isolated pathogen, identified 500 episodes (41%), followed by streptococci (318 episodes; 26%) and enterococci (203; 17%).
Flowchart of included episodes. Abbreviations: AT, antimicrobial treatment; BC, blood culture; CHUV, Lausanne University Hospital; IE, infective endocarditis; USZ, University Hospital Zurich. Suspicion of IE was defined as the combination of blood culture collection and echocardiography performed specifically to investigate IE.
Baseline Characteristics Among 1230 Episodes of Suspected IE
Transthoracic echocardiography, transesophageal echocardiography, ^18^F-FDG PET/CT, and cardiac CT were performed in 1164 (95%), 677 (55%), 215 (18%), and 39 (3%) episodes, respectively. The timing from blood culture collection to the first echocardiography was similar between the 2 centers (CHUV: median 2 days, interquartile range 1–3; USZ: median 2 days, interquartile range 1–4). Overall, IE was diagnosed in 597 episodes (49%) by the ETs or expert clinicians. Of these, IE involved native valves in 400 (67%), prosthetic valves in 156 (26%), and cardiac implantable electronic device leads in 71 (12%) episodes. Among the 633 episodes not diagnosed with IE, the most common alternative diagnoses were catheter-related bloodstream infection (219 episodes; 35%), BJI (190; 30%), and bacteremia of unknown origin (105; 17%).
Immediate AT (Group I) was initiated in 675 (55%) episodes, whereas AT was deferred until preliminary BC results became available (Group D) in 555 (45%) episodes (Table 1). In Group D, AT was initiated within 24 hours in 405 (73%) episodes, within 24–48 hours in 110 (20%) episodes, and within 48–72 hours in 40 (7%) episodes. Among the latter, time to BC positivity data were available in 20 cases; all of which had a time to positivity of ≥36 hours. A higher proportion of episodes in Group I received appropriate AT within 48 hours of BC collection compared to Group D [653 (97%) of 675 episodes versus 501 (90%) of 555 episodes; P < .001]. Source control interventions were deemed necessary in 580 episodes (47%) and were successfully performed in 299 of these cases (52%). The rate of source control intervention, when indicated, was similar between Groups I and D [170 (52%) of 329 episodes versus 129 (51%) of 251 episodes; P = 1.000].
Supplementary Table 1 presents data on the initiation of narrow-spectrum AT in cases of monomicrobial bacteremia caused by MSSA, penicillin-susceptible streptococci, or amoxicillin-susceptible E. faecalis. Among 863 episodes, a comparable proportion of episodes in Group I and Group D received narrow-spectrum treatment [398/476 (84%) versus 328/378 (87%); P = .061]. However, narrow-spectrum AT was initiated later in Group I (mean 2.8 ± 5.7 days) than in Group D (mean 1.7 ± 3.4; P < .001). Consequently, the duration of broad-spectrum AT was longer in Group I (mean 2.8 ± 5.7) compared to Group D (mean 1.5 ± 3.4; P < .001).
Baseline Characteristics Among 597 IE Episodes
Of the 1137 episodes of proven bacteremic IE, 597 (53%) met the inclusion criteria. Immediate AT (Group I) was initiated in 327 (55%) episodes, and deferred (Group D) in 270 (45%) episodes (Supplementary Table 2). Supplementary Table 3 presents data on the initiation of narrow-spectrum AT in 451 episodes of monomicrobial IE caused by MSSA, penicillin-susceptible streptococci, or amoxicillin-susceptible E. faecalis. A smaller proportion of episodes in Group I received narrow-spectrum agents compared to Group D [193/250 (77%) versus 172/201 (86%); P = .030]. Narrow-spectrum AT was initiated later in Group I (mean 3.2 ± 7.1 days) than in Group D (2.2 ± 4.2 days; P = .067), and the duration of broad-spectrum AT was longer in Group I (3.2 ± 7.1 days) compared to Group D (1.9 ± 4.2 days; P = .001).
Outcome Among 1230 Episodes With Suspected IE
Thirty-day mortality was 5% (59 episodes). Kaplan–Meier analysis showed no evidence of a difference in 30-day mortality between Group I and Group D [26 (5%) out of 675 episodes versus 33 (5%) out of 555 episodes; log-rank test P = .854] (Figure 2A).
Kaplan–Meier analysis based on the timing of antimicrobial treatment initiation: A, 30-day mortality among all 1230 episodes (log-rank test: P = .854); B, 30-day mortality among 597 infective endocarditis episodes (log-rank test: P = .174); and C, 30-day primary endpoint (composite of mortality, new embolic event, or new bone and joint infection) among 597 infective endocarditis episodes (log-rank test: P = .263).
Supplementary Table 4 compares baseline characteristics between 30-day survivors and non-survivors among episodes with suspected IE. Figure 3A and Supplementary Table 5 show the uni- and multivariable Cox regression analysis of 30-day mortality among the same patients. In the multivariable model, independent predictors of increased 30-day mortality included Charlson Comorbidity Index >4 (aHR 3.43; 95% CI 1.85–6.36) and persistent bacteremia (2.60; 1.51–4.46). Appropriate treatment within 48 hours remained protective (0.42; 0.20–0.88). Immediate initiation of antimicrobial treatment was not associated with lower 30-day mortality (1.28; 0.75–2.20). In the sensitivity analysis of 1081 episodes with suspected IE and with complete baseline information, the logistic regression to calculate the probability of initiating immediate AT yielded a poor to moderate model performance with a ROC AUC of 0.65. The Cox regression analysis with IPW showed that immediate AT was not associated with lower 30-day mortality (0.99; 0.56–1.74).
Uni- and multivariable Cox regression analysis of A, 30-day mortality among all 1230 episodes, and B, 30-day primary endpoint (composite of mortality, new embolic event, or new bone and joint infection) among 597 infective endocarditis episodes. Abbreviations: CHUV, Lausanne University Hospital; USZ, University Hospital Zurich.
Outcome Among 597 Episodes With IE
The composite 30-day primary endpoint occurred in 157 episodes (26%). Specifically, 30-day mortality was 4% (25 episodes), new embolic events occurred in 134 episodes (22%), and new BJIs in 11 episodes (2%). Kaplan–Meier analyses showed no evidence of a difference regarding 30-day mortality (log-rank test: P = .174) (Figure 2B), or primary endpoint (log-rank test: P = .263) (Figure 2C).
Supplementary Table 6 compares baseline characteristics between episodes that did and did not meet the 30-day composite primary endpoint among IE episodes. Multivariable analysis identified as independent predictors of the composite primary outcome persistent bacteremia (aHR 1.50; 95% CI 1.03–2.18), USZ (1.39; 1.01–1.93), and valve endocarditis (3.56; 1.46–8.68) (Figure 3B and Supplementary Table 7). Supplementary Table 8 show the uni- and multivariable Cox regression analysis of 30-day mortality among IE episodes. Immediate initiation of antimicrobial treatment was not associated with lower composite primary endpoint (1.32; 0.95–1.83) nor with lower 30-day mortality (2.51; 0.93–6.78). In the 505 IE episodes with complete baseline information, the IPW Cox regression analysis (ROC AUC 0.7) showed that immediate AT was neither associated with a lower composite primary endpoint (1.10; 0.76–1.61) nor with lower 30-day mortality (0.81; 0.38–2.41).
DISCUSSION
In this large, combined cohort of clinically stable patients with suspected IE, we found no evidence that deferring AT was associated with worse outcomes compared to immediate AT. These findings were consistent even when focusing specifically on clinically stable patients with confirmed IE, who comprised approximately half of the study population.
The decision to initiate AT appeared driven by clinical presentation rather than age or comorbidities, as baseline characteristics were comparable between groups. Immediate AT was more frequently observed in patients with S. aureus bacteremia, consistent with its acute presentation, while Enterococcus spp., generally causing a more indolent course, was associated with delayed AT [18, 19].
In Group D, 73% received AT within 24 hours, and 90% within 48 hours, compared to 97% in Group I. Delays beyond 48 hours were mainly due to late BC positivity and the time required for species identification. Notably, in most cases of monomicrobial bacteremia, narrow-spectrum AT was initiated within 2 days of BC collection, facilitated by rapid diagnostics [20–22].
In our analysis, timing of AT administration was not associated with 30-day mortality. These findings challenge current European and American guidelines [3, 4], which recommend immediate AT in all patients with suspected IE, regardless of disease severity. Mortality instead correlated with higher Charlson Comorbidity Index, persistent bacteremia beyond 48 hours, and inappropriate AT within the first 48 hours [1, 5, 8, 10–15]. Source control procedures rates, critical for bacteremia clearance and recognized predictor of clinical outcomes, were similar across groups [13–15, 23]. Although persistent bacteremia at 48 hours was more common in Group D, this association disappeared after adjusting for AT. Prior studies highlighted the importance of appropriate AT in bacteremia, particularly among severely ill patients [5, 8, 10, 11, 13–15]. However, in patients with less severe presentation, limited to under 24 hours have not been linked to increased mortality [8, 10, 11]. Our findings align with this evidence, showing that short delays in stable patients with suspected IE did not worsen outcomes. A similar observation was seen in S. aureus bacteremia, where delayed treatment was associated with poorer outcomes, only in patients with severe presentation [24].
One key advantages of withholding empiric AT in stable patients is the support of antimicrobial stewardship efforts [6]. A major rationale for deferring AT in stable patients also lies in the relatively low diagnostic yield of the Duke criteria. Nearly half of patients were ultimately diagnosed with a condition other than IE. Similarly, a previous study involving 3127 patients with suspected IE found that only 38% were ultimately diagnosed with IE. In contrast, 43% had an alternative bacterial infection, and 19% had a non-infectious condition [9]. Many of the alternative bacterial infections identified did not require immediate AT, and patients with non-infectious diagnoses will not benefit from AT. Immediate AT in all suspected IE cases would result in substantial unnecessary antimicrobial exposure. In contrast, withholding treatment allowed for more targeted and judicious use of AT, as evidenced by the earlier and more frequent use of narrow-spectrum agents among patients in Group D.
Beyond mortality, a major concern in IE is the risk of new embolic events, though incidence typically declines after the first 2 weeks of treatment [25, 26]. In this study, no difference was observed in new embolic events between Groups I and D. Both groups had comparable proportions of embolic events at the time of BC collection and similar rates of large vegetations, which are strong predictors of embolic complications during treatment [1, 25–27]. These findings suggest that deferring AT until BC results does not increase the risk of new embolic events or secondary BJI.
This study has limitations. The study conducted within a single healthcare system, where patients had access to consistent ID consultation and specialized ETs. Both institutions used MALDI-TOF technology directly from positive BCs, thus reducing the time to species identification [21]. These factors may limit the generalizability of our findings to other healthcare settings. Selection bias is inherent, as the decision to initiate or defer AT was based on complex clinical judgments not fully captured in the available data. Although we adjusted for numerous baseline variables using IPW, residual confounding by unmeasured factors cannot be excluded. Nonetheless, factors such as regional differences in clinical practice and antimicrobial stewardship policies may have influenced our results. Patients at CHUV were more likely to receive immediate AT, whereas at USZ, deferral of treatment until BC results was more common, consistent with previously reported regional variations in antimicrobial use in Switzerland [28, 29]. Moreover, in the majority of episodes, suspicion of IE did not arise at initial presentation, but only after the first blood culture results were available, as previously shown in a Swedish study that found that IE was suspected at presentation in only 23% of cases [30]. However, the exact timing of when IE was first suspected, as well as the interval between patient presentation and the collection of the initial blood cultures, was not systematically recorded. Safety outcomes, including adverse drug events such as Clostridioides difficile infection, were not systematically recorded, limiting comparisons of treatment-related harms between groups. Lastly, parameters reflecting medical decisions, such as the immediate initiation of antimicrobial treatment, are based on complex clinical evaluations that are not fully captured during data collection.
While early empirical AT may accelerate microbiological clearance, our findings suggest that deferring AT until initial BC results in clinically stable patients with suspected or confirmed IE did not negatively affect mortality or embolic complications. These findings advocate for a careful, patient-centered approach to initiating AT in clinically stable patients with suspected IE, particularly in cases with diagnostic uncertainty helping to avoid unnecessary use of broad-spectrum antimicrobials. Importantly, immediate AT remains essential for patients with sepsis, neutropenia, asplenia, or a clear alternative infectious focus. In contrast, the mere suspicion of IE in otherwise stable patients should not automatically trigger AT. These findings underscore the potential for antimicrobial stewardship even in high-stakes scenarios, but should be validated in external cohorts, especially in settings with a high burden of antimicrobial resistance.
Supplementary Material
ofaf628_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dickerman SA, Abrutyn E, Barsic B, et al The relationship between the initiation of antimicrobial therapy and the incidence of stroke in infective endocarditis: an analysis from the ICE Prospective Cohort Study (ICE-PCS). Am Heart J 2007; 154:1086–94.18035080 10.1016/j.ahj.2007.07.023 · doi ↗ · pubmed ↗
- 2Bin Abdulhak AA, Baddour LM, Erwin PJ, et al Global and regional burden of infective endocarditis, 1990–2010: a systematic review of the literature. Glob Heart 2014; 9:131–43.25432123 10.1016/j.gheart.2014.01.002 · doi ↗ · pubmed ↗
- 3Delgado V, Ajmone Marsan N, de Waha S, et al 2023 ESC guidelines for the management of endocarditis. Eur Heart J 2023; 44:3948–4042.37622656 10.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 4Baddour LM, Wilson WR, Bayer AS, et al Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015; 132:1435–86.26373316 10.1161/CIR.0000000000000296 · doi ↗ · pubmed ↗
- 5Corl KA, Zeba F, Caffrey AR, et al Delay in antibiotic administration is associated with mortality among septic shock patients with Staphylococcus aureus bacteremia. Crit Care Med 2020; 48:525–32.32205599 10.1097/CCM.0000000000004212 · doi ↗ · pubmed ↗
- 6Naucler P, Huttner A, van Werkhoven CH, et al Impact of time to antibiotic therapy on clinical outcome in patients with bacterial infections in the emergency department: implications for antimicrobial stewardship. Clin Microbiol Infect 2021; 27:175–81.32120032 10.1016/j.cmi.2020.02.032 · doi ↗ · pubmed ↗
- 7Alam N, Oskam E, Stassen PM, et al Prehospital antibiotics in the ambulance for sepsis: a multicentre, open label, randomised trial. Lancet Respir Med 2018; 6:40–50.29196046 10.1016/S 2213-2600(17)30469-1 · doi ↗ · pubmed ↗
- 8Van Heuverswyn J, Valik JK, Desirée van der Werff S, Hedberg P, Giske C, Nauclér P. Association between time to appropriate antimicrobial treatment and 30-day mortality in patients with bloodstream infections: a retrospective cohort study. Clin Infect Dis 2023; 76:469–78.36065752 10.1093/cid/ciac 727PMC 9907509 · doi ↗ · pubmed ↗