Novel variant of the NCSTN gene identified in a woman with hidradenitis suppurativa
Conrad Hempel, Sonja Grunewald, Till Mittank‐Weidner, Jan‐Christoph Simon, Franziska Schnabel, Robin‐Tobias Jauss, Viktor Schnabel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1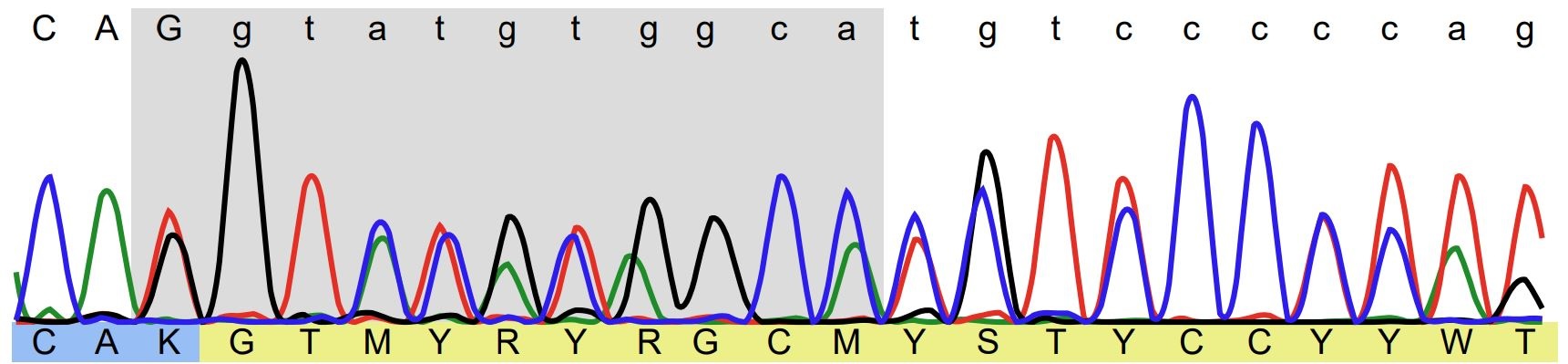 Figure 2
Figure 2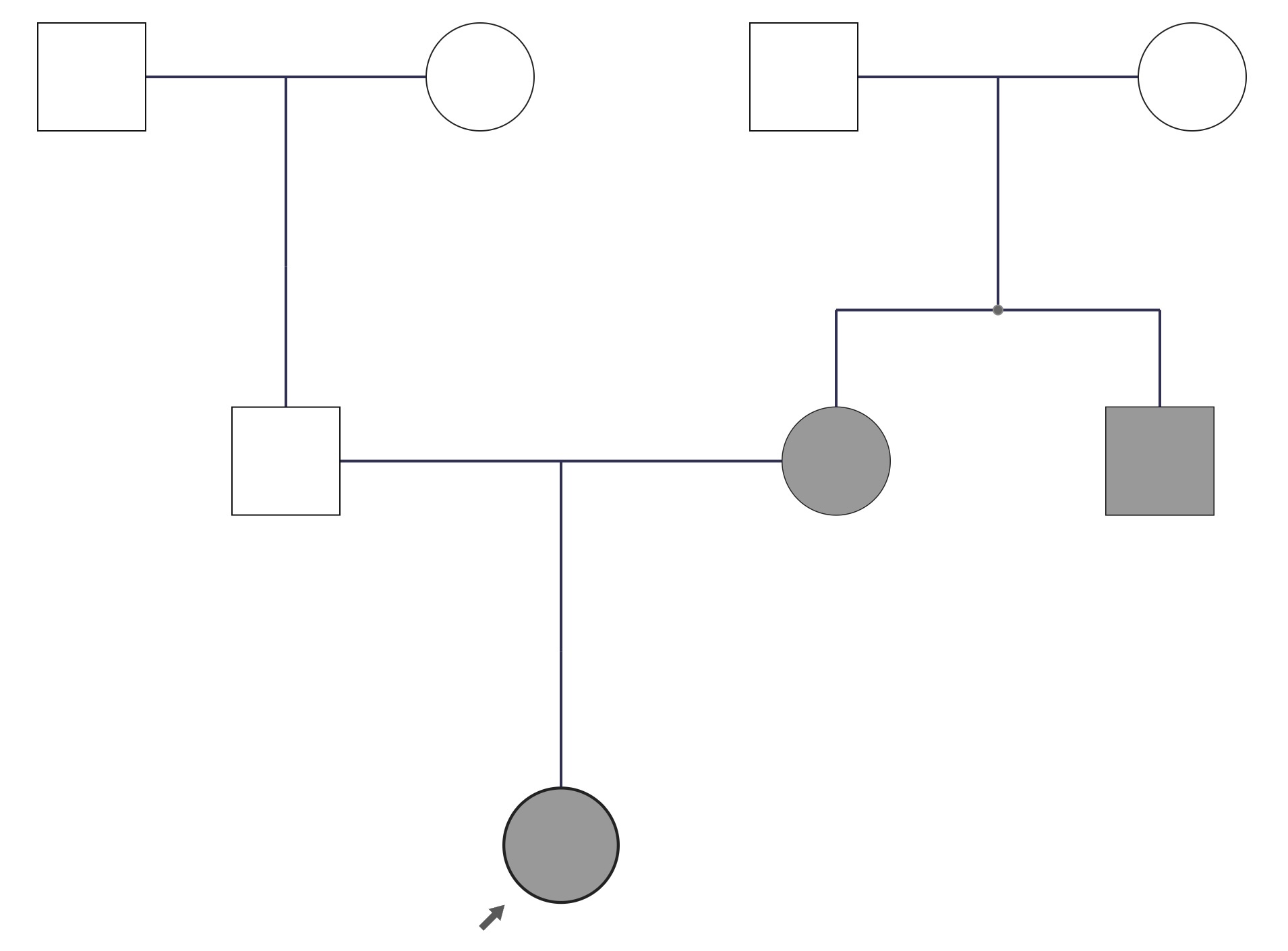 Figure 3
Figure 3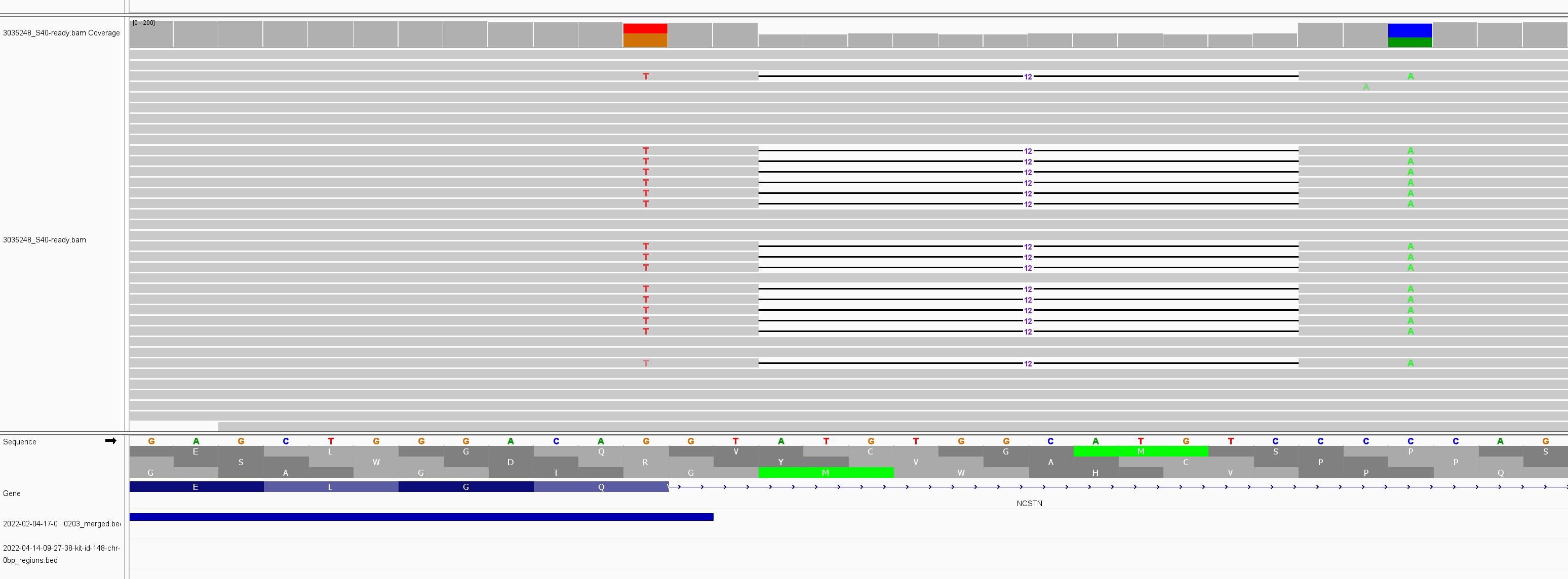 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHidradenitis Suppurativa and Treatments · Colorectal and Anal Carcinomas
Dear Editors,
A Caucasian 27‐year‐old female with a 4‐year history of hidradenitis suppurativa presented to our outpatient clinic. She reported undergoing repeated extensive surgical procedures for the removal of dermal abscesses in the axillae and groin, which, interestingly, also appeared in uncommon locations such as the trunk and thighs. Prior to this, she had been treated intermittently with antibiotics, isotretinoin, and a contraceptive pill. Additionally, anti‐TNF‐α antibody therapy had been administered for 6 months, and most recently, treatment with an anti–IL‐17 agent had been given for 3 months. All medications had been discontinued, either due to side effects or lack of efficacy.
She mainly complained of severe pain caused by recurrent abscesses, which resulted in an inability to work. She denied nicotine use and had a BMI of 18.5. Due to comorbid depression and anxiety disorder, she was receiving psychological support. Her Dermatology Life Quality Index (DLQI) score was 29.
Dermatological examination showed many inflammatory papules, comedones and pustules distributed over her whole body with predominant areas of face trunk und upper legs being involved. Abscess formations up to 2 cm diameter could be found in both axillae, in the pubic and gluteal area (Figure 1a,b), corresponding to Hurley grade 2. Interestingly, both her mother and maternal uncle had a history of recurrent painful abscesses, though to a lesser extent (online supplementary Figure S1).
Because of the positive family history, we performed whole exome sequencing using TWIST Human Core Exome Kit (TWIST Bioscience, San Francisco, USA) on an Illumina NovaSeq6000 sequencer (Illumina, San Diego, USA). Analysis using the browser‐based genomics software Varvis (Limbus Medical Technologies GmbH, Rostock, Germany) identified a heterozygous truncating variant in the NCSTN gene (NM_015331.3:c.1101_1101+17delinsTGTCCA, p.(Gln367Hisfs*6)) (online supplementary Figure S2). We obtained a mean coverage of the NCSTN gene of 79.49 times and the variant was confirmed in more than 50 reads with a quality score of 1918 (GATK HaplotypeCaller) and no conflicting reads in the area. For confirmation, Sanger sequencing was performed (online supplementary Figure S3). The variant causes a frameshift and premature protein truncation, but has not been reported in variant databases (HGMD, Decipher, ClinVar) or described in the literature. The variant is also absent from the general population database gnomAD, which includes sequencing data from over 1,150,000 European (non‐Finnish) controls at the variant position. According to ACMG Classification the variant was classified as pathogenic (criteria applied: PVS1, PM2_SUP, PP4).1 Unfortunately, other family members were not available for segregation analysis.
Hidradenitis suppurativa (HS), also known as Acne inversa, is a chronic, inflammatory, recurrent disease of the hair follicle that usually presents with painful, inflamed lesions, most commonly in the axillar, inguinal and anogenital region.2 The prevalence in Europe is about 1%.2 The typical age range for the onset of HS is generally between 20 and 40 years.3 Approximately 40% of cases can be classified as familial, in addition to syndromic and sporadic variants.3 Familial HS is generally characterized by more severe symptoms and earlier age of onset.3 In the literature, at least four different genes of the γ‐secretase complex have been reported as causative for HS, including NCSTN, PSENEN, PSEN1, and APH1B.4, 5 NCSTN encodes Nicastrin, a type‐1 transmembrane glycoprotein of the y‐secretase complex, which plays a central role in Notch signaling pathway and controls anti‐proliferative and differentiation‐promoting effects in human keratinocytes. Knockdown of NCSTN leads to increased proliferation and decreased differentiation of keratinocytes, primarily mediated through the Notch and PIK‐AKT signalling pathways.6 So far, 52 variants in NCSTN have been described in HS.7 A monogenic variation in NCSTN is linked to an earlier onset and atypical presentation at uncommon skin sites such as the torso. Furthermore, low body weight and an increased likelihood of treatment with biological therapy distinguish this genetic variant from classic HS, as confirmed by this case.7 The interaction between genetic factors and dysregulation of immune mediators such as TNF‐α, IL‐1β, IL‐17, and IL‐12/23 contributes to the chronic inflammatory nature of HS.3 Potential therapeutic targets are therefore anti‐TNF‐α, anti‐IL‐1α, anti‐IL‐17, and anti‐IL‐12/23 therapies as well as JAK inhibitors.
This case provides further evidence regarding the functional implication of NCSTN variants in the pathogenesis of familial HS, which has been described mainly in Asian populations.8, 9
In our patient we described a novel truncating NCSTN variant leading to HS. Interestingly, no environmental exacerbating factors, such as obesity or smoking could be identified in our patient. Clinically, the phenotype belongs to the rarer “follicular” subtype of HS, which was described by Canoui‐Poitrine et al as one of three subtypes.10 It is mainly characterized by follicular lesions, such as comedones, epidermal cysts, sinus pilonidalis and acne vulgaris and shows a more severe course of disease than the regular axillary/groin type. It should be noted that the comedones observed in our patient cannot solely account for the severe destructive inflammation. Considering the genetic background, this report provides further evidence that HS can no longer be considered a simple “disease of follicular occlusion”. The significant role of inflammation and innate/adaptive immunity in familiar HS cannot be overstated and raises the question whether follicular occlusion is a primary or secondary phenomenon in the pathogenesis of the disease.
Our case report broadens the genetic spectrum associated with HS. In combination with the clinical phenotype, it provides valuable information for future studies on treatment strategies and surveillance programs in affected families.
CONFLICT OF INTEREST STATEMENT
None.
Supporting information
Supplementary information
Supplementary information
Supplementary information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Richards S , Aziz N , Bale S , et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405‐424.25741868 10.1038/gim.2015.30PMC 4544753 · doi ↗ · pubmed ↗
- 2Zouboulis CC , Desai N , Emtestam L , et al. European S 1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol. 2015;29(4):619‐644.25640693 10.1111/jdv.12966 · doi ↗ · pubmed ↗
- 3Chu YL , Yu S . Hidradenitis Suppurativa: An Understanding of Genetic Factors and Treatment. Biomedicines. 2024;12(2):338.38397941 10.3390/biomedicines 12020338 PMC 10886623 · doi ↗ · pubmed ↗
- 4Pink AE , Simpson MA , Desai N , et al. Mutations in the γ‐secretase genes NCSTN, PSENEN, and PSEN 1 underlie rare forms of hidradenitis suppurativa (acne inversa). J Invest Dermatol. 2012;132(10):2459‐2461.22622421 10.1038/jid.2012.162 · doi ↗ · pubmed ↗
- 5Ratnamala U , Jain N , Jhala D , et al. An Updated Mutation Spectrum of the γ‐Secretase Complex: Novel NCSTN Gene Mutation in an Indian Family with Hidradenitis Suppurativa and Acne Conglobata. Indian J Dermatol. 2023;68(2):141.37275792 10.4103/ijd.ijd_995_21PMC 10238988 · doi ↗ · pubmed ↗
- 6Xiao X , He Y , Li C , et al. Nicastrin mutations in familial acne inversa impact keratinocyte proliferation and differentiation through the Notch and phosphoinositide 3‐kinase/AKT signalling pathways. Br J Dermatol. 2016;174(3):522‐532.26473517 10.1111/bjd.14223 · doi ↗ · pubmed ↗
- 7Mintoff D , Pace NP , Borg I . NCSTN In‐Frame Deletion in Maltese Patients With Hidradenitis Suppurativa. JAMA Dermatol. 2023;159(9):939‐944.37494055 10.1001/jamadermatol.2023.2227 PMC 10372757 · doi ↗ · pubmed ↗
- 8Xiao XM , Yang WZ , Lin LH , Li CR . Two novel nicastrin mutations in Chinese families with acne inversa. J Dermatol. 2020;47(12):e 449‐e 451.32940366 10.1111/1346-8138.15575 · doi ↗ · pubmed ↗