BAPoma, a rare nevus, as the key to a diagnosis of BAP1‐associated tumor predisposition syndrome
Lara Racz, Sandra Pasternack‐Ziach, Isabel Spier, Stephan Forchhammer, Claudia Rehkämper, Peter Kind, Julia Reifenberger, Silke Redler

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
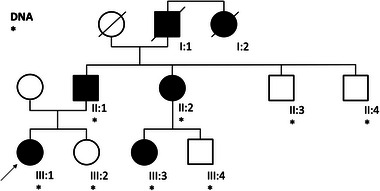 Figure 1
Figure 1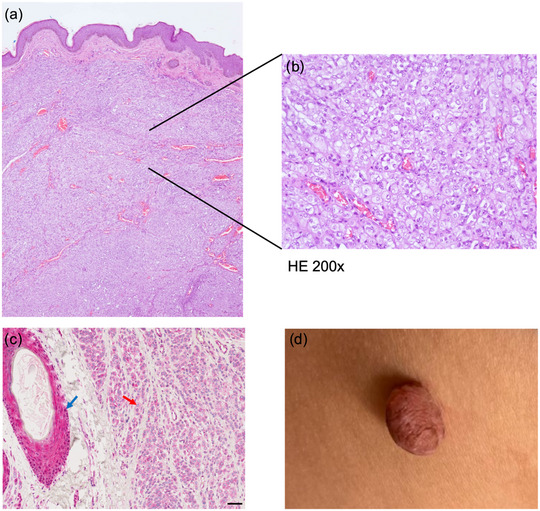 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases · Medical Imaging and Pathology Studies · Urologic and reproductive health conditions
Dear Editors,
A 23‐year‐old female presented to our clinic with progressively changing nevi. Skin cancer screening, including body mapping, was performed, and three suspicious nevi were excised from both the dorsal and ventral flanks. The first two were found to be junctional nevi. However, the histology of the tissue from the ventral flank revealed a melanocytic nevus with partial BAP1‐inactivation (BAPoma) (Figure 1). Immunohistochemistry of the latter revealed a loss of nuclear BAP1 expression (Figure 1). DNA was extracted from peripheral blood leucocytes. Sequencing and deletion/duplication screening of BRCA1‐Associated Protein 1 (BAP1) was performed in accordance with German gene diagnostic law. This revealed the heterozygous pathogenic germline variant c.1813G>T;p.(Glu605Ter), which results in a premature stop codon. A diagnosis of BAP1‐associated tumor predisposition syndrome (BAP1‐TPS) was made. In the present index patient, assessment of the family history over three generations revealed a familial clustering of tumors, some of which manifested in early adulthood (Figure 2). Interestingly, at the age of 23 years, the paternal cousin (III:3) had undergone excision of two suspicious skin lesions, which were found to be BAPomas. The father (II:1) had developed urothelial carcinoma of the urinary bladder at the age of 47 years, followed by metastatic recurrence. At the age of 54 years, a diagnosis of pleural mesothelioma was made. In addition, the patient's father had undergone excisions of numerous basal cell carcinomas since then. The paternal aunt (II:2) had 50 to 60 colonic adenomatous polyps removed since the age of 47 years, but carried no pathogenic germline variant in known polyposis‐associated susceptibility genes. She had at least three basal cell carcinomas excised from the neck area between the ages of 40 and 45 years. The paternal grandfather had died from renal cell carcinoma at the age of 75 years, and his sister had died from metastatic breast cancer at the age of 41 years. Thus, segregation of the familial BAP1 variant was no longer possible. Except for a paternal cousin (III:4), all tested family members carried the familial BAP1 variant (Figure 2).
BAP1‐associated tumor predisposition syndrome was first described in 2011.1 This rare familial cancer syndrome shows autosomal dominant inheritance, and involves pathogenic germline variants in BAP1, whose main function is tumor suppression at molecular levels. BAP1 was named based on its interaction with BRCA1 (BReast CAncer Gene 1), which ensures the repair of double‐stranded DNA breaks and genomic stability.2 BAP1 is recruited to double‐strand DNA break sites and promotes repair by homologous recombination by facilitating BRCA1 recruitment.3 Moreover, it is part of the polycomb group repressive deubiquitinase complex (PR‐DUB), which removes ubiquitin from histones (H2AK119ub), regulating gene transcription. Loss of BAP1 disrupts this process, resulting in altered expression of genes involved in cell cycle control, DNA damage repair, and metabolism.4 BAP1‐TPS is associated with predisposition to multiple tumors, including benign melanocytic cutaneous tumors and numerous malignant tumors in distinct organ systems.5 As with many rare TPS, it remains unclear which cancers are unequivocally associated with BAP1‐TPS. Consensus exists that the core phenotype includes BAPoma, as well as cutaneous melanoma, uveal melanoma, basal cell carcinoma, malignant mesothelioma of the pleura and peritoneum, and renal cell carcinoma. Furthermore, research has identified possible BAP1‐TPS associations with meningioma, cholangiocarcinoma, as well as breast, urinary bladder, and lung cancer.1, 6, 7 BAPoma is often the initial manifestation of this rare TPS.
Clinically, BAP1‐inactivated nevi appear as dome‐shaped, skin‐colored or reddish papules. Histologically, they typically present as dermal‐based melanocytic proliferations that are combined with prominent epithelioid cells. The latter may show nuclear pleomorphism and abundant amphophilic cytoplasm. These show an immunohistochemical loss of nuclear BAP1 expression.8, 9 Dermatologists are ideally positioned to recognize specific clinical features and to initiate germline testing and genetic counseling. This plays a crucial role in identifying high‐risk individuals for early screening strategies aimed at detecting malignant tumors in their initial stages and intercepting cancers before they become aggressive. In 2023, detailed recommendations on BAP1‐TPS clinical management were published by a panel of experts from Europe, highlighting the need for regular skin and ocular screening as well as renal imaging.10 The tumor spectrum described in the present report expands the phenotypic variability of BAP1‐TPS. In particular, this is the first BAP1‐TPS report to describe colonic adenomatous polyps (II:2), although we cannot exclude the possibility that the colonic adenomatous polyps developed independently of the familial BAP1 variant.
The present case demonstrates the difficulties involved in characterizing rare tumor syndromes for which limited scientific evidence is available. Characterizing the associated tumor spectrum, establishing respective genotype‐phenotype correlations, and exploring the utility of surveillance and clinical management are crucial steps forward. In conclusion, our report describes a BAP1‐TPS family with cutaneous and non‐cutaneous tumor manifestations. BAP1‐TPS is rare, and due to its varied phenotype – even within families – BAPoma may represent a valuable tool for identification. Early recognition of BAP1‐TPS facilitates the initiation of cancer surveillance to prevent advanced malignancies.
CONFLICT OF INTEREST STATEMENT
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Testa JR , Cheung M , Pei J , et al. Germline BAP 1 mutations predispose to malignant mesothelioma. Nat Genet. 2011;43(10):1022‐1025.21874000 10.1038/ng.912PMC 3184199 · doi ↗ · pubmed ↗
- 2Jensen DE , Proctor M , Marquis ST , et al. BAP 1: a novel ubiquitin hydrolase which binds to the BRCA 1 RING finger and enhances BRCA 1‐mediated cell growth suppression. Oncogene. 1998;16(9):1097‐1112.9528852 10.1038/sj.onc.1201861 · doi ↗ · pubmed ↗
- 3Yu H , Pak H , Hammond‐Martel I , et al. Tumor suppressor and deubiquitinase BAP 1 promotes DNA double‐strand break repair. Proc Natl Acad Sci U S A. 2014;111(1):285‐290.24347639 10.1073/pnas.1309085110 PMC 3890818 · doi ↗ · pubmed ↗
- 4Ge W , Yu C , Li J , et al. Basis of the H 2AK 119 specificity of the Polycomb repressive deubiquitinase. Nature. 2023;616(7955):176‐182.36991118 10.1038/s 41586-023-05841-y · doi ↗ · pubmed ↗
- 5Wiesner T , Obenauf AC , Murali R , et al. Germline mutations in BAP 1 predispose to melanocytic tumors. Nat Genet. 2011;43(10):1018‐1021.21874003 10.1038/ng.910PMC 3328403 · doi ↗ · pubmed ↗
- 6Carbone M , Yang H , Pass HI et al. BAP 1 and Cancer. Nat Rev Cancer. 2013;13(3):153‐159.23550303 10.1038/nrc 3459 PMC 3792854 · doi ↗ · pubmed ↗
- 7Abdel‐Rahman MH , Pilarski R , Cebulla CM , et al. Germline BAP 1 mutation predisposes to uveal melanoma, lung adenocarcinoma, meningioma, and other cancers. J Med Genet. 2011;48(12):10.1136/jmedgenet-2011-100156.PMC 382509921941004 · doi ↗ · pubmed ↗
- 8Haugh AM , Njauw CN , Bubley JA , et al. Genotypic and Phenotypic Features of BAP 1 Cancer Syndrome. JAMA Dermatol. 2017;153(10):999‐1006.28793149 10.1001/jamadermatol.2017.2330 PMC 5710339 · doi ↗ · pubmed ↗