Type I IFN receptor blockade by anifrolumab reduces cutaneous lupus in monogenic SLE
Julian Steininger, Christine Wolf, Min Ae Lee‐Kirsch, Claudia Günther

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
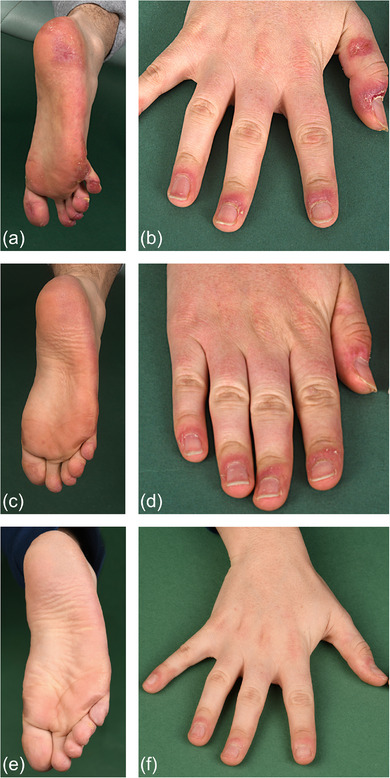 Figure 1
Figure 1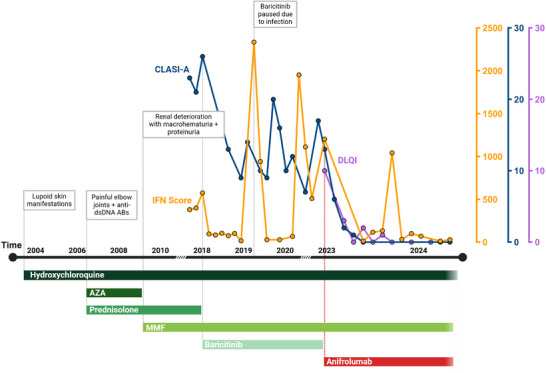 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · T-cell and B-cell Immunology · Immune Cell Function and Interaction
Dear Editors,
We report the complete remission (CR) of cutaneous lupus erythematosus (CLE) in a 24‐year‐old man with early‐onset lupus caused by a biallelic C1QC mutation,1 achieved under treatment with the interferon‐alpha/beta receptor (IFNAR) antagonist anifrolumab.
Monogenic deficiencies in C1 components (C1QDef) are extremely rare with only 74 reported cases.2 They are strongly associated with increased expression of type I interferon (IFN) and type I IFN‐stimulated genes (ISGs), which drive an innate immune response against self, resulting in a lupus‐like phenotype. The symptoms in patients with C1QDef typically manifest in early childhood and, unlike in sporadic systemic lupus erythematosus (SLE), usually exhibit a poor response to standard SLE treatments. Therapies involving regular fresh frozen plasma or hematopoietic stem cell transplantation carry a high risk of complications. In addition to significant morbidity, C1QDef is also associated with increased mortality.3
Our patient suffered from early onset CLE‐like manifestations, with the first cutaneous symptoms noticed at the age of 4 (10/2003), for which he was treated with hydroxychloroquine (Figure 1). In April 2004, proteinuria, increased rheumatoid factors, and anti‐nuclear, anti‐cardiolipin, and anti‐SSA antibodies appeared, resembling manifestations of SLE. Two years later, the patient began to experience fluctuating pain and swelling in the elbow joints. Additionally, borderline levels of anti‐double‐stranded DNA antibodies were detected, prompting the initiation of therapy with azathioprine and prednisolone. Due to severe renal deterioration with macrohematuria and proteinuria (12/2008), the patient was switched to mycophenolate (MMF) in combination with hydroxychloroquine.
From 2015 onwards, the SLE flares, including acute and discoid skin lesions (Figure 2), required monthly pulse therapy with prednisolone. Mutation analyses, performed after the first presentation in our clinic (02/2018), revealed a homozygous mutation in the C1QC gene (c.205C>T, p.Arg69Ter).1 Because of inadequate disease control, the JAK inhibitor (JAKi) baricitinib was added to the treatment. The drug was well tolerated and symptoms improved.1 However, fluctuating discoid plaques remained, especially on the face, and CLE Disease Area and Severity Index Activity (CLASI‐A) scores4 did not normalize completely (Figures 1, 2). Interestingly, the IFN score in blood declined significantly but this did not correlate with CR of CLE. Therefore, treatment was switched from baricitinib to infusions of 300 mg anifrolumab every 4 weeks. Anifrolumab is an IgG1κ monoclonal antibody that inhibits the binding of all type I IFN subtypes to their single common receptor. Several case series and clinical trials have demonstrated its efficacy in the treatment of CLE lesions.5, 6 The drug was most effective in patients with elevated type I IFNs,7, 8 and has been shown to substantially reduce the type I IFN signature in SLE patients.9
A rapid clinical response was observed following the first infusion with anifrolumab: previously refractory skin lesions improved by 50% within one month, as measured by CLASI‐A scores, and resolved almost completely within 12 months of treatment (Figures 1, 2). Importantly, the highly therapy‐resistant chilblain like lesions and vasculitis of the fingers and palms responded to the IFN blockade (Figure 2). This underscores the rarely reported observation of potential efficacy of anifrolumab in chilblain lupus.10 The patient's quality of life also improved (Figure 1).
The patient did not report any severe adverse events. However, he experienced a significant increase in the frequency of mild respiratory infections as well as a first episode of thoracic herpes zoster, which prompted us to extend the treatment intervals to 6 weeks. This was tolerated but accompanied by recurrent flares of CLE already after 2 months. Consequently, the previous treatment interval of 4 weeks was readopted.
Adding anifrolumab to baseline therapy with hydroxychloroquine and MMF resulted in superior control of CLE compared to baricitinib (median CLASI‐A baricitinib 13.00, median CLASI‐A anifrolumab 1.00; p = 0.0009).6, 7, 11, 12 In line with our findings, Triaille et al. also reported insufficient disease control with JAKi treatment.3 This may be explained by the fact that C1QDef‐patients exhibit similarly high IFN signatures as in classic interferonopathies, which could account for the superior outcomes achieved with direct IFNAR‐blockade. In contrast, JAKi impact multiple signaling pathways as JAKs are involved in the signal transduction of various cytokines. Consequently, JAKi may provide a broader, albeit potentially less complete, blockade of the affected type I IFN pathway. However, further studies are required to fully elucidate the long‐term effects of both drugs.
Given the absence of head‐to‐head studies between JAKi and anifrolumab, it remains possible that anifrolumab may also demonstrate superior pharmacological efficacy on cutaneous inflammation. The improved clinical response, however, is not reflected in the type‐I IFN score in the blood, which decreased to a comparable extent under both baricitinib and anifrolumab. Therefore, documentation of the CLE maifestations using verified clinical scores is important in clinical trials in SLE and their correlation with ISG levels in blood needs to be further validated.
FUNDING
This work was supported by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), grant TRR237 369799452/404458960 to C.G. M.L.‐K. is supported by DFG grants CRC237 369799452/B21, CRC237 369799452/A11, CRC369 501752319/C06 and by grants of the German Federal Ministry of Education and Research (BMBF) 01GM2206C (GAIN) and 01GL2405H (DZKJ). C.W. is supported by the DFG grant CRC237 369799452/A06.
CONFLICT OF INTEREST STATEMENT
C.G. has received honoraria for scientific lectures, participation on advisory boards, and research funding from AstraZeneca, GSK, Boehringer, Almirall, and Janssen. The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wolf C , Brück N , Koss S , et al. Janus kinase inhibition in complement component 1 deficiency. J Allergy Clin Immunol. 2020;146(6):1439‐1442.e 5.32325142 10.1016/j.jaci.2020.04.002 · doi ↗ · pubmed ↗
- 2Coss SL , Zhou D , Chua GT , et al. The Complement System and Human Autoimmune Diseases. J Autoimmun. 2023;137:102979.36535812 10.1016/j.jaut.2022.102979 PMC 10276174 · doi ↗ · pubmed ↗
- 3Triaille C , Rao NM , Rice GI , et al. Hereditary C 1q Deficiency is Associated with Type 1 Interferon‐Pathway Activation and a High Risk of Central Nervous System Inflammation. J Clin Immunol. 2024;44(8):185.39196411 10.1007/s 10875-024-01788-5PMC 11358312 · doi ↗ · pubmed ↗
- 4Albrecht J , Taylor L , Berlin JA , et al. The CLASI (Cutaneous LE Disease Area and Severity Index): an outcome instrument for cutaneous lupus erythematosus. J Invest Dermatol. 2005;125(5):889‐894.16297185 10.1111/j.0022-202X.2005.23889.x PMC 3928016 · doi ↗ · pubmed ↗
- 5Lintner KE , Wu YL , Yang Y , et al. Early Components of the Complement Classical Activation Pathway in Human Systemic Autoimmune Diseases. Front Immunol. 2016;7:36.26913032 10.3389/fimmu.2016.00036 PMC 4753731 · doi ↗ · pubmed ↗
- 6Günther C , Wolf C , Fennen L , et al. Case Report: Response of cutaneous lupus lesions in SLE to interferon receptor blockade parallels reduction of interferon score in blood. Front Immunol. 2023;14:1253279.37809086 10.3389/fimmu.2023.1253279 PMC 10551165 · doi ↗ · pubmed ↗
- 7Carter LM , Wigston Z , Laws P , Vital EM . Rapid efficacy of anifrolumab across multiple subtypes of recalcitrant cutaneous lupus erythematosus parallels changes in discrete subsets of blood transcriptomic and cellular biomarkers. Br J Dermatol. 2023;189(2):210‐218.36944572 10.1093/bjd/ljad 089 · doi ↗ · pubmed ↗
- 8Vital EM , Merrill JT , Morand EF , et al. Anifrolumab efficacy and safety by type I interferon gene signature and clinical subgroups in patients with SLE: post hoc analysis of pooled data from two phase III trials. Ann Rheum Dis. 2022;81(7):951‐961.35338035 10.1136/annrheumdis-2021-221425 PMC 9213795 · doi ↗ · pubmed ↗