Forced Duction Testing for Management of Small Orbital Floor Blowout Fractures
Jason V Djafar, Lloyd R Kopecny, Isobel Yeap, Alex Pitman, Ian C Francis

TL;DR
Forced duction testing can both diagnose and treat small orbital floor fractures by releasing trapped muscles and restoring eye movement.
Contribution
Demonstrates FDT's dual diagnostic and therapeutic utility in small orbital floor blowout fractures.
Findings
FDT successfully confirmed restricted eye movement in a patient with a small orbital floor fracture.
Immediate muscle release via FDT resolved painful restricted upgaze without surgery.
FDT may be an effective alternative to surgery in select small fracture cases.
Abstract
Forced duction testing (FDT) is a diagnostic clinical test of extraocular muscle function employed to confirm the mechanical and restrictive nature of a patient’s defective upgaze. Orbital floor blowout fractures (OFBFs) may lead to bony entrapment of the inferior orbital muscles and connective tissue, resulting in restricted vertical gaze and early or late enophthalmos. Management of OFBFs aims to restore normal ocular anatomy and physiology and may require definitive surgical intervention if there is significant entrapment and large fractures. The authors report a 19-year-old man with a small right OFBF due to a rugby football injury, who presented with painful restricted upgaze. High-resolution orbital computed tomography (CT) demonstrated minor impingement of the inferior rectus muscle by the fractured thin orbital floor bone. FDT was performed in the Emergency Department in an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
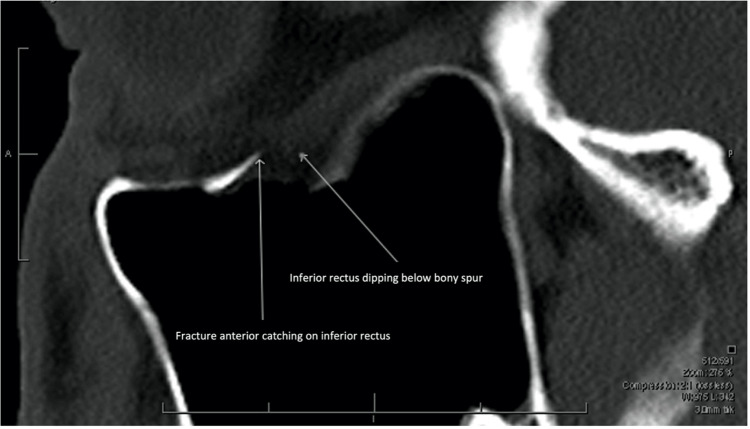 Figure 1
Figure 1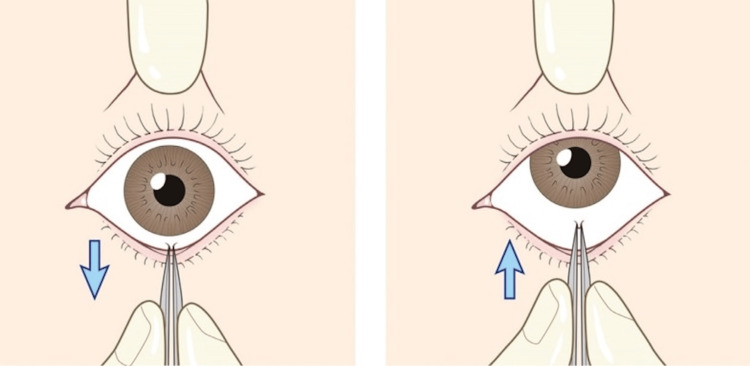 Figure 2
Figure 2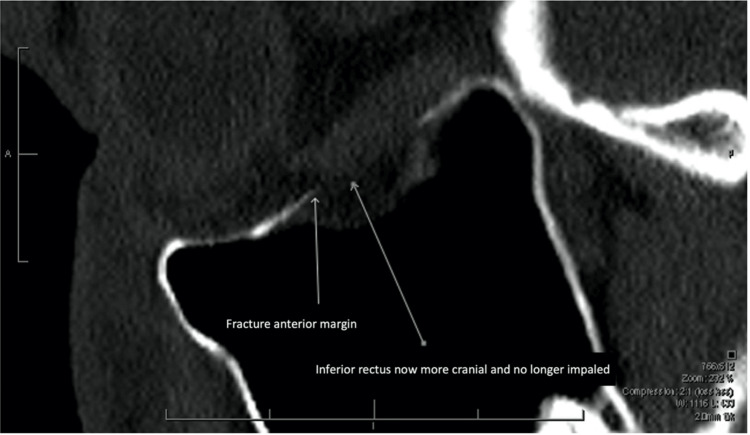 Figure 3
Figure 3| Protocol |
| Informed consent |
| Electrocardiograph (ECG) monitoring |
| Instillation of oxybuprocaine topical anaesthetic eyedrops |
| Placement of lid speculum |
| Infiltration of 2% lignocaine transconjunctivally into the insertion of the inferior rectus, using a 30-gauge needle |
| Application of toothed Adson forceps to inferior rectus insertion |
| Performance of standard Forced Duction Testing, assessing the patient’s defective elevation of the eye, and releasing the entrapped inferior rectus |
| Advantages of Forced Duction Testing | Disadvantages of Forced Duction Testing |
| Definitive and immediate re-establishment of normal eye movements | General anaesthesia is required in children. |
| Performance in an Outpatient/Emergency Department setting under local anaesthesia | Potential trauma by forced duction testing to the inferior rectus muscle insertion |
|
Avoidance of orbital floor implants for reconstruction (alloplasts, autografts)[ |
Theoretical risk of triggering the oculocardiac reflex with extraocular muscle traction (although no case reports to date in the literature)[ |
| Avoidance of common post-operative complications related to open interventiona | |
| Significant time and cost savings | |
| Operative surgery in operating theatre remains viable if the initial trial of forced duction testing for orbital floor blowout fractures fails |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Trauma and Fracture Management · Traumatic Ocular and Foreign Body Injuries · Dental Radiography and Imaging
Introduction
Orbital floor fractures were first described in 1844 [1]. The term “orbital blow-out” fracture was described by Smith and Regan in 1957 [2], referring to an orbital floor fracture caused by a sudden increase in intraorbital pressure. Initial imaging of orbital floor blowout fractures (OFBFs) was carried out using plain orbital X-rays, which were superseded with the advent of computed tomography (CT) scans [3].
The entrapment of the inferior rectus or inferior oblique muscles with their surrounding orbital connective tissues is a concerning possible complication of OFBFs. This may present as vertical diplopia, painful restriction of vertical gaze, and rarely the oculocardiac reflex. Forced duction testing (FDT) is a test of extraocular muscle restriction performed by first applying local anaesthetic to the conjunctiva and then mobilising the globe using forceps attached to the insertion of the relevant muscle [4]. In OFBF with entrapment, the examiner observes an inability to move the patient’s eye freely, reflective of the underlying globe tethering and restricted movement in this pathology. In the paediatric population, bony elasticity may cause the fractured orbital floor to snap back into position, simulating a “trapdoor” that incarcerates these muscles [5,6]. To avoid a Volkmann-like ischaemic contracture, urgent surgery is indicated [7].
Many OFBFs are not associated with entrapment and may be observed with follow-up in 1-2 weeks until orbital oedema, haemorrhage, and motor nerve palsy subside, enabling subsequent assessment of extraocular movements and enophthalmos. Indications for delayed surgery include enophthalmos greater than 2-3 mm, an orbital floor defect on CT greater than 2 cm², or one that involves 50% or more of the orbital floor surface [8]. Patients who do not meet surgical criteria after a period of observation have similar outcomes when managed conservatively [9,10].
Ophthalmological assessment is always indicated to exclude concomitant ocular trauma, which is reported in up to 75% of cases [11,12]. Richani et al. (2019) presented a series of 512 patients with orbital floor fractures, whereby 14% had severe ocular trauma and vision loss [13]. Early operative repair is contraindicated when hyphaema, retinal tears, globe perforation, or contralateral blindness is present.
Case presentation
A 19-year-old man presented to the emergency department (ED) of a tertiary referral teaching hospital in Sydney, Australia, following a right orbital injury whilst playing rugby that same day.
Vertical diplopia was present, related to defective elevation (-2/4) and depression (-1/4). The patient had severe ocular pain with upgaze of the right eye. Periorbital ecchymosis was evident. Using the Luedde proptometer [11], 3mm of right proptosis was observed (18mm right, 15mm left). Light touch sensation in the distribution of the ipsilateral infraorbital nerve was reduced. The ophthalmological examination was otherwise normal. Orbital CT demonstrated a small OFBF measuring 1.44 cm² in the mid-orbital floor. The anterior lip of the fractured bone impinged on the anteroinferior aspect of the inferior rectus muscle, with herniation of orbital fat (Figure 1).
Parasagittal CT Orbits (Bony Windows), Prior to Forced Duction Testing.Note the anterior lip of the fractured bone impinging on the anteroinferior aspect of the inferior rectus, with modest orbital fat herniation.
The corresponding author (ICF) had previously managed a similar case, where the patient’s vertical diplopia and defective eye elevation resolved with FDT. This was performed on a 28-year-old man who had sustained a punch to the orbit, resulting in radiological and clinical evidence of an OFBF. At that time, CT was not available, and a plain orbital X-ray was employed to confirm the clinical diagnosis radiologically. Using a standard diagnostic FDT, the patient’s OFBF resolved immediately and uneventfully (Figure 2) [6].
Diagram of Forced Duction Testing to Examine Extraocular Muscle Entrapment.The examiner uses forceps to grasp the anaesthetised conjunctiva overlying the attachment of the inferior rectus muscle. The examiner assesses the patient’s defective upgaze and gently attempts to release the entrapped inferior rectus muscle. (reproduced from Kim & Jeong, 2016 (6), used under the Creative Commons Non-Commercial Licence, CC BY 3.0)
Hence, with informed consent, for the current patient, FDT was performed in the ED. The indications in general for this procedure include a small OFBF (< 2 cm²), radiological evidence of bony impingement by orbital floor bone, and associated defective elevation of the patient’s affected eye. The procedure should be performed in the ED, where ECG monitoring is readily available to recognise the possibility of the oculocardiac reflex.
The authors’ protocol for Forced Duction Testing to manage small Orbital Floor Blowout Fractures (FDT-OFBF) is outlined below (Table 1).
Following FDT, there was immediate resolution of the patient’s diplopia. The patient’s defective elevation of that eye returned to near-normal and was pain-free. The patient remained comfortable throughout the procedure, without evidence of arrhythmias or haemodynamic instability. In fact, he broke out into a smile on an attempted, successful upgaze. The patient was admitted overnight to monitor for and exclude retrobulbar haemorrhage, employing standard neurological observations for pain, visual acuity, pupil reactivity, and proptosis.
By the next morning, his defective right ocular elevation had improved (-1/4), and depression had returned to normal (0/4). Repeat CT confirmed satisfactory OFBF reduction (Figure 3). After being provided with instructions for intensive eye movement exercises, the patient was discharged for outpatient follow-up.
Sagittal CT Orbits (Bony Windows), Following Forced Duction Testing for Resolution of Inferior Rectus Impingement.The inferior rectus is now more cranial and no longer impaled by the anterior margin of the fractured bone.
Seven weeks following therapeutic FDT, the patient reported no diplopia. Defective right elevation was reduced to less than -0.5/4. Infraorbital nerve sensation had returned to near normal. The patient’s proptosis had normalised as measured by Luedde proptometry (14 mm right, 15 mm left).
Discussion
This report demonstrates that FDT for OFBFs (FDT-OFBF), performed under topical and local infiltrative anaesthesia, may be used to resolve inferior orbital muscle impingement by the bones of the orbital floor. This simple, inexpensive, and minimally invasive technique may be performed in the ED where cardiac monitoring is readily available. It can represent an initial step in the conservative management of OFBFs, as opposed to immediate triaging for standard operative OFBF repair in the operating room (OR).
Suitable candidates for FDT-OFBF should include patients with small OFBFs who have radiological evidence of bony impingement of the inferior orbital muscles and connective tissue, with associated restriction in vertical eye movements. Small OFBFs have previously been described in the literature as those with an estimated fracture area between 1 and 2 cm² [14]. The authors have suggested the various advantages and disadvantages of FDT to manage extraocular muscle impingement in Table 2. FDT-OFBF avoids almost all the risks and complications of definitive surgery on OFBFs in the OR.
As plastic surgeons, ocular plastic surgeons, and maxillofacial surgeons are regularly faced with the management of OFBFs, diagnostic FDT may be an effective therapeutic option to treat selected OFBFs. Following FDT, rapid resolution of pain, diplopia, and defective ocular elevation and depression meant this patient avoided invasive surgery under general anaesthesia. If forced duction testing fails to provide symptom resolution, definitive surgery in the OR is still available.
The oculocardiac reflex (OCR) is reported to occur in 14-90% of patients undergoing strabismus surgery [16], attributed to the relatively long duration of extraocular muscle traction that occurs in strabismus surgery. Indeed, there are no reports of the OCR related to FDT, despite FDT being a relatively commonly performed procedure. By comparison, the almost instantaneous duration of FDT-OFBF renders the likelihood of the OCR almost negligible.
Trauma to the inferior rectus and inferior oblique muscles with therapeutic FDT is unlikely, since the mechanical force applied to the anaesthetised inferior rectus insertion is similar to that applied when carrying out diagnostic FDT. Indeed, there are no literature reports documenting such trauma. Finally, if impingement does not resolve with FDT-OFBF in the outpatient setting, definitive OFBF surgery in the OR is indicated and may be undertaken uneventfully.
Conclusions
In summary, FDT-OFBF offers an alternative, simple, and non-invasive management strategy for selected patients with OFBFs. FDT-OFBF may be considered as a possible and effective addition to the surgical repertoire of plastic surgeons, ocular plastic surgeons, and maxillofacial surgeons for the management of select OFBFs. When successful, FDT avoids definitive surgical management of the OFBF along with its potential associated complications. Further research, such as a prospective multicentre trial, should refine the indications for, the outcomes of, and the complications associated with FDT-OFBF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Traité Pratique Des Maladies Des Yeux Mackenzie W Paris Bibliothèque du Palais des Arts 1844 https://books.google.co.in/books?id=YL 8qk_j Wug QC&dq=Trait%C 3%A 9+Pratique+Des+Maladies+Des+Yeux:+Dusillon+1844&lr=&source=gbs_navlinks_s
- 2Blow-out fracture of the orbit: mechanism and correction of internal orbital fracture Ame Jr Oph Smith B Regan Jr WF 73373944195710.1016/0002-9394(76)90774-113487709 · doi ↗ · pubmed ↗
- 3Medical imaging: from roentgen to the digital revolution, and beyond Rambam Maimonides Med J Bercovich E Javitt MC 9201810.5041/RMMJ.10355 PMC 618600330309440 · doi ↗ · pubmed ↗
- 4Duction test Encyclopedia of Ophthalmology D’Souza NM Almarzouqi SJ Morgan ML Lee AG 12Berlin, Heidelberg Springer 2016 https://link.springer.com/rwe/10.1007/978-3-642-35951-4_1185-1
- 5Evidence-based medicine: Orbital floor fractures Plast Reconstr Surg Gart MS Gosain AK 1345135513420142541509810.1097/PRS.0000000000000719 · doi ↗ · pubmed ↗
- 6Orbital floor fracture Arch Craniofac Surg Kim HS Jeong EC 1111181720162891326710.7181/acfs.2016.17.3.111PMC 5556798 · doi ↗ · pubmed ↗
- 7Volkmann's contracture of the extraocular muscles following blowout fracture Plast Reconstr Surg Smith B Lisman RD Simonton J Della Rocca R 200216741984646314510.1097/00006534-198408000-00004 · doi ↗ · pubmed ↗
- 8Clinical recommendations for repair of isolated orbital floor fractures: an evidence-based analysis Ophthalmology Burnstine MA 12071210200210.1016/s 0161-6420(02)01057-612093637 · doi ↗ · pubmed ↗