Brevibacterium casei: A Rare Cause of Peritoneal Dialysis-Associated Peritonitis
Veerle Wijtvliet, Katrien Leyssens, Marleen Vanden Driessche, Veerle Matheeussen, Andrea Bertels

TL;DR
This paper reports a rare case of peritoneal dialysis-associated peritonitis caused by Brevibacterium casei, which was successfully treated with antibiotics.
Contribution
The paper presents a rare clinical case of peritonitis caused by Brevibacterium casei and highlights successful catheter preservation.
Findings
Brevibacterium casei caused peritoneal dialysis-associated peritonitis in a patient.
Intraperitoneal antibiotics successfully treated the infection and preserved the PD catheter.
Only four global cases of B. casei peritonitis have been reported, with catheter preservation in just one other.
Abstract
Peritonitis is an important complication of peritoneal dialysis (PD), affecting up to 40% of patients at some point of their PD treatment. Here, we describe a case of PD-associated peritonitis due to an unusual pathogen, Brevibacterium casei. The patient was treated with intraperitoneal antibiotics, successfully preserving the PD catheter. To the best of our knowledge, only four cases of peritonitis due to B. casei have been previously documented worldwide, with catheter preservation achieved in just one other case.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
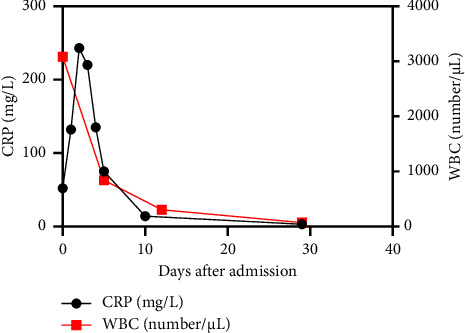 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Diphtheria, Corynebacterium, and Tetanus · Enterobacteriaceae and Cronobacter Research
1. Introduction
Peritonitis remains an important complication of peritoneal dialysis (PD), frequently leading to a transfer to haemodialysis. It is most often caused by Gram-positive bacteria, accounting for 45%–65% of the cases [1]. Here, we describe a case of PD-associated peritonitis due to an unusual pathogen, Brevibacterium casei, a Gram-positive coryneform bacterium identified through matrix-assisted laser desorption/ionisation time-of-flight (MALDI TOF) and confirmed by 16S ribosomal RNA (16S rRNA) gene sequencing. To the best of our knowledge, only four cases of peritonitis due to B. casei have been previously documented worldwide [2–5].
2. Case Report
A 62-year old Caucasian male on PD was admitted to the emergency department because of increasing abdominal pain since five days. His medical history included Type 2 diabetes, without need for therapy, and epilepsy, for which he was taking levetiracetam as maintenance treatment. The patient had initiated automated peritoneal dialysis (APD) 9 months prior, following nephroureterectomy of his solitary kidney due to a pyelum carcinoma. He had experienced no previous episodes of peritonitis. At the time of hospital admission, the PD prescription comprised 8.5 h of overnight continuous peritoneal dialysis (OCPD) with four cycles, each with a 3-L fill volume of physioneal 1.36/2.27% dextrose bags (tidal at 80%), followed by two cycles of 2.5 L extraneal during the day. Clinical examination revealed a hemodynamically stable patient with a subfebrile body temperature following antipyretic therapy (paracetamol 1 g), along with diffuse abdominal tenderness. There were no signs of exit site or tunnel infection, and the patient denied any manipulation error. Laboratory results were significant for leucocytosis (15.1 × 10^3^/μL) with neutrophilia (13.2 × 10^3^/μL) and C-reactive protein (CRP) of 52 mg/L. The PD effluent was cloudy with a white blood cell count (WBC) of 3085/μL (77.1% polymorphonuclear [PMNs] leukocytes), confirming the diagnosis of peritonitis. After taking two sets of blood culture bottles and inoculating PD fluid in one set as well (BactAlert FA and FN plus, bioMérieux), antibiotic treatment was started with intraperitoneal cefazolin (1.8 g, compatible with 20 mg/kg body weight) and ceftazidime (3 g), along with antifungal prophylaxis (fluconazole 100 mg daily). After one day, the patient's clinical condition further deteriorated with the development of hypotension (96/69 mmHg), increasing abdominal pain, and fever up to 38.6°C. Moreover, after 19.7 h of incubation, the aerobic bottle with PD effluent flagged positive, showing Gram-positive rods with a coryneform shape on Gram stain, and antibiotic therapy was switched to vancomycin intraperitoneally. Subsequent culture showed growth of grey-whitish colonies with a shiny surface, identified as B. casei by MALDI-TOF (Bruker), with a maximum log score of 2.4. The identification was later confirmed by Sanger sequencing targeting 500 base pairs of the 16S rRNA gene. Antibiotic susceptibility testing was performed according to EUCAST Breakpoint tables for interpretation of minimum inhibitory concentrations (MICs) and zone diameters, Version 13.0, 2023 guidelines for Corynebacterium species [6]. Vancomycin tested sensitive by gradient diffusion test (E-test) with a MIC of 0.25 μg/mL, while penicillin tested resistant (MIC 2 μg/mL). Of note, the anaerobic bottle of PD effluent and the blood cultures remained negative during 5 days of incubation.
According to antibiotic susceptibility testing, intraperitoneal vancomycin was administered continuously for a total 3-week duration, with a target serum trough level of 15 mg/L [4]. After five days of treatment, repeat PD-effluent WBC decreased to 843/μL, and culture remained negative. Subsequent PD-effluent tests at two and four weeks post-treatment showed a further reduction in WBC to 305/μL and 73/μL (Figure 1), respectively, with both cultures remaining negative. Due to the rapid favourable clinical and biochemical improvement, removal of the PD catheter was deemed unnecessary. No relapse of PD-associated peritonitis was observed in the following 7 weeks.
3. Discussion
Peritonitis is a common complication of PD, occurring in up to 40% of patients at some point of their treatment. It is associated with considerable morbidity and can lead to membrane failure, catheter loss, transfer to haemodialysis and even death [7]. PD-associated peritonitis is most often caused by Gram-positive bacteria, responsible for 45%–65% of the cases [1]. Here, we report a case of PD-associated peritonitis due to the unusual pathogen B. casei.
B. casei are obligate aerobic, Gram-positive, catalase-producing, immotile, rod-shaped bacteria. They are commonly found in dairy products, such as raw milk or cheese, as well as on human skin. B. casei can lead to various infections, including meningitis, salpingitis, cholangitis and peritonitis [8]. Its diagnosis may be challenging, as Brevibacterium resembles diphtheroids on Gram stain [4]. While biochemical testing can aid in differentiating Brevibacterium from other organisms, 16S rRNA gene sequencing is considered the gold standard for definitive species identification [9]. Despite being sensitive to vancomycin, three cases of recurrent PD peritonitis have already been reported [2, 3, 5]. So far, in addition to our case, the PD catheter could only be salvaged in one other case (Table 1) [4].
Current treatment guidelines recommend a 2-week course of antibiotics for Gram-positive peritonitis, except 3 weeks for Staphylococcus and Enterococcus infections [7]. Based on our case and the case of Roy et al., an extended treatment duration of 3 weeks may be required for B. casei to ensure eradication and prevent relapse [4]. Most Brevibacterium isolates are susceptible to vancomycin, which remains the first-choice antibiotic. Antimicrobial resistance of more than 50% has been observed for trimethoprim/sulfamethoxazole, clindamycin and first-line beta-lactams [10].
In conclusion, when managing PD peritonitis, inoculating PD fluid in blood culture bottles is essential for accurately identifying unexpected pathogens, determining their susceptibilities and guiding tailored antibiotic therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perl J. Harel Z. Nessim S. J. Peritoneal Fluid Analysis in Peritoneal Dialysis–Associated Peritonitis JAMA 2022328212157215810.1001/jama.2022.2128936355384 · doi ↗ · pubmed ↗
- 2Althaf M. M. Abdelsalam M. S. Alsunaid M. S. Hussein M. H. Brevibacterium casei Isolated as a Cause of Relapsing Peritonitis BMJ Case Reports 20142014 p. bcr 201420361110.1136/bcr-2014-2036112-s 2.0-84898647276 PMC 396293924648477 · doi ↗ · pubmed ↗
- 3Poesen K. Meeus G. Boudewijns M. Colaert J. Doubel P. Relapsing Brevibacterium casei Peritonitis: Value of 16S r RNA Gene Sequencing in Accurate Species Identification Peritoneal Dialysis International 201232334134410.3747/pdi.2011.001792-s 2.0-8486166469822641738 PMC 3525440 · doi ↗ · pubmed ↗
- 4Roy S. Garcha A. S. Patel S. S. Rahman E. Adapa S. Brevibacterium casei Induced Peritonitis in a Patient Undergoing Continuous Cycler Peritoneal Dialysis: Case Report and Literature Review Journal of Community Hospital Internal Medicine Perspectives 2022121646710.55729/2000-9666.1012 PMC 919511635711868 · doi ↗ · pubmed ↗
- 5Roger P. M. Sichez-Com H. Ollier J. Boumezber S. Bataille S. Oral Clindamycin for Peritonitis due to Brevibacterium casei and Bacillus Cereus in Two Successive Patients Undergoing Peritoneal Dialysis JAC-Antimicrobial Resistance 20246410.1093/jacamr/dlae 128PMC 1133133839161927 · doi ↗ · pubmed ↗
- 6EUCAST Clinical Breakpoints-Breakpoints and Guidance; Version 13.0, 2023 Guidelines for Corynebacterium species 2024
- 7Li P. K.-T. Chow K. M. Cho Y. ISPD Peritonitis Guideline Recommendations: 2022 Update on Prevention and Treatment Peritoneal Dialysis International: Journal of the International Society for Peritoneal Dialysis 202242211015310.1177/0896860822108058635264029 · doi ↗ · pubmed ↗
- 8Kim R. Reboli A. C. Other Coryneform Bacteria and Rhodococci Bennett’s Principles and Practice of Infectious Diseases 2015