A Novel Variant in the BICRA Gene, Expanding the Phenotype: A Case Report
Catherine Kentros, Wendy K. Chung, Mythily Ganapathi

TL;DR
A 71-year-old woman with a rare BICRA gene variant shows expanded symptoms and long-term outcomes for this condition.
Contribution
This is the oldest reported case of a pathogenic BICRA variant, expanding the known clinical phenotype.
Findings
A novel BICRA variant (c.1910del) was identified in a patient with intellectual disabilities and psychiatric symptoms.
The case expands the known clinical features and long-term prognosis of BICRA-related disorders.
This is the first reported case of a BICRA variant in an individual over 70 years old.
Abstract
We report a 71-year-old female patient with a history of intellectual disabilities, dysmorphic features, schizoaffective disorder, bipolar type, and psychosis. Exome sequencing revealed a novel, heterozygous, predicted loss-of-function variant in the BICRA gene (NM_015711.3: c.1910del, p.[Leu637ArgfsTer87]). Heterozygous rare variants in BICRA have been associated with Coffin–Siris Syndrome 12 (CSS-12; OMIM #619325). This is the oldest patient to date with a pathogenic variant in BICRA. This case report expands the clinical phenotype associated with BICRA variants and sheds light on the long-term prognosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
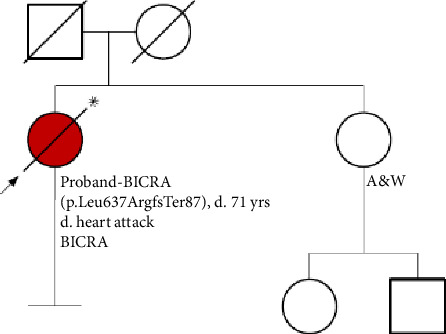 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital heart defects research · Genetics and Neurodevelopmental Disorders · Ubiquitin and proteasome pathways
Summary
- • Here, we report a novel variant in the BICRA gene associated with CSS-12.
- • Although previous reports of patients with BICRA-related disorders highlight the intellectual disability, developmental delay, and behavioral issues in patients, this report expands the adult psychiatric phenotype to include schizoaffective disorder and bipolar type with accompanying psychosis.
- • To our knowledge, a causal association between BICRA disease-causing variants and psychosis or psychotic features has not been established.
- • Patients with reported disease-causing BICRA variants are primarily pediatric, and the onset of psychotic is usually in adults.
- • Because all patients with BICRA-related disorders are younger than this patient, this case provides useful insight into the adult psychiatric phenotype.
1. Introduction
With the increased accessibility of comprehensive genomic testing, rare genetic etiologies of neurodevelopmental disorders and intellectual disability (ID) are being identified. The prevalence of ID in the general population is approximately 1%–3% [1]. In 2016, the worldwide prevalence of ID was 12.5 million [2]. So far, over 2500 genes associated with ID have been identified [3]. ID can be non-syndromic (NSID), presenting as an isolated feature, or syndromic (SID), presenting with dysmorphic features, structural anomalies, and/or multisystemic features. Psychiatric disorders are common comorbid conditions in individuals with ID. Some of the most prevalent chronic health conditions in children with ID are epilepsy, cerebral palsy, and anxiety disorder [4, 5]. With the exception of a few known recurrent conditions such as 22q11.2 deletion syndrome, the associations between monogenic conditions associated with developmental delay/ID in childhood and adult-onset psychiatric disorders such as psychosis and schizophrenia are not well understood. This is in part due to low utilization of genetic testing in certain practices such as adult psychiatric programs, and lack of long-term follow-up in adults.
Pathogenic and likely pathogenic variants in BICRA have been identified in patients with Coffin–Siris 12 [6], a cause of SID ID. Here, we report a patient with ID, adult-onset schizoaffective disorder and psychosis, with a likely pathogenic BICRA variant.
2. Materials and Methods
Informed written consent for personal data processing was obtained from patient's legal guardian. This study was approved by the Institutional Review Board of Columbia University Medical Center.
Duo exome sequencing was performed on the proband at Prevention Genetics with variant filtering and analyses as previously described [7].
3. Case Presentation
The proband is a 71-year-old female with a longstanding history of moderate to severe ID. The prenatal and early history were limited. Microcephaly was noted shortly after birth, as well as abnormal neonatal cry and colic. She developed a limited vocabulary of about 60 words. At 21 months of age, the patient underwent the Kuhlmann-Binet Intelligence test due to developmental delays. At the time, she was unable to sit without support, drink from a glass, or speak. She was found to have the mental age of an 11-month-old and an IQ score of 52, corresponding to moderate ID. The patient had several subsequent neuropsychological and IQ evaluations and scored consistently low, with limited speech and echolalia. At 18 years and 9 months of age, the Stanford-Binet intelligence test was repeated, revealing an IQ of 32. Cognitive testing was repeated at age 26, and results were similar to the previous scores in the range of severe ID. The patient was, at the time, on medication (unspecified) due to “head banging behaviors” and “tendency to act out.” She had occasional temper tantrums, staring off, completely dissociating, and fixating on her hands or her hair. Years later, these behaviors would be attributed to the patient responding to internal stimuli. No EEG, brain MRI, or metabolic results were available if they were performed.
By age 29, the patient was receiving 50 mg of thioridazine BID. She was in a sheltered workshop placement, in a loud setting. She started displaying episodes of screaming and staring at her hand and would appear to be talking to someone who was not there. These episodes would escalate to self-injurious behaviors. At the age of 35, thioridazine was discontinued following a gradual wean. Within 3 weeks of discontinuation, the emergence of outbursts and agitation was reported. A behavior support plan was developed to address this behavioral change. These outbursts occurred one to three times per month, lasting between 2 and 45 minutes. Interventions included attempts to restrain her and take her to an isolated room. Thioridazine was restarted, which resulted in the de-escalation of behavioral issues. At 35 years and 11 months, re-emergence of disruptive behaviors occurred, including disrobing and urinating on floors. The patient was evaluated by a psychiatrist, who recommended a neurological workup to rule out temporal lobe seizures, but follow-up documentation is unavailable. The patient was started on haloperidol, and thioridazine was discontinued. In the next 2 months, reports of excessive self-stimulatory behaviors were noted. The patient was thought to be allergic to haloperidol and was switched back to thioridazine. At age 38, the patient had a psychological reassessment, and her clinical picture became more indicative of psychosis; she began to refer to herself in the third person and would give commands to herself in the third person. She would often talk or yell at her hand. The patient would display mood swings that would manifest as irritability and emotional lability, as well as auditory and visual hallucinations. Negative symptoms of schizophrenia were also noted.
By age 53, the patient was started on olanzapine at bedtime, and thioridazine was discontinued. Olanzapine was noted to be highly effective in managing her behaviors, including a marked reduction in response to internal stimuli and a decrease in agitation. At 54 years, olanzapine was discontinued for unknown reasons, and agitation re-emerged. The patient was started on oxcarbazepine. The patient began talking to herself incessantly. Staff at her program noted an increase in aggression. The patient started clenching her hands into fists and demonstrated rapid eye-blinking. Divalproex sodium 500 mg BID was initiated. Oxcarbazepine was discontinued as it was deemed ineffective. A few months later, divalproex sodium was discontinued due to the emergence of manic behaviors. Olanzapine was reintroduced and aggressive episodes were significantly reduced. At age 58, the patient was taking olanzapine 10 mg QD and lorazepam 0.5 mg PRN to help with insomnia. By this time, self-injurious behaviors had subsided. Episodes of talking to herself, her hand, the ceiling, or the wall would happen occasionally, but not nearly as often as before starting olanzapine. Psychiatry notes started referencing the diagnoses of schizoaffective disorder, bipolar type, and psychosis. The patient displayed auditory hallucinations and mood swings. Prior to the start of olanzapine, the patient would also display negative symptoms of schizophrenia (monotonic speech, lack of eye contact, lack of gesturing, and social withdrawal), all of which were reduced while on olanzapine.
In her late 60s, episodes of talking to herself and responding to internal stimuli still occasionally occurred, though her psychiatric symptoms appeared to have been best managed on olanzapine. The patient died of a myocardial infarction at age 71. To our knowledge, there are no documented cardiovascular phenotypes associated with BICRA variants. As described in a meta-analysis conducted by Yu et al. [8], myocardial infarction may be linked to long-term antipsychotic use.
In addition to having many overlapping clinical features with the previously reported CSS-12 patients, this patient's case expands the adult psychiatric phenotype. The patient was notably dysmorphic. Her physical features included bilateral arm deformity, thin upper and lower lips, high hairline, epicanthal folds, bilaterally low-set ears, bulbous nasal tip, and prominent nasal bridge. Her history was notable for short stature (adult height of 4 feet 9 inches). The patient shared many of the features described in the literature (Table 1). The patient was able to state and write her full name, read basic words, identify certain colors, and match objects to pictures.
The patient had one full biological sibling (Figure 1). Her sister and both parents were developmentally appropriate. There is no notable history of psychiatric disorder, autism, developmental delay, or ID in the immediate family. The family is of European ancestry.
4. Results
Singleton exome sequencing revealed a novel, likely pathogenic, rare, loss-of-function variant in the BICRA gene (NM_015711.3: c.1910del, p.[Leu637ArgfsTer87]) in the coding exon 4 of 13. Inheritance of the variant is unknown, as the parental samples are unavailable (parents are deceased). Cases with loss of function variants downstream of this variant have been reported [9, 10]. No other genetic testing was performed.
5. Discussion
At the time of this report, 15 individuals have been published with BICRA-related disorders [10–12]. Their shared phenotypes include developmental delay, ID, autism spectrum disorder, behavioral issues, microcephaly, and dysmorphic features. Out of the 15 individuals reported, 13 were heterozygous for predicted loss-of-function variants and 2 for missense variants.
As noted by Asadauskaitė et al. and Barish et al., emotional outbursts, irritability, impulsivity, echolalia, labile moods, and oppositionality have been noted in patients with BICRA-related disorders. The psychiatric history of these patients, however, has not been followed longitudinally. The clinical findings of this case confirm the findings previously associated with BICRA-related disorders, including the cognitive phenotype, craniofacial findings, and short stature, yet further expand the psychiatric phenotype through a long life course. Besides our patient, the oldest patient reported was 28 years old and no adult-onset psychiatric illness was reported [10].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patel D. R. Cabral M. D. Ho A. Merrick J. A Clinical Primer on Intellectual Disability Translational Pediatrics 20209 S 1S 23S 3510.21037/tp.2020.02.0232206581 PMC 7082244 · doi ↗ · pubmed ↗
- 2Manickam K. Mc Clain M. R. Demmer L. A. Exome and Genome Sequencing for Pediatric Patients With Congenital Anomalies or Intellectual Disability: An Evidence-Based Clinical Guideline of the American College of Medical Genetics and Genomics (ACMG) Genetics in Medicine 202123112029203710.1038/s 41436-021-01242-634211152 · doi ↗ · pubmed ↗
- 3Maia N. Nabais SáM. J. Melo-Pires M. de Brouwer A. P. M. Jorge P. Intellectual Disability Genomics: Current State, Pitfalls and Future Challenges BMC Genomics 2021221 p. 90910.1186/s 12864-021-08227-434930158 PMC 8686650 · doi ↗ · pubmed ↗
- 4Oeseburg B. Dijkstra G. J. Groothoff J. W. Reijneveld S. A. Jansen D. E. Prevalence of Chronic Health Conditions in Children with Intellectual Disability: A Systematic Literature Review Intellectual and Developmental Disabilities 2011492598510.1352/1934-9556-49.2.592-s 2.0-7995450147121446871 · doi ↗ · pubmed ↗
- 5Gautam P. Bhatia M. S. Rathi A. Intellectual Disability and Multiple Co Morbid Psychiatric Disorders in a Child: A Case Report Journal of Clinical and Diagnostic Research: Journal of Clinical and Diagnostic Research 2014811 WD 01WD 0210.7860/JCDR/2014/9336.511025584292 PMC 4290243 · doi ↗ · pubmed ↗
- 6OMIM Coffin-Siris Syndrome 12; CSS 122024 https://www.omim.org/entry/619325
- 7Prevention Genetics P Gxome—Whole Exome Sequencing 2024 https://www.preventiongenetics.com/pgxome/rapid
- 8Yu Z. H. Jiang H. Y. Shao L. Zhou Y. Y. Shi H. Y. Ruan B. Use of Antipsychotics and Risk of Myocardial Infarction: A Systematic Review and Meta-Analysis British Journal of Clinical Pharmacology 201682362463210.1111/bcp.129852-s 2.0-8498293351927198162 PMC 5338104 · doi ↗ · pubmed ↗