Characteristics and Outcomes of Immunocompromised Patients With COVID-19 Infection Admitted to an Intensive Care Unit: A Retrospective Cohort Study
Xizi Duo, Kush Deshpande

TL;DR
This study found that being immunocompromised was not a strong predictor of death in ICU patients with COVID-19, though other factors like age and severity of illness were significant.
Contribution
The study provides new insights into the mortality risk of immunocompromised ICU patients with COVID-19 using a combination of logistic regression and MARS models.
Findings
Immunocompromised patients had higher hospital mortality (39.5%) compared to non-immunocompromised patients (14.4%).
Age, APACHE III score, vasopressor use, and single-dose vaccination were independent predictors of mortality.
The MARS model identified APACHE III score >70 as the most important variable for predicting mortality.
Abstract
Background Several studies have reported that the course of illness is different in immunocompromised and non-immunocompromised patients with COVID-19 infection. The impact of COVID-19 on immunocompromised patients is not clear due to conflicting evidence from different observational studies. Aim This study aimed to compare the characteristics and outcomes of immunocompromised and non-immunocompromised patients with COVID-19 infection admitted to an intensive care unit and to evaluate whether the immunocompromised status is associated with increased mortality. Methods We conducted this retrospective cohort study using an electronic database in St. George Hospital, a tertiary ICU in Sydney. We included all adult patients (age >16 years) admitted to the ICU with COVID-19 infection over a 33-month period (March 1, 2020, to November 30, 2022). We collected the data on demographics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
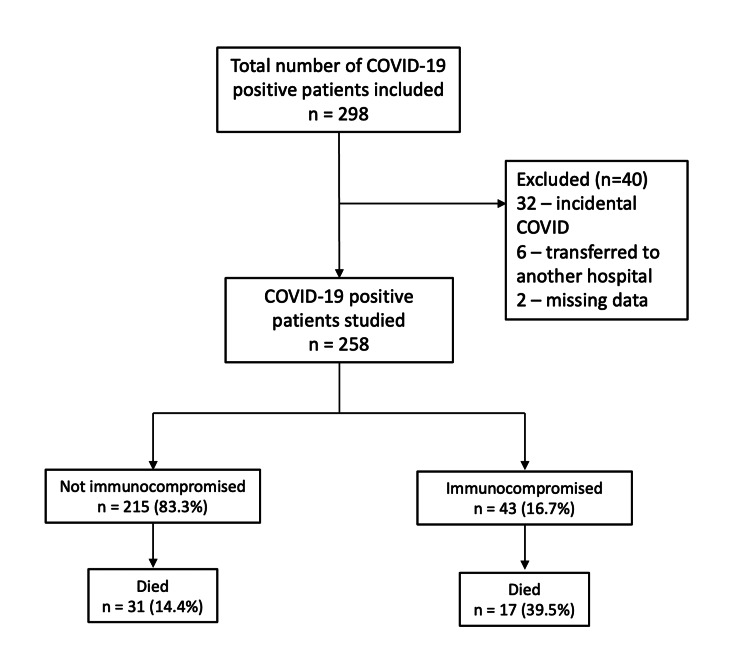 Figure 1
Figure 1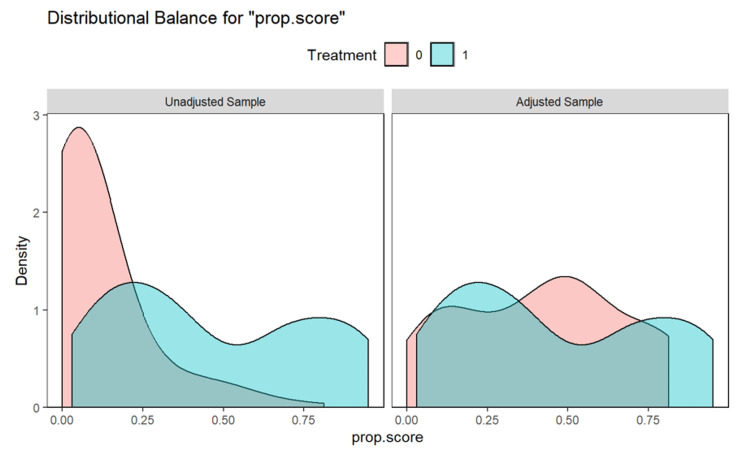 Figure 2
Figure 2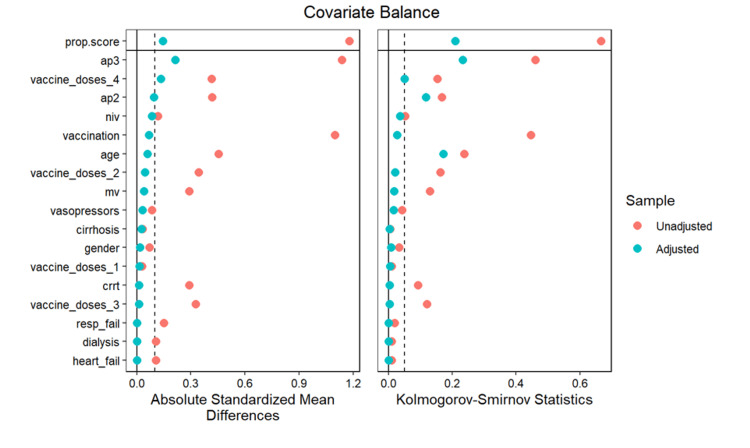 Figure 3
Figure 3| Immunosuppressive disease | Immunosuppressive therapy |
| Leukemia | Immunosuppression such as in organ transplant |
| Acquired immunodeficiency syndrome (AIDS) | Chemotherapy |
| Lymphoma | Radiation therapy |
| Severe autoimmune disease | High-dose steroids equivalent to >1.5 mg/kg m ethylprednisone for five days or more |
| Documented metastatic cancer |
| n = 258 | |
| Age, years | 60.7 ± 16.2 |
| Gender (Males) | 167 (64.7) |
| APACHE II | 14.1 ± 5.0 |
| APACHE III | 54.1 ± 21.6 |
| Vaccination | 108 (41.9) |
| Vaccine doses | |
| 0 | 150 (58.1) |
| 1 | 28 (10.9) |
| 2 | 55 (21.3) |
| 3 | 16 (6.2) |
| 4 | 9 (3.5) |
| Immune compromised | 43 (16.7) |
| Respiratory failure | 4 (1.6) |
| Heart failure | 2 (0.8) |
| Cirrhosis | 5 (1.9) |
| Dialysis | 2 (0.8) |
| Non-invasive ventilation | 55 (21.3) |
| Invasive ventilation | 100 (38.8) |
| Vasopressors | 105 (40.7) |
| CRRT | 10 (3.9) |
| MV duration, hours* | 0 (0-186) |
| ICU LOS, days* | 5.8 (3.1-12.2) |
| Hospital LOS, days* | 15.2 (8.9-24.7) |
| Hospital mortality | 48 (18.6) |
| Discharge destination | |
| Died | 48 (18.5) |
| Home | 186 (71.5) |
| Other hospital | 8 (3.1) |
| Rehabilitation ward | 18 (6.9) |
| Cause of immunocompromise | Total = 43, n (%) | Died = 17, n (%) |
| Metastatic cancer | 10 (23.3) | 4 (23.5) |
| Haematological malignancy | 9 (20.9) | 5 (29.4) |
| Stem cell transplant | 1 (2.3) | 0 |
| Solid organ transplant | 14 (32.6) | 6 (35.3) |
| AIDS | 2 (4.7) | 1 (5.9) |
| Immunosuppressive therapy for other conditions | 7 (16.3) | 1 (5.9) |
| Not immunocompromised (n = 215) | Immunocompromised (n = 43) | p-value | |
| Age | 59.8 ± 16.7 | 65.3 ± 12.2 | 0.04 |
| Gender (males) | 138 (64.2) | 29 (67.4) | 0.82 |
| APACHE II | 13.7 ± 5.0 | 15.6 ± 4.5 | 0.02 |
| APACHE III | 50.5 ± 20.1 | 72.6 ± 19.4 | <0.001 |
| Vaccination | 74 (34.4) | 34 (79.1) | <0.001 |
| Vaccine doses | <0.001 | ||
| 0 | 141 (65.6) | 9 (20.9) | |
| 1 | 23 (10.7) | 5 (11.6) | |
| 2 | 40 (18.6) | 15 (34.9) | |
| 3 | 9 (4.2) | 7 (16.3) | |
| 4 | 2 (0.9) | 7 (16.3) | |
| Respiratory failure | 4 (1.9) | 0 (0.0) | 0.82 |
| Heart failure | 2 (0.9) | 0 (0.0) | 1.0 |
| Cirrhosis | 4 (1.9) | 1 (2.3) | 1.0 |
| Dialysis | 2 (0.9) | 0 (0.0) | 1.0 |
| Non-invasive ventilation | 44 (20.5) | 11 (25.6) | 0.59 |
| Invasive ventilation | 88 (40.9) | 12 (27.9) | 0.15 |
| Vasopressors | 86 (40.0) | 19 (44.2) | 0.73 |
| CRRT | 5 (2.3) | 5 (11.6) | 0.01 |
| MV duration, hours* | 0 (0-199) | 0 (0-60.5) | 0.11 |
| ICU LOS, days* | 5.7 (3.2-12.2) | 5.8 (2.8-12.5) | 0.68 |
| Hospital LOS, days* | 14.3 (8.6-24.5) | 19.4 (11-24.9) | 0.24 |
| Hospital mortality | 31 (14.4) | 17 (39.5) | <0.001 |
| Odds ratio | 95% CI | P-value | |
| Logistic regression (univariate) | 3.88 | 1.89 - 7.97 | 0.00 |
| Logistic regression (multivariate) | 2.97 | 0.93 - 9.54 | 0.07 |
| Covariate balancing propensity score matching | 2.02 | 0.78 - 5.23 | 0.15 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Long-Term Effects of COVID-19 · COVID-19 Impact on Reproduction
Introduction
The COVID-19 pandemic has posed unprecedented challenges to global healthcare systems, with varying outcomes observed across different patient populations. Among the most vulnerable are immunocompromised individuals, who may have heightened susceptibility to severe illness and complications from viral infections. COVID-19 manifests with a wide range of symptoms, including fever, cough, shortness of breath, fatigue, and loss of taste or smell, but can escalate to more severe complications such as pneumonia, acute respiratory distress syndrome (ARDS), multi-organ failure, and death. This variability in clinical presentation underscores the complexity of the disease, particularly in individuals with altered immune responses [1].
Immunocompromised populations are heterogeneous and include individuals with malignancies, organ transplants, autoimmune diseases, or those on chronic immunosuppressive therapies. While it is widely assumed that these individuals face worse outcomes, the literature presents conflicting evidence. For instance, Li et al. found that moderately to severely immunocompromised patients had higher nasal viral loads and greater plasma viremia, suggesting more severe viral dynamics and delayed clearance [2]. Similarly, Gupta et al. showed increased 28-day mortality in ICU patients with active cancer, and Han et al. reported a 44% increased mortality risk and 49% greater risk of severe disease in cancer patients across multiple studies [3,4].
By contrast, other studies found no significant mortality difference after adjusting for confounding factors such as age and comorbidities. These inconsistencies may reflect differences in the type and degree of immunosuppression and underlying illness. For example, Cravedi et al. found that compared to reported mortality rates of the general population requiring hospitalization for COVID-19, the mortality rate of their kidney transplant recipients who needed to be hospitalized with COVID-19 was similar [5]. This highlights how certain forms of immunosuppression might not universally lead to poorer outcomes.
The management of critically ill patients in the ICU presents numerous challenges, including limited resources, staffing shortages, and the need for invasive interventions such as mechanical ventilation and renal replacement therapy. These challenges are compounded in immunocompromised patients, who may require more aggressive monitoring and tailored therapeutic approaches due to their unique clinical profiles.
Understanding the range of symptoms, complications, and specific difficulties encountered in ICU settings for these two groups is crucial for optimizing care strategies and resource allocation. This retrospective cohort study aims to compare the clinical outcomes of immunocompromised and non-immunocompromised patients admitted to our ICU during the COVID-19 pandemic. We hypothesized that the immunocompromised patients with COVID-19 would have higher mortality.
Materials and methods
Study design
We conducted a single-centre, retrospective cohort study in the ICU of St. George Hospital in Sydney using an electronic database. We included all adult patients (age >18 years) admitted to the ICU who had positive COVID-19 polymerase chain reaction (PCR) results over a 33-month period between March 1, 2020, and November 30, 2022. We excluded patients who had incomplete data due to being transferred to a different unit, as well as patients with incidental COVID-19 infection, which we defined by having no oxygen requirement or any infiltrates on chest X-ray. The records for 258 patients were reviewed, including 43 immunocompromised patients and 215 non-immunocompromised patients. We collected the data on demographics, comorbidities, severity of illness scores including Acute Physiology and Chronic Health Evaluation (APACHE) II [6] and III [7], interventions, and outcome measures including length of stay (LOS) and hospital mortality, for all patients. The primary outcome was hospital mortality. We also compared other outcomes, such as ICU length of stay, number of patients who needed mechanical ventilation and its duration, number of patients requiring vasopressors, and continuous renal replacement therapy (CRRT) in the immunocompromised and non-immunocompromised patients.
We defined the immunocompromised state using the Australian and New Zealand Intensive Care Society (ANZICS) definitions (Table 1).
Ethics statement
This study was submitted to the Human Research Ethics Committee for the South Eastern Sydney Local Health District (SESLHD) for review and was deemed not to raise any ethical risks requiring submission to an ethical review committee in accordance with NSW Health Policy.
Statistical analysis
We analysed the continuous variables using mean ± SD or median (IQR) and the categorical variables as numbers and percentages (%). To compare the distribution of characteristics and outcomes between immunocompromised and non-immunocompromised patients, we used the Chi-square test or Fisher's exact test for categorical variables and the independent-samples t-test or the non-parametric Wilcoxon Mann-Whitney U test for continuous variables.
We used a multiple logistic regression model and a multivariate adaptive regression splines (MARS) model to determine the predictors of mortality. All variables were included in the logistic regression model. Variables were selected using the "step" function from the "MASS" package in R. This method uses Akaike Information Criteria (AIC) iteratively to select the variables and avoids overfitting and multicollinearity. The MARS model was developed using the "earth" package in R. This method addresses the issues of nonlinearity and collinearity.
We used propensity score analyses [8] to check whether immunocompromised patients had higher mortality compared to non-immunocompromised patients. Covariate balancing propensity score matching was performed using the "cobalt" package in R. All variables were included in the model, and covariate balance was assessed by "absolute standardized mean differences" and "Kolmogorov-Smirnov statistics."
A p-value of <0.05 was considered statistically significant. All analyses were performed using R statistical software (version 4.2.3).
Results
The flow of participants in the study is shown in Figure 1, and their baseline characteristics are shown in Table 2. Table 3 shows the underlying conditions resulting in an immunocompromised state. A total of 258 patients (mean age: 61 ± 16 years; males: 65%) admitted to the ICU with COVID-19 were included in this study. Among them, 43 (16.7%) were immunocompromised. The immunocompromised patients were older (mean age: 65.3 ± 12.2 vs. 59.8 ± 16.7 years, p = 0.04), had higher APACHE II (15.6 ± 4.5 vs. 13.7 ± 5.0, p = 0.02) and APACHE III scores (72.6 ± 19.4 vs. 50.5 ± 20.1, p < 0.001), and had higher vaccination rate (79.1% vs. 34.4%, p < 0.001). Table 4 shows the baseline characteristics stratified by the immune status.
Participant flowchart
The hospital mortality rate was significantly higher in immunocompromised patients (39.5% vs. 14.4%, p < 0.001). Independent predictors of mortality identified through multivariate logistic regression included age (OR 1.05, 95% CI 1.01-1.1, p = 0.02), APACHE III score (OR 1.05, 95% CI 1.02-1.09, p < 0.001), vasopressor use (OR 6.7, 95% CI 2.6-17.2, p < 0.001), and single-dose vaccination (OR 3.76, 95% CI 1.19-11.9, p = 0.02). The MARS model identified APACHE III (score > 70) as the most significant predictor of hospital mortality.
Figures 2-3 show the matching between the immunocompromised and non-immunocompromised groups using the covariate balancing propensity score method.
Covariate balancing propensity score
Covariate balancing propensity score by absolute standardized mean differences and Kolmogorov-Smirnov statistics
Covariate balancing propensity score
The covariate balancing propensity score analysis did not reveal a statistically significant increase in the risk of hospital mortality for immunocompromised patients (OR 2.02, 95% CI 0.78-5.23, p = 0.14), although there was a trend toward higher mortality (Table 5).
Discussion
Statement of principal findings
This study found that immunocompromised patients admitted to the ICU with COVID-19 had higher severity of illness scores and a significantly increased crude hospital mortality rate compared to non-immunocompromised patients. However, when adjusting for confounding factors using multivariate regression and propensity score methods, immunocompromised status was not identified as an independent predictor of hospital mortality. Instead, age, severity of illness (APACHE III score), vasopressor use, and single-dose vaccination were significant predictors of hospital mortality.
Comparison with similar studies
Previous studies have presented mixed results regarding the impact of immunocompromise on COVID-19 outcomes. Some meta-analyses, such as Belsky et al. [1], found that only solid organ transplant patients had a significantly increased risk of hospital mortality compared to non-immunocompromised patients, whereas cancer and hematopoietic cell transplant patients did not show statistically significant differences. Similarly, Gatti et al. and Raja et al. found no statistically significant difference in mortality for solid organ transplant patients compared to non-immunocompromised patients, suggesting that immunocompromised status alone may not be a determinant of worse outcomes [9,10].
Conversely, retrospective cohort studies, such as those by Suárez-García et al. in Spain and Baek et al. in Korea, reported significantly higher mortality in immunocompromised patients compared to their non-immunocompromised counterparts [11,12]. Specifically, Suárez-García et al. found an adjusted odds ratio (aOR) of 1.6 (95% CI 1.43-1.79), with transplant patients showing the highest risk [8]. Likewise, the WHO ISARIC CCP-UK study found an increased risk of mortality among immunocompromised patients (aOR 1.44, 95% CI 1.39-1.50, p < 0.001) [13].
By contrast, a large retrospective cohort study using the National COVID Cohort Collaborative found no significant association between immunosuppression and in-hospital mortality after propensity score matching, except for patients receiving rituximab for rheumatologic or cancer-related conditions [14]. Andersen et al. similarly found that rituximab had worse outcomes; however, not all immunosuppressive medications had a significant association between immunosuppression and worse outcomes [15].
Our findings align more closely with studies that emphasize the importance of overall illness severity rather than immunocompromised status alone. The strong influence of APACHE III scores and vasopressor use on hospital mortality in our study suggests that clinical factors beyond immune status may play a more significant role in predicting outcomes in critically ill COVID-19 patients.
The heterogeneity of immunocompromised states remains a critical challenge in interpretation. In our study, subgroup numbers were too small to differentiate between transplant recipients, autoimmune conditions, and malignancy.
Importantly, a meta-analysis by Han et al. emphasized cancer as a distinct high-risk group, but did not find consistent outcome differences in other forms of immunosuppression [4]. This supports the idea that future studies should stratify by immunosuppression type and intensity, ideally in multicenter or pooled cohorts.
Our study not only contributes to the growing body of literature on COVID-19 but also highlights the need for tailored approaches in managing critically ill patients with varying immune profiles, ultimately aiming to improve outcomes for the most at-risk populations.
Strengths and limitations
One of the strengths of this study is the well-defined cohort with accurate and comprehensive data collection. The use of robust statistical analysis methods, including logistic regression, MARS modelling, and propensity score analysis, strengthens the reliability of the findings by accounting for potential confounders. In addition, this study contributes valuable data from a tertiary ICU in Australia, a region where limited research has been published on immunocompromised COVID-19 patients. The study’s high internal validity is another key strength, enhancing the credibility of the results.
However, there are several limitations. The single-center, retrospective study design limits the generalizability of the findings. The small sample size, particularly the limited number of immunocompromised patients and their subgroups, restricts the ability to draw definitive conclusions about specific immunocompromised conditions. Patients who were transferred to other hospitals were not included, which may have introduced selection bias. Another limitation is the lack of data on different SARS-CoV-2 variants, which may have influenced disease severity and outcomes. Additionally, immunocompromised patients constitute a heterogeneous group with varying degrees of immune dysfunction, which may impact outcomes.
Implications for future research
Given these findings and the conflicting evidence in the literature, a larger multicentre study is needed to further evaluate the impact of immunocompromised status on COVID-19 ICU outcomes. Future research should also consider subgroup analyses based on specific causes of immunosuppression, as different immunocompromised conditions may have varying risks and prognoses.
Conclusions
This study did not find immunocompromised status to be an independent predictor of mortality in our ICU cohort of COVID-19 patients. While the mortality rate was higher among immunocompromised individuals in unadjusted analyses, this association did not hold in multivariate analyses or propensity score assessments. There is also a need for subgroups of immunocompromised patients to be studied separately. The immunocompromised patients are a heterogeneous group and have varying degrees of mortality with COVID-19. Further studies with larger sample sizes and multi-center designs are necessary to explore these findings in greater detail.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1COVID-19 in immunocompromised patients: a systematic review of cancer, hematopoietic cell and solid organ transplant patients J Infect Belsky JA Tullius BP Lamb MG Sayegh R Stanek JR Auletta JJ 3293388220213354962410.1016/j.jinf.2021.01.022PMC 7859698 · doi ↗ · pubmed ↗
- 2Virological and clinical characteristics of immunocompromised patients with COVID- 19: a systematic review and meta-analysis Lancet Microbe Li M Ye R Wang Y 31232242023
- 3Factors associated with death in critically ill patients with coronavirus disease 2019 in the USJAMA Intern Med Gupta S Hayek SS Wang W 1436144718020203266766810.1001/jamainternmed.2020.3596 PMC 7364338 · doi ↗ · pubmed ↗
- 4Holiday ratio of hospitalization and 30-day readmission rates among cancer patients after major surgery Cancer Med Chiou LJ Chen HM Pan LF Lee CC 7437521120223490439410.1002/cam 4.4482 PMC 8817097 · doi ↗ · pubmed ↗
- 5COVID-19 and kidney transplantation: results from the TANGO International Transplant Consortium Am J Transplant Cravedi P Mothi SS Azzi Y 314031482020203264979110.1111/ajt.16185 PMC 7405285 · doi ↗ · pubmed ↗
- 6The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults Chest Knaus WA Wagner DP Draper EA 161916361001991195940610.1378/chest.100.6.1619 · doi ↗ · pubmed ↗
- 7Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients Crit Care Med Zimmerman JE Kramer AA Mc Nair DS Malila FM 129713103420061654095110.1097/01.CCM.0000215112.84523.F 0 · doi ↗ · pubmed ↗
- 8An introduction to propensity score methods for reducing the effects of confounding in observational studies Multivariate Behav Res Austin PC 3994244620112181816210.1080/00273171.2011.568786 PMC 3144483 · doi ↗ · pubmed ↗