Pneumococcal Myocarditis in an Immunocompetent Young Adult: A Case Report and Literature Review
Khalil Tritar, Souha Hannachi, Rym Abid, Riadh Battikh

TL;DR
A young adult with pneumococcal pneumonia developed myocarditis, highlighting the need for cardiac evaluation in such cases.
Contribution
This case report highlights pneumococcal myocarditis as an under-recognized complication in immunocompetent individuals.
Findings
An 18-year-old male with pneumococcal pneumonia developed myopericarditis confirmed by echocardiography and MRI.
The patient fully recovered after 14 days of intravenous antibiotics and supportive care.
The case underscores the importance of cardiac evaluation in pneumococcal infections.
Abstract
Pneumococcal myocarditis is an uncommon complication of invasive pneumococcal disease, although experimental data suggest that cardiac involvement may be more frequent than clinically recognized. We describe the case of an 18-year-old immunocompetent male who developed community-acquired pneumonia complicated by myopericarditis. Streptococcus pneumoniae was isolated from blood cultures. Transthoracic echocardiography revealed a reduced left ventricular ejection fraction (40-45%) with pericardial effusion, and cardiac MRI confirmed functional impairment without evidence of necrosis or inflammation. The patient was treated with a 14-day course of intravenous antibiotics alongside supportive care, resulting in full clinical and cardiac recovery. This case emphasizes the under-recognized risk of myocarditis in the context of pneumococcal pneumonia, underscores the importance of routine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
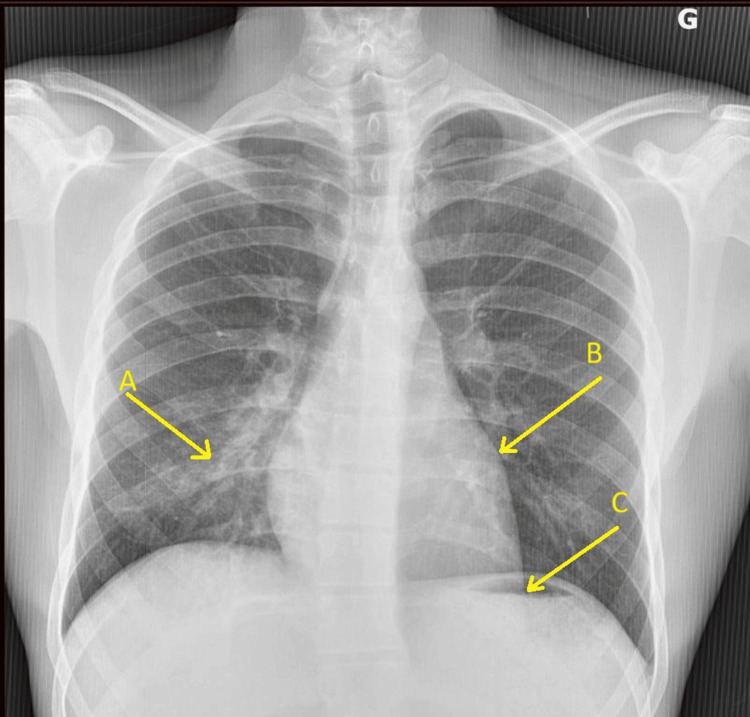 Figure 1
Figure 1| Laboratory Parameter | Patient Value | Reference Range |
| Leukocytes | 28 × 10⁹/L | 4-10 × 10⁹/L |
| Neutrophils | 26.8 × 10⁹/L | 1.8-7 × 10⁹/L |
| CRP | 249 mg/L | <5 mg/L |
| Procalcitonin | 19 ng/L | <0.5 ng/L |
| Prothrombin time | 38% | 70-100% |
| LDH | 434 U/L | 190-390 U/L |
| CPK | 638 U/L | 15-200 U/L |
| High-sensitivity troponin (day 1) | 272 ng/L | <19 ng/L |
| High-sensitivity troponin (day 2) | 210 ng/L | <19 ng/L |
| Antibiotic | MIC/Result | Interpretation |
| Penicillin G | Intermediate | Reduced susceptibility |
| Amoxicillin | Intermediate | Reduced susceptibility |
| Ceftriaxone | Susceptible | Appropriate option |
| Levofloxacin | Susceptible | Appropriate option |
| Doxycycline | Resistant | Not recommended |
| Erythromycin | Resistant | Not recommended |
| Azithromycin | Resistant | Not recommended |
| Author | Year | Age | Sex | Comorbidities | Clinical Form | LVEF (%) | Antibiotics | Duration | Outcome |
| Tritar K et al. | 2025 | 18 | M | None | CAP | 40-45 | Amox-clav + gentamicin + levofloxacin | 14 days | Favorable |
| Gandhi T et al. [ | 2008 | 42 | M | None | CAP | 15-20 | Ceftriaxone + levofloxacin | 23 days | Favorable |
| Ahmed AR et al. [ | 2017 | 52 | F | None | CAP | 40-45 | Ceftriaxone | N/A | Favorable |
| Cano CB et al. [ | 2019 | 18 | M | None | CAP | 49 | N/A | N/A | Favorable |
| Chiong YK et al. [ | 2020 | 17 | M | None | CAP | 35 | Ceftriaxone | 10 days | Favorable |
| Chang CY et al. [ | 2023 | 56 | F | ITP, splenectomy | Meningitis | N/A | Ceftriaxone | 14 days | Favorable |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Cardiac Structural Anomalies and Repair · Infective Endocarditis Diagnosis and Management
Introduction
Invasive pneumococcal disease (IPD) remains a major cause of morbidity and mortality worldwide, particularly in young children, elderly patients, and individuals with chronic comorbidities. Streptococcus pneumoniae is the most common cause of community-acquired pneumonia (CAP) and is associated with high rates of bacteremia and cardiovascular complications among hospitalized adults [1]. In addition to pneumonia, meningitis, and sepsis, pneumococcal infection can also affect the cardiovascular system through both direct and indirect mechanisms [2].
Experimental studies have demonstrated that pneumococci can translocate into the myocardium, forming microlesions and inducing cardiomyocyte necrosis [3-5]. Clinical observations further suggest that cardiac complications during pneumococcal infections, including arrhythmias, pericarditis, and myocardial dysfunction, may be under-recognized [6-8]. Myocarditis, in particular, has only rarely been reported, despite the established pathogenic potential of the organism [9-12].
We present here the case of an immunocompetent young adult with pneumococcal pneumonia complicated by myopericarditis, followed by a review of the available literature.
Case presentation
An 18-year-old immunocompetent male presented to the emergency department on the third day of a febrile illness with chills and malaise. Two days prior, he had developed right-sided chest pain with productive cough and greenish sputum. On admission, he was febrile (41°C), tachycardic (105 bpm), hypotensive (100/70 mmHg), and mildly tachypneic (20 breaths/min). Auscultation revealed right-sided crackles and a pericardial friction rub.
The electrocardiogram showed a regular sinus rhythm without conduction or repolarization abnormalities.
Laboratory tests revealed leukocytosis (28 × 10⁹/L) with neutrophilic predominance (26.8 × 10⁹/L), elevated C-reactive protein (249 mg/L), and high-sensitivity troponin (272 ng/L). Other laboratory results are summarized in Table 1.
Chest X-ray revealed right basal reticulonodular opacities and an abnormal cardiac silhouette with left heart border bulging and a subdiaphragmatic apex (Figure 1).
Chest X-ray on admission Chest X-ray showing right basal reticulonodular opacities (A) and cardiac silhouette abnormalities, including a bulging left middle arch (B) and a subdiaphragmatic apex (C).
The patient was hospitalized and started on empiric intravenous amoxicillin‑clavulanic acid (1 g/200 mg, three times daily) for CAP. Intravenous gentamicin (5 mg/kg/day) was also administered early due to initial suspicion of sepsis. Transthoracic echocardiography showed moderate global hypokinesia with a left ventricular ejection fraction (LVEF) of 40-45% and a small circumferential pericardial effusion, measuring approximately 6 mm posteriorly and 5 mm anteriorly. Blood cultures grew S. pneumoniae. Antimicrobial susceptibility testing revealed intermediate resistance to penicillin G and amoxicillin, preserved susceptibility to ceftriaxone and levofloxacin, and resistance to doxycycline, erythromycin, and azithromycin (Table 2).
Antibiotic therapy was escalated with oral levofloxacin (500 mg twice on day 1, then 500 mg daily). Cardioprotective therapy with bisoprolol (2.5 mg/day) and ramipril (2.5 mg/day) was initiated. Colchicine (1 mg/day) was started as adjunctive therapy for pericardial inflammation.
Extensive workup excluded alternative etiologies: the patient had no history of drug use, eosinophil count was normal, viral polymerase chain reactions (PCRs) including cytomegalovirus (CMV) blood and BioFire® multiplex panel from nasopharyngeal swab and sputum were negative, and serologies for human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), Parvovirus B19, and Coxsackie viruses were negative. Epstein-Barr virus (EBV) and CMV profiles indicated past infection, and autoimmune screening, including antinuclear antibody (ANA) and rheumatoid factor (RF), was negative.
Cardiac MRI performed on day 7 revealed moderate pericardial effusion, septal dyskinesia, and LVEF of 52%, without evidence of edema, hyperemia, or necrosis.
The patient defervesced by day 3 of antibiotic therapy, which was continued for 14 days. Inflammatory and cardiac biomarkers normalized, and echocardiography at three months confirmed complete recovery of cardiac function. Cardioprotective therapy was maintained for one year.
Discussion
S. pneumoniae is the leading cause of CAP and is associated with the highest mortality and cardiovascular complication rate among hospitalized adults with CAP [1]. Its ability to cause pneumonia depends on evasion of mucosal defenses through neuraminidase activity and capsule shedding [3,4]. Bacteremia occurs in 20-25% of hospitalized cases [5].
In our case, S. pneumoniae was isolated from blood cultures. The pathogen accesses the bloodstream via lymphatic invasion or transcellular passage across epithelial and endothelial cells, the latter facilitated by pneumolysin and phosphorylcholine (ChoP), which bind the platelet-activating factor receptor (PAFr). Once in circulation, it evades phagocytosis via increased capsule expression [3].
Cardiac involvement is mediated by virulence factors ChoP and CbpA (Choline-binding protein A), which facilitate pneumococcal translocation into the myocardium [3,5,6]. Once in the myocardium, pneumococci form biofilms and create intramyocardial microlesions. Resident macrophages are destroyed via necroptosis [5], leading to contractile dysfunction and cardiomyocyte necrosis [6].
Clinically evident pneumococcal myocarditis remains rare, and the true incidence is unknown due to likely underdiagnosis; only a limited number of cases have been reported in the literature [6-12]. It typically presents with chest pain, palpitations, dyspnea, or syncope, with chest pain being the most frequent symptom. One-quarter of cases are complicated forms. ECG abnormalities (90%) and elevated troponins (≥50 %) are common in myocarditis [13]. Chest X-ray may reveal cardiomegaly or pulmonary congestion [13].
In our case, chest pain was the primary symptom suggestive of myocarditis, although the patient also presented with tachycardia and hypotension related to systemic infection. The diagnosis was supported by elevated troponins and echocardiographic abnormalities. Cardiac MRI confirmed functional impairment without inflammation or necrosis. MRI is the preferred non-invasive tool for myocarditis diagnosis and is recommended in all suspected cases [13].
Endomyocardial biopsy remains the gold standard but is reserved for selected severe or atypical presentations due to procedural risk [13]. It was not indicated in our case.
Beyond antimicrobial therapy, supportive treatment was guided by both the myocardial and pericardial components of the disease. Colchicine was prescribed in accordance with current guidelines for the management of acute pericarditis, due to concomitant pericardial involvement [14]. Its role in isolated myocarditis remains uncertain, and in our case, colchicine was used specifically for the pericardial component rather than the myocardial dysfunction.
For the left ventricular dysfunction, standard heart failure therapy with an ACE inhibitor (ramipril) and a beta-blocker (bisoprolol) was initiated. Such cardioprotective agents are recommended in patients with reduced LVEF, including those with myocarditis, to improve ventricular remodeling and long-term outcomes [15].
Standard treatment for IPD includes beta-lactams. For non-severe CAP in hospitalized, immunocompetent adults, a beta-lactam-macrolide combination or fluoroquinolone monotherapy is recommended. Severe cases require combination therapy [16]. Standard treatment for infectious myocarditis consists of targeted antibiotics against the causative organism. For pneumococcal myocarditis, no specific guidelines exist regarding adjunctive therapy or exact treatment duration, and practices vary. In our case, 14 days of antibiotic therapy were administered with a good outcome.
Reported cases of pneumococcal myocarditis generally have favorable long-term outcomes (Table 3), though the true incidence may be underestimated due to subclinical or unrecognized presentations.
Conclusions
IPD carries significant morbidity and can affect multiple organ systems, including the heart. Myocarditis may complicate pneumococcal pneumonia more frequently than currently recognized, even in immunocompetent young adults. Pulmonary and cardiac symptoms often overlap, which can delay diagnosis and appropriate treatment. Early recognition through careful clinical assessment, measurement of cardiac biomarkers, and imaging, especially cardiac MRI, can guide timely intervention and prevent long-term cardiac dysfunction. Clinicians should maintain a high index of suspicion for cardiac involvement in patients with IPD to ensure optimal management and outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies P Lo S Med Corrales-Medina VF Suh KN Rose G Chirinos JA Doucette S Cameron DW Fergusson DA 08201110.1371/journal.pmed.1001048 PMC 312517621738449 · doi ↗ · pubmed ↗
- 2Cardiotoxicity during invasive pneumococcal disease Am J Respir Crit Care Med Brown AO Millett ERC Quint JK Orihuela CJ 73974519120152562964310.1164/rccm.201411-1951 PPPMC 4407487 · doi ↗ · pubmed ↗
- 3Streptococcus pneumoniae: invasion and inflammation Microbiol Spectr Loughran AJ Orihuela CJ Tuomanen EI 347201910.1128/microbiolspec.gpp 3-0004-2018 PMC 642205030873934 · doi ↗ · pubmed ↗
- 4Emerging concepts in the pathogenesis of the Streptococcus pneumoniae: from nasopharyngeal colonizer to intracellular pathogen Cell Microbiol Subramanian K Henriques-Normark B Normark S 021201910.1111/cmi.13077 PMC 689978531251447 · doi ↗ · pubmed ↗
- 5Streptococcus pneumoniae in the heart subvert the host response through biofilm-mediated resident macrophage killing P Lo S Pathog Shenoy AT Brissac T Gilley RP 013201710.1371/journal.ppat.1006582 PMC 558926328841717 · doi ↗ · pubmed ↗
- 6Pneumococcal meningitis and myocarditis in a splenectomized patient J Glob Infect Dis Chang CY 1301311520233780008210.4103/jgid.jgid_36_23PMC 10549901 · doi ↗ · pubmed ↗
- 7A peculiar case of invasive Streptococcus pneumoniae Case Rep Infect Dis Ahmed AR Townsend L Tuite H Fleming C 1530507201720172946412910.1155/2017/1530507 PMC 5804339 · doi ↗ · pubmed ↗
- 8Acute ventricular wall thickening: sepsis, thrombotic microangiopathy, or myocarditis?Case Rep Cardiol De Schryver N Hoton D Castanares-Zapatero D Hantson P 275825201520152586148310.1155/2015/275825 PMC 4377372 · doi ↗ · pubmed ↗