Silent Migration of an Intrauterine Device into the Peritoneum: A Case Report
Morris A Simwa, Satbir Karwal, Sumayyah Ibrahim, Anisha Dave, Ahmed Alsobhi, Edna Mensah, Mahmoud Hani

TL;DR
A woman's IUD silently migrated into her abdominal cavity over 11 months without causing symptoms, highlighting risks of delayed diagnosis and management.
Contribution
This case report highlights asymptomatic IUD migration and the impact of delayed care due to financial constraints.
Findings
A levonorgestrel-releasing IUD migrated into the peritoneum over 11 months without symptoms.
Delayed follow-up due to financial limitations contributed to the IUD's intraperitoneal displacement.
The device was successfully removed via laparotomy, adhering to the greater omentum.
Abstract
Uterine perforation is an uncommon but potentially adverse outcome of intrauterine device (IUD) placement. It often occurs around the time of insertion and may go unnoticed, though delayed perforation can also present months or years later. Diagnosis is typically suspected when IUD strings are not visualized on vaginal examination and confirmed by imaging demonstrating displacement, perforation, or migration. Definitive management requires device removal. We report the case of a 34-year-old woman with silent migration of a levonorgestrel-releasing IUD into the peritoneal cavity. IUD displacement was incidentally noted during a routine Papanicolaou (Pap) test six months after insertion when the strings were not visualized. A pelvic ultrasound done at that time reported an IUD embedded in the uterine wall without serosal perforation. Unfortunately, delayed follow-up, partly due to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
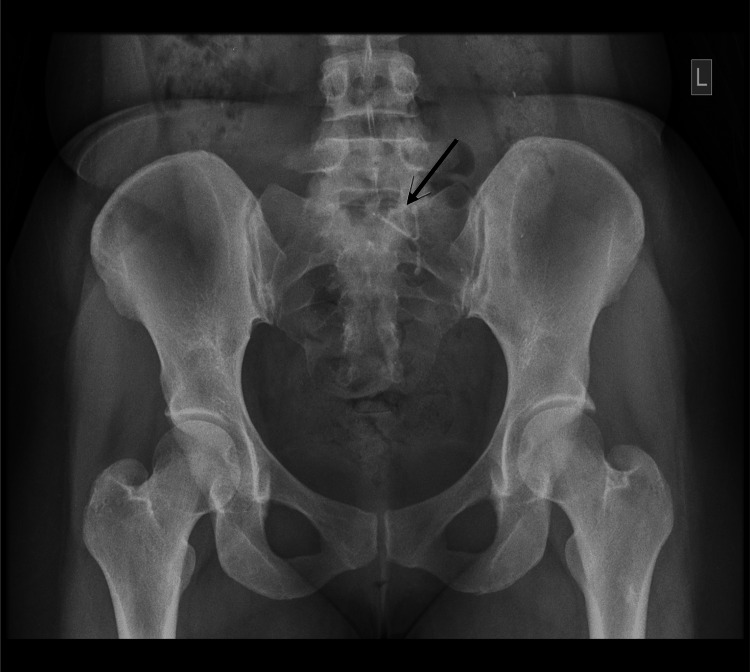 Figure 1
Figure 1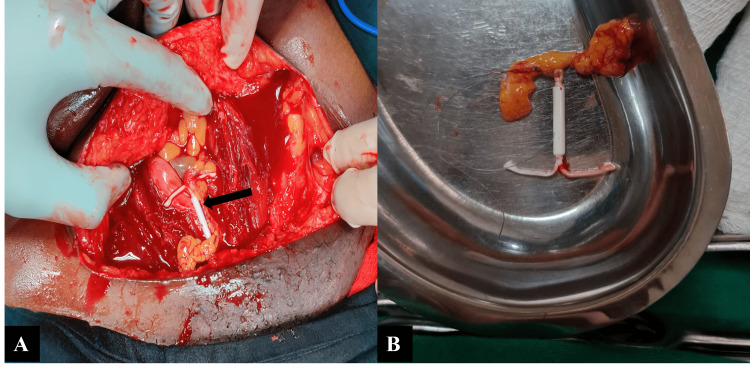 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Assisted Reproductive Technology and Twin Pregnancy · Pregnancy and Medication Impact
Introduction
Intrauterine devices (IUDs) are widely used contraceptives due to their high effectiveness, low cost, and extended duration of action [1]. Globally, approximately 14.3% of women of reproductive age use IUDs, though the prevalence varies markedly by region [2]. Complications may occur with insertion, including pain, infection, abnormal bleeding, expulsion, and uterine perforation [3]. Perforation is rare, with an incidence of 0.1%, and often goes unrecognized at the time of placement [4]. Symptoms depend on the final site of the IUD migration, which may vary from the pouch of Douglas to the mesentery, colon, or urinary bladder. Some patients present with non-specific symptoms or may be asymptomatic, delaying diagnosis and management [5]. In such patients, displacement is often first suspected when strings are absent on vaginal examination or the IUD is incidentally noted on imaging performed for other reasons. Confirmation of device migration can be achieved with ultrasound, abdominal X-ray, or computed tomography, with the latter offering the most accurate localization [5,6]. Minimally invasive techniques such as laparoscopy are the gold standard for extrauterine IUD retrieval, offering lower morbidity and shorter hospital stays, unless extensive adhesions or other complicating factors necessitate laparotomy [7]. The high upfront costs and dependence on specialized equipment often make minimally invasive approaches less feasible in resource-limited settings [8]. Our case highlights the silent migration of a levonorgestrel-releasing IUD, the risks of delayed intervention, and the impact of financial and resource limitations on timely diagnosis and optimal management.
Case presentation
A 34-year-old woman with two previous pregnancies, including one cesarean delivery seven years earlier, underwent successful insertion of a levonorgestrel-releasing 52 mg IUD (Mirena) at a general clinic. She subsequently experienced two days of colicky suprapubic pain with light spotting, which resolved spontaneously, and thereafter remained asymptomatic.
During a routine follow-up for a Papanicolaou (Pap) test at her local clinic six months later, the IUD strings were not visualized. A pelvic ultrasound at that time reported asymmetric uterine wall thickening, an embedded IUD extending from the endometrial cavity into the fundal myometrium without serosal breach, and features consistent with focal adenomyosis. Advanced imaging and intervention were not undertaken due to financial constraints related to limited medical insurance.
Eleven months after insertion, she presented to our gynecology unit with the report from her previous scan, but no images. Repeat transabdominal ultrasound demonstrated focal adenomyosis, normal ovaries bilaterally, and an extrauterine IUD now located in the peritoneum, posterior to the left ovary. The pouch of Douglas and the urinary bladder appeared normal. A pelvic X-ray confirmed the presence of the IUD within the left pelvis in an extrauterine position (Figure 1). On examination, she only had localized tenderness in the left lower abdominal quadrant on deep palpation. After discussing possible management options and the associated risks, she opted for an exploratory laparotomy, as laparoscopy was not financially feasible. Informed consent was obtained, and the procedure was carried out electively. The laparotomy was undertaken via a Pfannenstiel approach following excision of the previous cesarean section scar. Intraoperatively, the uterus was bulky but otherwise normal, with intact adnexa and a clear pouch of Douglas. The IUD was identified behind the left ovary, partially adherent to omental tissue, without involvement of bowel, bladder, or other viscera (Figure 2A). It was carefully freed through partial omental cauterization and removed without complication (Figure 2B). The recovery was uneventful, and she was discharged after two days. She remained well and stable during long-term follow-up.
Plain pelvic radiograph showing the IUD (black arrow) located in the left pelvis in an extrauterine position.IUD: intrauterine device
Intraoperative images showing the migrated IUD (black arrow)The IUD is seen adherent to the omentum on laparotomy (A) before successful retrieval (B).IUD: intrauterine device
Discussion
Uterine perforation following IUD insertion is a rare but potentially serious complication, occurring in approximately one to two per 1,000 insertions [4]. Primary perforation occurs within the first month of insertion, when the risk is highest, while secondary perforation develops later. Perforations may be partial, with the device embedded in the myometrium, or complete, in which the IUD penetrates the serosa and migrates into the peritoneal cavity or adjacent visceral organs [4,5]. Our patient’s initial ultrasound demonstrated partial perforation, which later progressed to complete perforation with extrauterine migration over five months.
Perforation and migration may be symptomatic, presenting with pelvic pain, abnormal bleeding, or missing strings; however, approximately 31% of cases are asymptomatic and identified only incidentally during imaging or examination [9]. As in our patient, asymptomatic migration poses a risk for delayed recognition and intervention, which increases the risk of visceral involvement, adhesions, and further translocation of the device.
Several risk factors for perforation have been reported, including high parity, insertion in the early postpartum period, lactation, and previous cesarean delivery [10]. Uterine pathology, such as adenomyosis or fibroids, may also alter myometrial architecture, making insertion more technically challenging and predisposing to abnormal embedment [10,11]. Our patient had both a history of cesarean section and sonographic features of adenomyosis, which likely contributed to the risk of perforation and migration. Studies show there is no clinically significant difference in the perforation risk between copper and levonorgestrel-releasing IUDs [10,12]. Ultimately, operator experience, uterine anatomy, and timing of insertion remain key determinants for uterine perforation [4].
The final location of migrated IUDs varies. While the intestine and bladder are frequent sites, with incidences of 32% and 24%, respectively, omental migration occurs in approximately 12% of cases [5,13-15]. Our case is unusual in that the IUD was found posterior to the left adnexa, adherent to the omentum, without injury to pelvic or abdominal viscera.
Management of migrated IUDs depends on location, patient symptoms, and available resources. Minimally invasive techniques such as laparoscopy or hysteroscopy are the gold standard, as they are associated with shorter hospital stays and fewer postoperative complications [7,16,17]. Laparotomy is typically reserved for cases with complex visceral involvement, dense adhesions, or where laparoscopy is unavailable [16]. In resource-limited settings such as ours, financial constraints and limited insurance coverage delayed diagnosis and ruled out laparoscopy, leaving laparotomy as the only practical option [18]. Despite these limitations, retrieval was successful, and recovery was uneventful.
Conclusions
Uterine perforation is a serious complication of IUD insertion that may remain undetected, particularly in asymptomatic patients. This case underscores the importance of prompt evaluation when retrieval strings are not visualized and highlights how uterine pathology and prior cesarean section may predispose to device displacement. Awareness of the potential for silent migration is crucial, emphasizing the need for clinical vigilance and a low threshold for imaging in high-risk patients to facilitate early detection and optimal management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The intrauterine device and the intrauterine system Best Pract Res Clin Obstet Gynaecol Stephen Searle E 8078242820142494760010.1016/j.bpobgyn.2014.05.004 · doi ↗ · pubmed ↗
- 2Worldwide use of intrauterine contraception: a review Contraception Buhling KJ Zite NB Lotke P Black K 1621738920142436930010.1016/j.contraception.2013.11.011 · doi ↗ · pubmed ↗
- 3Risk factors of uterine perforation when using contraceptive intrauterine devices BMC Womens Health Tabatabaei F Hosseini ST Hakimi P Vejdani R Khademi B 5382420243933432410.1186/s 12905-024-03298-3PMC 11428400 · doi ↗ · pubmed ↗
- 4Intrauterine devices and risk of uterine perforation: current perspectives Open Access J Contracept Rowlands S Oloto E Horwell DH 1932720162938693410.2147/OAJC.S 85546 PMC 5683155 · doi ↗ · pubmed ↗
- 5Migration of intra-uterine devices Open Access J Contracept Verstraeten V Vossaert K Van den Bosch T 41471520243849545110.2147/OAJC.S 458156 PMC 10944303 · doi ↗ · pubmed ↗
- 6Migration of intrauterine devices: radiologic findings and implications for patient care Radiographics Boortz HE Margolis DJ Ragavendra N Patel MK Kadell BM 3353523220122241193610.1148/rg.322115068 · doi ↗ · pubmed ↗
- 7Laparoscopic removal of an intra-abdominal intrauterine device: case and systematic review Contraception Gill RS Mok D Hudson M Shi X Birch DW Karmali S 15188520122206780110.1016/j.contraception.2011.04.015 · doi ↗ · pubmed ↗
- 8Global utilization of minimally invasive surgery: practice and challenges J Surg Res Mc Ginnis OC Wesonga AS Amano H 19820931320254067479510.1016/j.jss.2025.06.024PMC 12326319 · doi ↗ · pubmed ↗