Adherence to the Colombian guideline on congenital toxoplasmosis
Sara Correa-Pérez, Mauricio Daniel Carrascal-Petro, Catalina Arango-Ferreira, Claudia Patricia Beltrán-Arroyave, Javier Mauricio Sierra-Abaunza

TL;DR
This study assessed how well two hospitals in Medellin followed the Colombian guidelines for diagnosing and treating congenital and gestational toxoplasmosis between 2016 and 2020.
Contribution
The study provides the first evaluation of adherence to the Colombian clinical guidelines for congenital and gestational toxoplasmosis in a real-world setting.
Findings
Adherence to the guidelines varied, with high adherence observed in treating congenital toxoplasmosis (96.7%).
Only 85.4% of cases included the recommended serology tests for gestational toxoplasmosis.
Barriers to adherence included limited dissemination of guidelines and challenges in accessing diagnostic tools.
Abstract
Congenital toxoplasmosis is associated with high morbidity and mortality in the neonatal period. Despite the existence of a Colombian clinical practice guideline for the diagnosis and treatment of gestational and congenital toxoplasmosis, adherence to its recommendations remains unknown. To evaluate adherence to the Colombian clinical practice guidelines of congenital and gestational toxoplasmosis in two hospitals in Medellin during 2016-2020. We conducted a descriptive study in children under one year of age with suspected or confirmed congenital toxoplasmosis, treated at two hospitals in Medellin between 2016 and 2020. We used proportion measures to assess adherence to the clinical practice guidelines recommendations. Two hundred and forty-seven children were included; 17% had a confirmed congenital toxoplasmosis diagnosis. Adherence to the different clinical practice guidelines…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
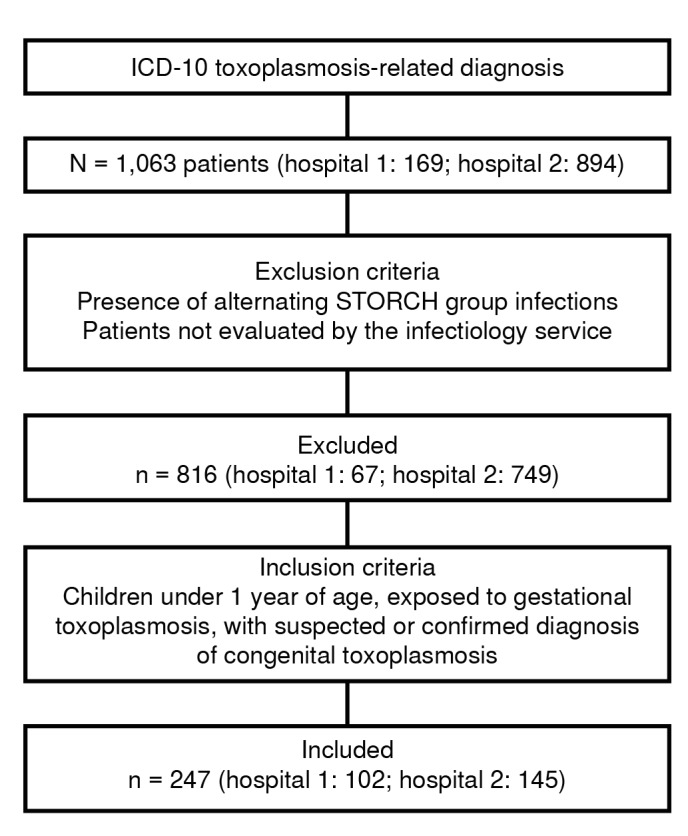 Figure 1
Figure 1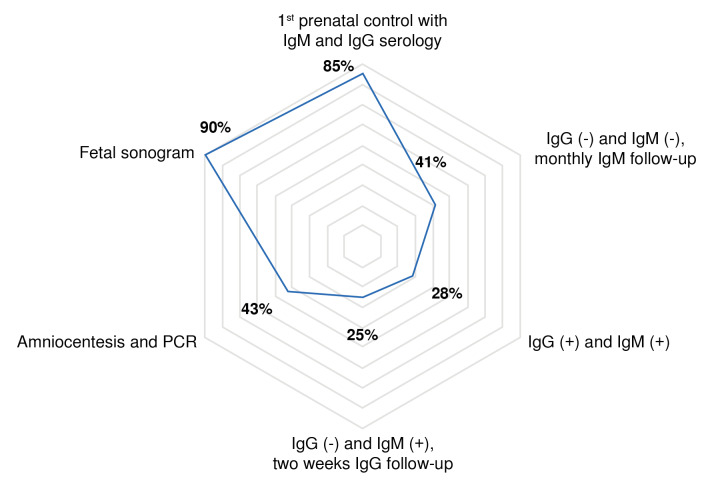 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsToxoplasma gondii Research Studies · Rabies epidemiology and control · Viral Infections and Vectors
Toxoplasmosis is a zoonotic disease caused by the parasite Toxoplasma gondii, with variable global prevalence (40-50%), depending on climate conditions and risk factors such as exposure to cat feces, raw or non-processed meats, uncooked vegetables, untreated water, or residence in rural areas 1^,^2. A higher infection burden is present in low-income countries, with a reported overall prevalence of 47.1% in Colombia 3.
Gestational toxoplasmosis is generally asymptomatic, but its screening is required due to the severity of congenital infection, which is responsible for almost 65% of the estimated 1.9 million disability-adjusted life years (DALY) 4.
In Colombia, more than half of pregnant women (50-60%) have IgG antibodies against toxoplasmosis, indicating high exposure and circulation within the country 5. The rate of mother-to-child transmission varies according to the trimester of maternal primary infection and the absence of gestational toxoplasmosis treatment 6.
Congenital toxoplasmosis has a global incidence ranging from 0.5 to 3.4 per 1,000 live births 5^,^7. In Colombia, the estimated incidence is 2-10 per 1,000 live births 8^,^9. This condition is a multisystemic disease with a high morbidity and mortality burden during the perinatal period, causing prematurity, hearing impairments, chorioretinitis, hydrocephalus, and neurological sequelae, among others 4^,^8. Ocular toxoplasmosis is the second leading cause worldwide of congenital blindness, with up to 75% of untreated neonates developing chorioretinitis and up to 50% experiencing long-term neurological sequelae 4^,^10^,^11. However, subclinical disease in neonates occurs in 75% of cases, with symptoms that may manifest many years later 4.
Several strategies have been found to reduce mother-to-child toxoplasmosis transmission. Primary prevention includes education on risk factors, and serological and follow-up screenings through pregnancy. Secondary prevention involves timely diagnosis and treatment of gestational toxoplasmosis, which can reduce vertical transmission by up to six-fold 12. Finally, proper interpretation of neonatal studies is necessary 2.
From this evidence-based approach, the Colombian clinical practice guideline was established in 2013. This guideline has good methodological quality and applicability, as demonstrated in a study comparing international guidelines on gestational and congenital toxoplasmosis 13. However, information on adherence and impact of these recommendations remains limited, as reported in a recent literature review in the country 14.
The objective of this study was to evaluate adherence to the Colombian clinical practice guideline for the diagnosis and treatment of gestational and congenital toxoplasmosis, to describe perinatal care practices, and to identify strengths and weaknesses in the management of the mother-infant dyad at two high-complexity neonatal care institutions in Medellin.
Materials and methods
We conducted a descriptive cohort study classified as "no risk" according to Resolution 8430 of 1993 from the Ministerio de Salud of Colombia. It was approved by the Comité de Ética of the Universidad de Antioquia and both participating hospitals. Patients were selected from medical records that reported the corresponding International Classification of Diseases, 10^th^ revision (ICD-10) diagnostic codes related to gestational or congenital toxoplasmosis.
We included infants under twelve months of age with suspected or confirmed congenital toxoplasmosis, treated after birth or during outpatient follow-up at two referral hospitals in Medellin between 2016 and 2020. The sample was convenience-based and included those who met the eligibility criteria during the study period. We excluded patients not evaluated by the pediatric infectious disease service. Electronic medical records served as the primary data source. Data collection forms included sociodemographic, clinical, and other variables required to evaluate adherence to the clinical practice guideline 2.
Categorical variables were analyzed using relative and absolute frequencies. For quantitative variables, normality was assessed using the Shapiro-Wilk test. For normally distributed variables, we estimated means and standard deviation; otherwise, medians and interquartile ranges (25-75%) were calculated.
Data was analyzed according to the clinical practice guideline recommendations. Maternal serological screening with initial IgG and IgM was used to determine the applicability of the recommendation for each clinical scenario 2:
- Susceptibility to primary infection is defined by negative IgM and IgG serology.
- Acute infection (seroconversion) is detected by positive IgM in previously seronegative individuals, or positive IgM and negative IgG, followed by IgG seroconversion after two weeks.
- Recent infection is indicated by IgM and IgG positivity, low IgG avidity test before 16 weeks of gestation, or positive IgA after 16 weeks, and
- Chronic infection is confirmed by initial negative IgM and positive IgG, or positive IgM and IgG with high IgG avidity test or negative IgA.
Adherence to recommendations was evaluated using the specific indicators proposed in the same clinical practice guideline 2. For other recommendations, relative frequencies were estimated for each clinical scenario.
Results
A total of 247 patients were included (figure 1). Sociodemographic, clinical, and serological data of the included patients are shown in table 1. Adherence to the clinical practice guideline recommendations varied depending on the clinical scenario, as described in table 2. No primary prevention measures for gestational toxoplasmosis were found in the medical records.
Figure 1. Recruitment flowchart of patients with suspected or confirmed congenital toxoplasmosis in two tertiary-level hospitals in Medellin, ColombiaICD-10: International Statistical Classification of Diseases
Table 1. Sociodemographic, clinical, and serological characteristics (N = 247)Variable n%Pregnant individuals With prenatal care24699.6Prenatal care entry (trimester)
1^st^14458.52nd5722.33^rd^166.3Number of prenatal visits 7(5-8)Toxoplasma gondii transmission risk factors* 7430Initial maternal serological screening IgG (-), IgM (-)4116.6IgG (+), IgM (+)15261.5IgG (+), IgM (-)104.0IgG (-), IgM (+)83.2IgG or IgM with missing or indeterminate data3614.6Newborns
Female 11446.2Gestational age Preterm 4317.4Term 18173.3Missing data 239.3Low birth weight (n = 222) 5524.8Social security 23996.8* Median (IQR)** Exposure to cat feces, raw or unprocessed meats, or unwashed vegetables; residence in rural areas; lack of access to safe drinking water; gardening activities
Table 2. Adherence to the clinical practice guideline recommendationsRecommendation PerformedIndicatedAdherence(n)(n)(%)Prevention and diagnosis of gestational toxoplasmosis Recommendations on maternal risk factors02470Baseline IgM and IgG serology during the first prenatal control21124785.4Monthly IgM follow-up (seronegative mothers)174141.5Positive IgG and IgM4114428.5IgG avidity test (before the 16th week)308933.7IgA (after the 16^th^ week)*115520Negative IgG and positive IgM: two weeks IgG follow-up2825Fetal toxoplasmosis Amniocentesis and PCR in the second trimester307042.9Positive IgG and IgM in the first trimester; low-IgG avidity151978.9Positive IgG and IgM in the second or third trimester; positive IgA060Seroconversion154533.3Fetal ultrasound22224789.9Gestational toxoplasmosis Spiramycin558068.8Positive IgG and IgM in the first trimester; low IgG avidity171989.5Positive IgG and IgM in the second or third trimester; positive IgA5683.3IgM seroconversion335560Congenital toxoplasmosis treatment Pyrimethamine + sulfadiazine + folinic acid121675Positive amniotic fluid PCR1010100Central nervous system ultrasound abnormalities61060Congenital toxoplasmosis diagnosis IgG, IgM, and IgA testing in newborns with suspected infection12524750.6Western blot in newborn with positive IgG and negative IgA and IgM0850.0IgG follow-up in newborn with negative results in all three tests (IgM, IgA, and IgG detected by Western blot)128514.1Congenital toxoplasmosis Pyrimethamine + sulfadiazine + folinic acid or alternative regimen414297.6 Of 152 patients, 8 had positive IgG and IgM, and unknown time of admission.** Patients with IgM and IgG positive before the 16^th^ gestational week, with indication of avidity test*** Patients with IgM and IgG positive after week the 16^th^ gestational week, with indication of IgA**** Alternative regime: clindamycin, sulfadoxine, or azithromycin in combination with pyrimethamine + folinic acidIgG: Immunoglobulin G; IgM: Immunoglobulin M; IgA: Immunoglobulin A; PCR: Polymerase chain reaction
In compliance with the guidelines, 30.2% (13/43) of IgA tests were performed after week 16, of which six were positive for gestational toxoplasmosis. Additionally, 69.7% (30/43) underwent IgG avidity testing. Upon admission, two of the eight pregnant women with negative IgG and positive IgM had an adequate follow-up. Both seroconverted IgG at two weeks, confirming recent exposure. Subsequently, their two neonates underwent confirmatory testing, including positive cerebrospinal fluid PCR and IgM, and presented central nervous system manifestations.
Amniocentesis was performed on 56 patients. Toxoplasma gondii DNA was detected by PCR in 10 (17.8%) samples, while 26 (46.4%) had no clear indication according to the clinical practice guideline. Unfortunately, no details on the PCR test were available.
Of the 222 gestational ultrasounds, 43 (19.3%) had abnormal findings. The most frequent were intrauterine growth restriction (n = 29; 13%), ventriculomegaly (n = 5; 2.2%), and brain calcifications (n = 4; 1.8%). Figure 2 displays the adherence percentages to the clinical guideline recommendations for the serological parameters for the diagnosis of gestational toxoplasmosis.
Figure 2. Adherence to diagnostic recommendations for gestational toxoplasmosisPCR: Polymerase chain reaction
Spiramycin was prescribed to 162 patients, of whom 80 (52.4%) met the clinical criteria for its use. Among those treated, 108 patients received an adequate dose, and 62 (38.2%) initiated treatment opportunely, within four weeks of diagnosis. Causes of inadequate spiramycin treatment included inconclusive diagnosis (n = 12), administrative reasons (n = 7), incomplete treatment duration (n = 7), and patient refusal (n = 1). Seventy-nine patients received spiramycin without a clear indication.
Fifteen pregnant women received fetal toxoplasmosis treatment; 10 had a positive amniotic fluid PCR, two had fetal ultrasound abnormalities related to the central nervous system (calcifications), and three had unidentifiable indications. Of the 162 children whose mothers received spiramycin, 21 (12.9%) had suggestive symptoms of congenital toxoplasmosis either in the central nervous system or the retina. In contrast, 24 (28.2%) out of 85 patients whose mothers did not receive treatment developed clinical manifestations.
Postnatal diagnosis of congenital toxoplasmosis was confirmed in 42 patients (17%). Seroconversion occurred in 3 patients during the first trimester, 11 during the second, and 11 during the third one; in 12 cases, the trimester of infection could not be identified. Five neonates were diagnosed based on their clinical manifestations, all born to mothers with poor prenatal serological monitoring or follow-up.
The diagnostic methods included: positive IgM in 22 (52.4%) patients, positive IgA in 2 (4.8%) patients, positive cerebrospinal fluid PCR in 8 (19%) patients, elevated IgG associated with clinical symptoms and a history of gestational toxoplasmosis in 2 (4.8%) patients, and two or more confirmatory tests for congenital toxoplasmosis in 8 (19%) patients. Physical examination and other diagnostic aids revealed abnormalities in 34 (80.9%) infants, as described in table 3.
Table 3. Clinical and laboratory manifestations of congenital toxoplasmosis (N = 42)Manifestations n%Neurological 2866.7 Calcifications1228.6Hypotonia, seizures1023.8Hydrocephalus37.1Microcephaly24.8Ophthalmological 2559.5 Chorioretinitis1126.2Retinal hemorrhages24.8Inactive lesions511.9Hematological 511.9 Thrombocytopenia49.5Anemia12.4Leukocytosis00.0Hepatic 1228.6 Impaired liver function 921.4Hepatomegaly 24.8Asymptomatic 819.1
Among the 34 children with central nervous system or retinal manifestations, 12 (35.2%) were born to mothers who had received spiramycin treatment. Of those with confirmed congenital toxoplasmosis, 11 (26.1%) received pyrimethamine/sulfadoxine/folinic acid during pregnancy.
Six (24.3%) patients were exposed to T. gondii during pregnancy and developed clinical symptoms suggestive of infection; however, no paraclinical confirmation was performed. All of them received treatment.
Cerebrospinal fluid samples were ordered for 73 newborns (29.6%) and collected on 69 (27.9%). Analysis showed abnormal results in 23 cases (33%). Out of the 51 (69.8%) PCR samples, 8 (15.6%) were positive for T. gondii. Brain imaging was performed on 231 (93.5%) neonates. Auditory evoked potentials were requested for 150 neonates (60.1%), and 73 (29%) underwent the test, with no abnormal findings reported.
Of 42 patients diagnosed with congenital toxoplasmosis, only one did not receive treatment due to early death. Among the 41 treated patients, 21 (51.2%) received first-line treatment with pyrimethamine/sulfadiazine/folinic acid, 4 (9.5%) were treated with alternative regimens such as pyrimethamine/ sulfadoxine/folinic acid or trimethoprim-sulfamethoxazole, and 16 (39%) initially received alternative management while waiting for first-line treatment.
It is important to consider that 12 (28.5%) patients experienced difficulties with authorization, timely delivery, or consistent supply of medications, which led to the use of alternative regimens. Among patients diagnosed with congenital toxoplasmosis, 8 (19%) received corticosteroids; of them, 2 (4.75%) had chorioretinitis, while the remaining cases had unclear indications for steroid treatment.
Discussion
Evidence has shown that implementation of the clinical practice guideline improves the timely diagnosis and treatment opportunity of gestational and congenital toxoplasmosis, with a reduction in the number of severe cases and sequelae in children 2. This study is one of the few that evaluates the implementation of the Colombian clinical practice guideline for toxoplasmosis and found variable adherence -higher for treatment and lower for clinical or serological follow-up- in patients with suspected gestational toxoplasmosis. These findings are likely related to implementation barriers such as limited dissemination, insufficient training or updates for health personnel, and restricted access to diagnostic tests and follow-up care. These results align with those described by Wang et al. in their systematic review, which report a 60-70% non-compliance with the general clinical practice guidelines 15.
Adherence to the diagnostic recommendations for gestational toxoplasmosis ranges from 20 to 85.4%, with greater difficulty observed in the serological follow-up after the initial IgG and IgM screening. During diagnosis and serological follow-up, we found that a large number of the ordered IgG avidity tests and IgA serologies did not comply with the clinical practice guideline, which can alter the interpretation and lead to diagnostic errors 16. Almost 50% of amniocentesis had no clear indications. These practices can cause negative outcomes for the patient and represent unnecessary use of healthcare system resources, as reported by Liu et al16.
Spiramycin has been shown to reduce the risk of vertical transmission by up to 52% 7. During our study, 68.8% of mothers with gestational toxoplasmosis received this treatment. In comparison, Mejía-Oquendo et al. reported that only 52.5% of mothers were treated against T. gondii infection before the implementation of the clinical practice guideline. However, this percentage changed after its implementation, since all mothers received adequate treatment 17. In this study, conducted in Quindío, Colombia, central nervous system or retinal manifestations were observed in 8.7% of patients whose mothers received spiramycin as treatment compared to 28.2% of those whose mothers did not receive treatment 17. More than half of the pregnant women who received spiramycin did not meet the criteria outlined in the clinical practice guideline, suggesting a lack of clarity regarding the appropriate indication and timing for initiating secondary prevention 2^,^6. The Colombian and French clinical practice guidelines recommend that treatment for acute gestational toxoplasmosis should be started early, ideally within the first three to four weeks after seroconversion 2^,^9^,^18^,^19. This study identified different treatments initiated later than recommended.
According to the clinical practice guideline, diagnosis of congenital toxoplasmosis is defined by a history of gestational toxoplasmosis and positive neonatal serology 2. Adherence to diagnostic recommendations in newborns ranged from 0 to 50%. We highlight that seronegative results after birth do not rule out congenital toxoplasmosis 20. Therefore, some studies have established additional criteria to support the diagnosis, including: detailed physical evaluation, positive serology 6^,^21, IgG serology follow-up 6^,^21, molecular testing for T. gondii identification 6^,^21, and imaging studies to assess systemic compromise. A postnatal follow-up remains necessary in the first year of life to fully exclude the infection 4. Additionally, recent literature does not report Western blot for diagnosis, probably explained by the lack of commercial tests 6^,^21.
In contrast with the literature reporting up to 85% of patients with congenital toxoplasmosis as asymptomatic 11, the present study only found 19.1%. Central nervous system and retina involvement were the most frequent clinical manifestations. These findings can be explained by the fact that one of the two included hospitals is a referral center -where more severe cases are concentrated- and because of the low proportion of mothers (35.2%) who received spiramycin treatment.
The highest adherence (96.7%) was observed in the treatment of congenital toxoplasmosis using first-line schemes or therapeutic alternatives 6^,^12^,^21. This percentage reflects compliance with the clinical practice guideline at high complexity centers, guided by infectious disease specialists. In cases where first-line treatment or alternative regimens were unavailable, trimetoprim/sulfametoxazol was used. This scheme has been described by authors such as Hernández et al., particularly for cerebral toxoplasmosis in developing countries (in the absence of other regimens) due to several advantages, like tolerability, multiple formulations, and easy access 19. Additionally, the literature recommends corticosteroid treatment for patients with severe chorioretinitis or high protein levels (≥ 1 g/dl) 6 in the cerebrospinal fluid. This scenario occurred in a group of patients in this study, but the clinical practice guideline does not include these indications 2.
The literature reports that the time of maternal primary infection determines the risk of transmission and the severity of the clinical presentation in the neonate. In our study, seroconversion was more frequent during the second and third trimesters (more than 50%). However, cross-sectional analyses were not performed to associate seroconversion with the severity of the clinical presentation 6^-^7.
We identified several weaknesses related to the study's design, including possible data loss, as it relies on information recorded in electronic medical records. Additionally, a risk of selection bias exists as it includes patients assessed by infectious disease specialists in high-complexity centers.
Despite high morbidity and mortality associated with toxoplasmosis in newborns, knowledge gaps persist among pregnant women and healthcare providers regarding prevention, diagnosis, and treatment 22. Adherence to clinical practice guideline recommendations for toxoplasmosis was variable. Opportunities to enhance adherence have been identified, especially for the diagnosis and follow-up of pregnant women. Some clinical scenarios circumstances are not included in the clinical practice guideline but could be addressed in future updates. For example, recommendations for the clinical and paraclinical follow-up are not clear for children with suspected or diagnosed congenital toxoplasmosis. Institutions and governments should develop policies to provide periodic updates to prenatal and newborn care personnel 22.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guedez IV Barroso LA Caracterización del tratamiento de la toxoplasmosis gestacional Rev Salud Vive 20203697610.33996/revistavive.v 3i 8.44 · doi ↗
- 2Gómez-Sánchez PI Arévalo-Rodríguez I Rubio-Romero JA Guío JA Osorio-Castaño JH Buitrago-Gutiérrez G Guías de Práctica Clínica para la prevención, detección temprana y tratamiento de las complicaciones del embarazo, parto o puerperio. Sección Toxoplasmosis BogotáMinisterio de Salud y Protección Social - Colciencias 2013369400
- 3Cañón-Franco WA López-Orozco N Gómez-Marín JE Dubey JP An overview of seventy years of research (1944 - 2014) on toxoplasmosis in Colombia, South America Parasit Vectors 20147427427 https://doi/10.1186/1756-3305-7-4272519052510.1186/1756-3305-7-427PMC 4262115 · doi ↗ · pubmed ↗
- 4Franco PS Morais AC Silva RJ Araujo TE Gonzaga HT Ferreira C Systematic review and meta-analysis of congenital toxoplasmosis diagnosis: Advances and challenges J Trop Med 2024112710.1155/2024/1514178 PMC 1090158038419946 · doi ↗ · pubmed ↗
- 5Rosso F Agudelo A IsazaÁ Montoya JG Congenital toxoplasmosis: Clinical and epidemiological aspects of the infection during pregnancy Colomb Med Cali 200738316337
- 6Maldonado YA Read JS Byington CL Barnett ED Davies HD Edwards KM Diagnosis, treatment, and prevention of congenital toxoplasmosis in the United States Pediatrics 201713915210.1542/peds.2016-386028138010 · doi ↗ · pubmed ↗
- 7Thiébaut R Leproust S Chêne G Gilbert R SYROCOT (Systematic Review on Congenital Toxoplasmosis) Study Group Effectiveness of prenatal treatment for congenital toxoplasmosis: A meta-analysis of individual patients’ data Lancet 200736911512210.1016/S 0140-6736(07)60072-517223474 · doi ↗ · pubmed ↗
- 8Rueda-Páez YS Valbuena-Ruiz L Quintero-Pimiento N Pinilla-Plata A Sayago-Silva J Toxoplasmosis congénita, una mirada en la actualidad del tratamiento; revisión de la literatura Med UNAB 201922516310.29375/01237047.2612 · doi ↗