Factors associated with positive blood cultures in children in nine African and Asian countries: the ACORN2 surveillance network
Cristina Ardura-Garcia, Jill Hopkins, Sue J Lee, Naomi Waithira, Chris Painter, Clare L Ling, Tamalee Roberts, Thyl Miliya, Noah Obeng-Nkrumah, Japheth A Opintan, Emmanuel P Abbeyquaye, Raph L. Hamers, Yulia R Saharman, Robert Sinto, Mulya R Karyanti, R Fera Ibrahim

TL;DR
This study identifies factors that increase the likelihood of positive blood cultures in hospitalized children in low- and middle-income countries.
Contribution
The study provides a model to prioritize blood culture use in children based on clinical and demographic factors.
Findings
Blood cultures had a low diagnostic yield with true pathogens in only 4.5% of cases.
Children aged 5–18 years and those with severe clinical signs were more likely to have positive blood cultures.
Hospital-acquired infections and non-respiratory infections increased the likelihood of positive blood culture results.
Abstract
Blood culture (BC) in children has relatively low diagnostic yield and high contamination rates, limiting cost-effectiveness. We aimed to determine readily available baseline characteristics to identify hospitalised children with a likelihood of higher diagnostic yield in low- and middle-income countries. We used data from ACORN2, a prospective clinical surveillance network including 19 hospitals across Africa and Asia. We included participants <18 years, hospitalised for a suspected infection, prescribed parenteral antibiotics and with a BC sample. Sociodemographic and clinical data were recorded for each infection episode and linked to routine microbiology data. We described true pathogen (non-contaminant) BC positivity proportion and performed mixed-effects logistic regression, with study site and patient as the random effect, to identify factors associated with BC positivity. Of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
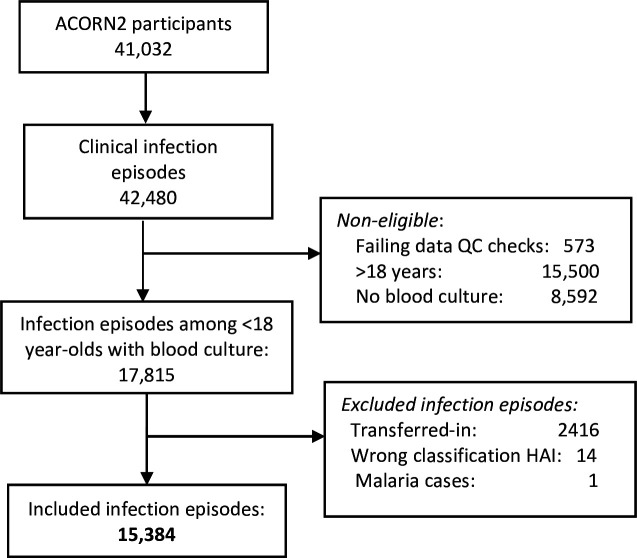 Figure 1
Figure 1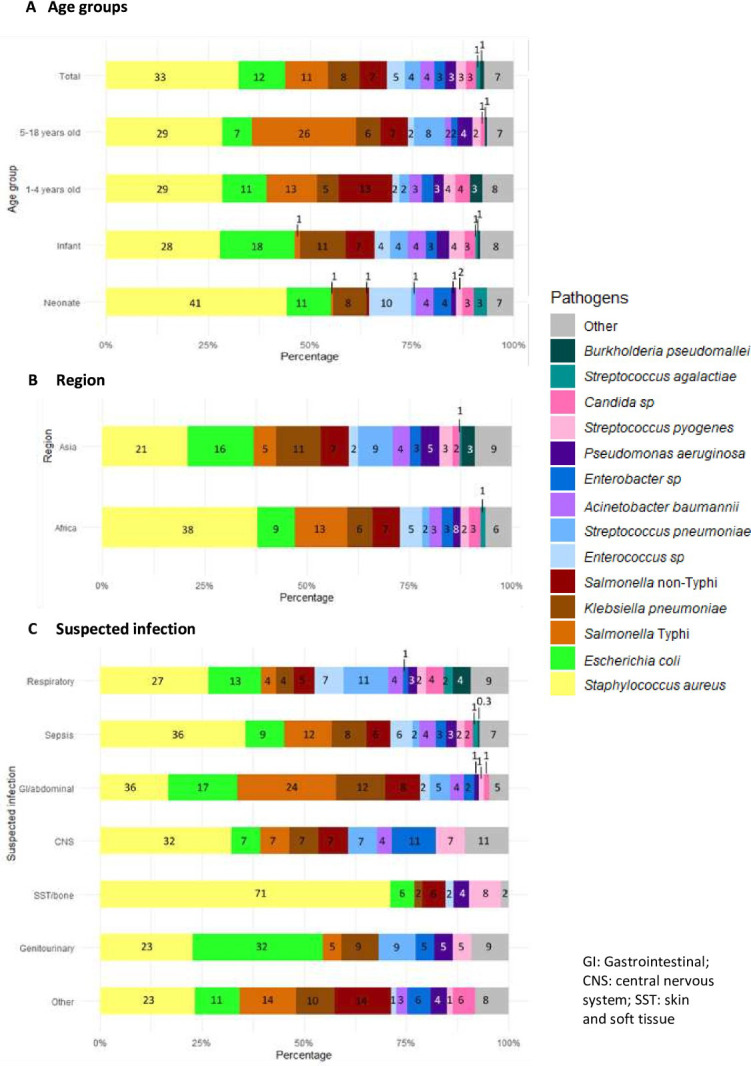 Figure 2
Figure 2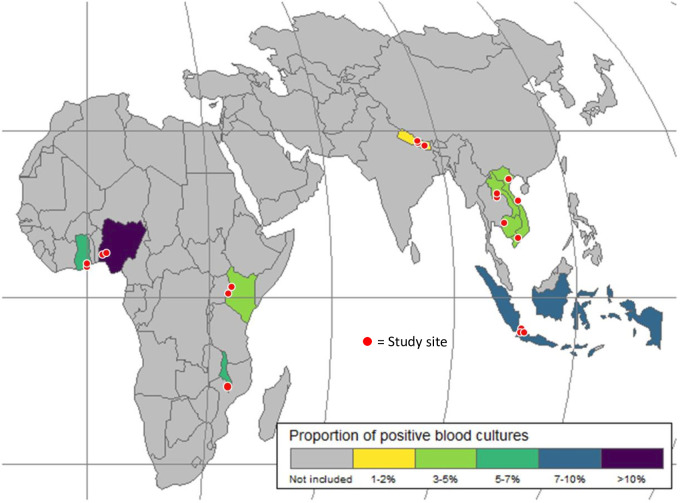 Figure 3
Figure 3| Characteristic | N | All | Blood culture results | P value | |
|---|---|---|---|---|---|
| Negative | Positive (n=689, 4.5%) | ||||
| Sociodemographics | |||||
| Region | 15 384 | <0.001 | |||
| Africa | 8391 (55) | 7917 (94.4) | 474 (5.6) | ||
| Asia | 6993 (45) | 6778 (96.9) | 215 (3.1) | ||
| Country | 15 384 | <0.001 | |||
| Ghana | 731 (4.8) | 688 (94.1) | 43 (5.9) | ||
| Indonesia | 395 (2.6) | 355 (89.9) | 40 (10.1) | ||
| Kenya | 3912 (25) | 3808 (97.3) | 104 (2.7) | ||
| Cambodia | 3152 (20) | 3061 (97.1) | 91 (2.9) | ||
| Laos | 1927 (13) | 1875 (97.3) | 52 (2.7) | ||
| Malawi | 2391 (16) | 2236 (93.5) | 155 (6.5) | ||
| Nigeria | 1357 (8.8) | 1185 (87.3) | 172 (12.7) | ||
| Nepal | 1282 (8.3) | 1257 (98.0) | 25 (2.0) | ||
| Vietnam | 237 (1.5) | 230 (97.0) | 7 (3.0) | ||
| Age (years), median (IQR) | 15 384 | 1.1 (0.1–4.1) | 1.1 (0.1–4.0) | 1.0 (0.1–5.9) | 0.900 |
| Age groups | 15 384 | <0.001 | |||
| <29 days | 3318 (22) | 3141 (94.7) | 177 (5.3) | ||
| 29 days-12 months | 3425 (22) | 3272 (95.5) | 153 (4.5) | ||
| 1–4 years | 5173 (34) | 5008 (96.8) | 165 (3.2) | ||
| 5–18 years | 3468 (23) | 3274 (94.4) | 194 (5.6) | ||
| Female sex | 15 372 | 6656 (43) | 6358 (95.5) | 298 (4.5) | >0.9 |
| Recent HC exposure | 15 259 | 3046 (20) | 2917 (95.8) | 129 (4.2) | 0.500 |
| Comorbidities | 15 384 | ||||
| Any | 2744 (18) | 2604 (94.9) | 140 (5.1) | 0.082 | |
| Cancer | 421 (2.7) | 397 (94.3) | 24 (5.7) | 0.200 | |
| Malnutrition | 442 (2.9) | 414 (93.7) | 28 (6.3) | 0.056 | |
| Infection episode | |||||
| Hospital acquired infection | 15 384 | 435 (2.8) | 358 (82.3) | 77 (17.7) | |
| Suspected diagnosis | 15 384 | <0.001 | |||
| Respiratory infection | 5396 (35) | 5260 (97.5) | 136 (2.5) | ||
| Sepsis | 4516 (29) | 4214 (93.3) | 302 (6.7) | ||
| GI or abdominal infection | 1308 (8.5) | 1226 (93.7) | 82 (6.3) | ||
| CNS infection | 979 (6.4) | 952 (97.2) | 27 (2.8) | ||
| SST or bone infection | 585 (3.8) | 533 (91.1) | 52 (8.9) | ||
| Genitourinary infection | 365 (2.4) | 343 (94.0) | 22 (6.0) | ||
| Other or unknown | 2235 (15) | 2167 (97.0) | 68 (3.0) | ||
| Clinical severity characteristics | |||||
| No clinical severity characteristics | 15 384 | 5993 | 5786 (96.5) | 207 (3.5) | <0.001 |
| Abnormal temperature | 15 187 | 5421 (36) | 5118 (94.4) | 303 (5.6) | <0.001 |
| Tachycardia | 14 784 | 3456 (23) | 3274 (94.7) | 182 (5.3) | 0.004 |
| Altered mental status | 15 013 | 3444 (23) | 3267 (94.9) | 177 (5.1) | 0.021 |
| Reduced peripheral perfusion | 14 268 | 1737 (12) | 1652 (95.1) | 85 (4.9) | 0.4 |
| Reduced activity (neonates) | 3165 | 596 (19) | 546 (91.6) | 50 (8.4) | <0.001 |
| Feeding difficulty (neonates) | 3084 | 918 (30) | 839 (91.4) | 79 (8.6) | <0.001 |
| Convulsions (neonates) | 3188 | 112 (3.5) | 98 (87.5) | 14 (12.5) | <0.001 |
| Clinical severity score, median (IQR) | 13 455 | 1 (0–2) | 1 (0–2) | 1 (0–2) | <0.001 |
| BC within 24 hours of admission | 15 318 | 14 677 (96) | 14 017 (95.5) | 660 (4.5) | 0.6 |
| Antibiotic 24 hours before BC | 13 559 | 3527 (26) | 3397 (96.3) | 130 (3.7) | 0.002 |
| Characteristic | Univariate | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P value | AOR | 95% CI | P value | |
| Sociodemographics | ||||||
| Age groups | ||||||
| <29 days | 1.13 | 0.90 to 1.42 | 0.275 | 0.97 | 0.76 to 1.23 | 0.812 |
| 29 days–12 months |
|
|
|
|
|
|
| 1–4 years | — | — | — | — | ||
| 5–18 years |
|
|
|
|
|
|
| Female sex | 0.96 | 0.82 to 1.12 | 0.607 | |||
| Recent HC exposure | 1.04 | 0.82 to 1.31 | 0.754 | |||
| Comorbidities | ||||||
| Any | 1.14 | 0.92 to 1.41 | 0.231 | |||
| Cancer | 1.36 | 0.86 to 2.14 | 0.188 | |||
| Malnutrition | 1.28 | 0.84 to 1.95 | 0.246 | |||
| Infection episode | ||||||
| Hospital acquired infection |
|
|
|
|
|
|
| Suspected diagnosis | ||||||
| Respiratory infection | — | — | — | — | ||
| Sepsis |
|
|
|
|
|
|
| GI or abdominal infection |
|
|
|
|
|
|
| CNS infection | 0.82 | 0.54 to 1.24 | 0.340 | 0.74 | 0.49 to 1.13 | 0.166 |
| SST or bone infection |
|
|
|
|
|
|
| Genitourinary infection |
|
|
|
|
|
|
| Other or unknown |
|
|
| 1.26 | 0.93 to 1.72 | 0.136 |
| Clinical characteristics | ||||||
| Abnormal temperature |
|
|
| |||
| Tachycardia |
|
|
| |||
| Altered mental status |
|
|
| |||
| Reduced peripheral perfusion |
|
|
| |||
| Number of clinical severity signs* |
|
|
|
|
|
|
| BC within 24 hours of admission | 1.36 | 0.91 to 2.03 | 0.136 | |||
| Antibiotic 24 hours before BC | 1.20 | 0.91 to 1.57 | 0.191 | |||
- —http://dx.doi.org/10.13039/100010269Wellcome Trust
- —http://dx.doi.org/10.13039/501100001711Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Streptococcal Infections and Treatments · Neonatal and Maternal Infections
Introduction
Blood culture (BC) has a low positive yield overall and is even lower in neonates and children.18 However, BC is the gold standard diagnostic method for bloodstream infections (BSIs), which are associated with high mortality in neonates and children.911 Published data on BC yield in children with suspected infection vary greatly from <1% to over 50%,18 depending on the setting, age, year performed (post Haemophilus influenzae type B and pneumococcal conjugate vaccine era) and inclusion criteria (hospitalised, sicker children). BCs are recommended in clinical practice guidelines for severe focal infections, such as pneumonia, skin and soft tissue (SST) or bone infections,1214 to attempt to identify the causative bacteria and guide targeted antibiotic treatment. As a result, they are performed in up to half of children hospitalised for suspected infections, depending on the setting and diagnosis.4 15 16 In addition, due to sampling difficulties, the contamination rate (positive BC with a non-pathogenic microbe) in paediatric BCs is often up to twofold to fourfold higher than the true-positive rate.7 17 18 Performing BCs that are not informative for patient management results in increased costs, longer hospital stays and suboptimal antibiotic use.1820
Targeting BCs to cases with a higher positive yield may enhance their cost-effectiveness and availability, particularly in resource-limited settings. The recent BC bottle shortage in the USA led to recommendations to reduce BC testing in low yield cases.21 Laboratory supply shortages, limited availability and the need for patients to pay out of pocket are recurrent issues in low- and middle-income country (LMIC) settings, which together with the high cost of an individual BC, highlight the need for more cost-effective BC testing. There are limited data on factors associated with BC positivity in children in LMICs. Existing severity prediction scores may identify children at risk of poor outcomes,2224 but do not identify children with bacteraemia,25 26 and they include measurements that are not always available in LMICs. Most paediatric studies on predictors of BC positivity have focused on specific bacterial species,27 infection syndromes,28 comorbidities (eg, febrile neutropenia)29 or age groups30 or were performed before the extensive implementation of pneumococcal conjugate vaccine.7 Laboratory tests, such as white blood cell count with differential or C-reactive protein, have also been associated with paediatric bacteraemia,8 28 31 32 but these are not always available in LMICs and the turnaround time may be too long for initial decision-making on need for BC testing. Clinical characteristics, such as lethargy, prolonged fever, comorbidities and hospitalisation, may also predict BC positivity in children,3 5 though evidence is scarce. In addition, specific focal infections such as SST or respiratory infections283337 have a lower BC yield, while infants and neonates have a higher yield than older children.38 39 It may therefore be possible to determine readily available factors that may help optimise BC sampling. We aimed to identify clinical factors associated with BC positivity in hospitalised children, using data from a multicentre antimicrobial resistance surveillance study from LMICs.
Methods
Study design and setting
A Clinically Oriented Antimicrobial Resistance Surveillance Network 2 (ACORN2) is an international prospective clinical surveillance study incorporated into the routine workflow in 19 hospitals from nine LMICs (Cambodia, Ghana, Indonesia, Kenya, Laos, Malawi, Nepal, Nigeria and Vietnam).11 40 In brief, participating hospitals collected sociodemographic data, clinical features, microbiology results and management data and outcomes of hospitalised patients treated with parenteral antibiotics for clinically suspected acute infection (online supplemental figure 1). The study was approved by the Oxford Tropical Research Ethics Committee (OxTREC 524–21), with additional approvals from local or national ethics committees for each hospital as required.
Study population
For this analysis, we included children under 18 years old enrolled into ACORN2 who had a valid blood sample sent for culture. We included both community-acquired infections (CAIs) and hospital-acquired infections (HAIs). We excluded children who had been transferred in from other health centres, those with an HAI where the date of symptom onset was less than 2 days after date of admission and those with a presence of malaria parasites.
Study procedures
Selected wards were screened daily to identify eligible participants with CAI and by weekly point prevalence surveys to identify HAI. Sociodemographic and clinical data were entered into a REDCap database.41 42 Prior to study commencement, site diagnostic microbiology laboratories were audited to determine readiness for surveillance, with corrective actions implemented to ensure alignment with accepted international quality standards. At the time of assessment, using the ACORN2 laboratory assessment tool, 12 laboratories were using a BD Bactec, four a BioMerieux BacT/Alert, two had both Bactec and Bact/Alert systems and two were using manual methods.11 Clinical and nursing staff were trained in the appropriate collection and transport of diagnostic microbiology specimens before the start of the study, with real-time monitoring via the project dashboard and quarterly follow-up of specimen processing at laboratory quality management meetings. This information and more can be found in the study′s diagnostic stewardship manual (https://doi.org/10.6084/m9.figshare.27900042.v2). Routine microbiology data were exported from laboratory information systems or WHONET files from each centre. Microbiology data were standardised and merged with clinical data via a RShiny app.43 Patients and infection episodes for each patient were assigned a unique identifier. Specimens were identified using the patient identifier and a specimen collection date and were linked to an infection episode if collected within two calendar days of the admission for CAI or if collected on or up to two calendar days following the day of symptom onset for HAI.
Definitions of exposures
We selected factors potentially associated with BC positivity based on previous literature3 5 7 8 25 26 28 30 and information available in the ACORN2 database44 . The selected factors included sociodemographics, recent healthcare exposure (previous 3 months), comorbidities and admission characteristics from the admission form, as well as suspected diagnosis, CAI versus HAI, clinical severity, BC timing (first 24 hours or later) and antibiotic exposure (24 hours before BC yes/no) from the infection episode form. Sociodemographic information included country, age and sex. Age was classified into four groups: neonates (<29 days), infants (29 days to 12 months), 1–4 year-olds and 5–18 year-olds, following frequently used age groups in paediatrics and the age distribution of the study sample. We included HIV/AIDS, tuberculosis, malnutrition, diabetes, cancer and heart, respiratory, neurologic, gastrointestinal (GI), hepatic, renal and rheumatologic or connective tissue diseases as ‘any comorbidity yes/no’. Suspected diagnoses were classified into respiratory infection, sepsis, GI or abdominal, central nervous system (CNS), SST or bone, genitourinary infection and other or unknown. Sepsis was defined as clinical sepsis with an unclear source, without an obvious source or when the source was not specified. The complete definition of clinical sepsis included in the study′s diagnostic stewardship manual may be found in the Supplementary Materials. HAIs were defined as a clinically suspected infection with symptom onset occurring >48 hours after admission and with prescription of new parenteral antibiotics; the rest were classified as CAI (including recent healthcare exposure). Clinical signs used for severity classification were abnormal temperature, tachycardia, altered mental status and reduced peripheral perfusion for every child (‘sepsis six’ for children,45 together with reduced activity, feeding difficulties and convulsions for neonates (WHO general danger signs for neonates)).46 We used each sign separately and as a continuous clinical severity score of 0–4 points (plus 0–7 points for neonates). For HAI, we recorded admission to the intensive care unit >48 hours, surgery during admission and medical devices as potential factors associated with BC positivity. Medical devices included peripheral venous catheter (PVC), central nervous catheter (CVC), urinary catheter and intubation, both independently and as a composite exposure variable (any medical device yes/no).
Definitions of outcomes
The outcome of interest for this analysis was a positive BC from an independent infection episode. BC results were classified into negative, contaminant, uncertain and pathogen. Negative BCs included reported results of no (significant) growth, no organism name, no culture result or blank. Contaminant bacteria included Bacillus spp (not anthracis), coagulase-negative staphylococci (lack of prematurity and medical devices), Corynebacterium spp (not diphtheriae), diphtheroids, Micrococcus spp, Cutibacterium and unidentified bacteria with only Gram stain result. Pathogens included WHO-GLASS / antimicrobial resistant priority organisms,47 miscellaneous Enterobacterales (defined as human pathogens in UK Standards for Microbiology Investigations ‘Identification of Enterobacteriaceae’),48 WHO Global Invasive Bacterial Vaccine-Preventable Disease/meningitis organisms,49 HACEK group, Brucella, Vibrio, Yersinia, Franciscella, beta-haemolytic Streptococci and Enterococci, Burkholderia pseudomallei, Chromobacterium, Candida (or ‘yeast’) and Cryptococcus. All other growth was defined as uncertain significance (online supplemental table 1).
Statistical analyses
Demographic and clinical data were tabulated and summarised using descriptive statistics, by BC positivity. We performed a mixed-effects logistic regression analysis to identify predictors of BC positivity (vs negative) per infection episode. We included study site and patient id as random effects to allow for different intercepts. All the variables described under ‘exposures’ were considered. A positive BC was defined as the presence of a ‘pathogen’, and the rest were defined as negative. When there was more than one identified bacterial species per infection episode per child, the infection episode’s BC was classified as positive if any were identified as ‘pathogen’, and negative in all other cases. Infection episodes with more than one isolated species classified as ‘pathogen’ were included as positive BCs (n=16). We constructed two multivariable models: one ‘simple’ model including exposures associated with BC positivity in univariable analysis with a p value ≤0.1 and one ‘stepwise’ model using automated stepwise backward selection methods. The final model was selected based on Akaike’s information criterion (AIC) and the log likelihood. Missing values were excluded from the analyses. Information available per variable is shown in table 1. We report (adjusted) ORs ((A)ORs) with 95% CIs. R statistical programme V.4.3.0 was used for computation.50
We described the pathogens found in infection episodes where none of the risk factors for BC positivity were present. We performed a sensitivity analysis, in which BCs classified as ‘uncertain’ were also defined as a positive BC. We also performed two subgroup analyses: one including only neonates (specified a priori) and another including only respiratory infections. The model for respiratory infections included only study site as random effect due to lack of convergence. Factors associated with BC positivity for HAI were reported in a descriptive table, but no further regression analysis was performed, as HAIs were not the main focus of this study and the number of positive BCs among this group was small, limiting any multivariable analysis.
Patient and public involvement
There was no patient or public involvement in the design and conduct of this study.
Results
Between 7 September 2021 and 31 March 2024, 41 032 patients were enrolled into ACORN2, including 26 407 paediatric infection episodes (from 26 000 paediatric patient admissions), of which 17 815 (67.5%) had a BC sample and 15 384 were included in this analysis (figure 1). Characteristics of the included infection episodes are summarised in table 1. Infection episodes were evenly distributed between African and Asian countries. Median age was 1.1 years (IQR: 0.1–4.1 years), including 3318 infections in neonates (21.6%), and 43.3% of the infections occurred in female children. Associated comorbidities were reported in 17.8% (2744) of infection episodes, the most common being malnutrition (442, 2.9%) and any type of cancer (421, 2.7%). One fifth (3,046) reported healthcare exposure during the previous 3 months and 435 (2.8%) were classified as HAI. The most common suspected diagnoses were respiratory infections (5396, 35.1%) and sepsis (4516, 29.4%). Among the clinical severity characteristics, the most common was an abnormal temperature (5421, 35.7%) and feeding difficulties among infection episodes in neonates (918, 29.8%). The median clinical severity score was 1 (IQR 0–2). Nearly all BCs were taken within the first 24 hours of admission or of symptom onset for HAI, and 26% (3527) of infections had received antibiotics in the 24 hours preceding the BC collection. Of the 435 HAI episodes, 74% (323) had a medical device in situ at HAI symptom onset, a PVC being the most common (301, 69.2%), with 5.3% having a CVC (23) and 7.4% a urinary catheter32 (online supplemental table 2).
Study population. HAI, hospital acquired infection; QC, quality control.
Out of the 15 384 infection episodes with a BC sample, 689 (4.5%) were positive for a pathogen. In 16 infection episodes, two bacterial species were identified as pathogens (total n=705). Contamination was identified in 9.1% of BCs (1399) and an uncertain pathogen in 0.9% (143). The most common pathogen was Staphylococcus aureus (229/705, 32.5%), followed by gram-negative bacilli: Escherichia coli (81, 11.5%), Salmonella Typhi (74, 10.5%), Klebsiella pneumoniae (54, 7.7%) and non-Typhi Salmonella sp (47, 6.7%). Distribution of pathogens varied by age with S. aureus being identified in 41.3% of positive BCs in neonates, E. coli in 18.4% in infants and S. Typhi in 25.5% in 5–18 year-olds. Distribution of pathogens also varied by region, with a larger proportion of S. aureus in African countries (37.8% vs 20.8% in Asian countries) and of Enterobacterales in Asian countries (E. coli: 16.3% vs 9.3% in African countries and K. pneumoniae: 10.9% vs 6.2% in Africa). Burkholderia pseudomallei was exclusively found in Asian countries (7, 3.2% of positive BCs) (figure 2 & online supplemental table 1).
Pathogens identified from the 689 positive blood cultures, by age group (A), by region (B) and by suspected infection (C). (n=705).
The proportion of positive (true pathogen) BCs varied by location from 2.0% in Nepal to 13% in Nigeria, averaging 3.1% (215/6993) in Asian countries and 5.6% (474/8391) in African countries (figure 3B, table 1). The distribution of BC positivity rate also varied by age, being higher in neonates (177, 5.3%) and infants (153, 4.5%), with a decrease among 1–4 year-olds (165, 3.2%), to increase again among 5–18 year-olds (194, 5.6%), with no differences by sex. BC yield was higher among children with HAI (17.7% vs 4.1%, 612/14949 among CAI). BC positivity rates also differed by initial diagnosis, with respiratory infections presenting the lowest (2.5%) and SST or bone infections being the highest (8.9%).
Countries and sites participating in ACORN2 and proportion of blood culture positivity.
In the univariate mixed-effects model, age group, HAI, diagnosis of suspected infections other than respiratory infections and each of the clinical severity characteristics were associated with BC positivity (table 2). All four clinical severity characteristics and the continuous composite clinical severity score were associated with BC positivity (table 2). We included only the composite clinical score in the multivariable model, as it had the lowest AIC when compared with models that included each severity characteristic separately. The best performing multivariable model (simple model) showed that 29 days–12-month-olds (AOR 1.33, 95% CI 1.06 to 1.66) and 5–18 year-olds (AOR 1.62, 95% CI 1.30 to 2.01) compared with 1–4 year-olds, and children with signs of clinical severity (AOR 1.29, 95% CI 1.18 to 1.40 per each additional sign) had higher odds of a positive BC. The odds of positive BC were three times higher for HAI when compared with CAIs (AOR 3.05, 95% CI 2.30 to 4.06). From the suspected diagnoses, sepsis (AOR 2.09, 95% CI 1.67 to 2.61), GI or abdominal (AOR 2.36, 95% CI 1.78 to 3.13), SST or bone (AOR 3.64, 95% CI 2.57 to 5.14) and genitourinary infection (AOR 2.22, 95% CI 1.39 to 3.56) were associated with BC positivity when compared with respiratory infections.
Next, we described the pathogens identified among children with none of the identified risk factors associated with BC positivity (see above, (online supplemental table 3). Among 1–4 year-olds with suspected community-acquired respiratory infection, there were 9/743 (1.2%) positive BCs if no clinical severity characteristic, and 18/818 (1.0%) if ≤1 clinical severity characteristic. The specific pathogens found in the latter group included only two cases of S. pneumoniae, as well as five S. aureus, two each of B. pseudomallei, yeast and Salmonella non-Typhi and one each of E. faecium, E. coli, Gr. A streptococcus, Mycobacterium and Salmonella Typhi.
The sensitivity analysis redefining BCs with ‘uncertain pathogen’ as positive (n=832 positive BCs) returned the same associated factors as the main analysis, though with weaker associations (online supplemental table 4). For the neonates’ subgroup analysis, we still found a strong association between HAI (AOR 4.46, 95% CI 2.56 to 7.77) and BC positivity (online supplemental table 5). Clinical severity signs were also independently associated with an increased odds of BC positivity of 1.18 (95% CI 1.05 to 1.32) for each added sign from the seven included in the clinical neonatal severity score. Sepsis (AOR 1.68, 95% CI 1.01 to 2.81) and SST or bone infection (AOR 2.64, 95% CI 1.01 to 6.88) were also associated with increased odds of BC positivity compared with respiratory infections. To better characterise the role of BC samples for respiratory infections in children, we analysed factors associated with BC positivity in this subgroup (online supplemental table 6). Results were similar to the main analysis, with the added importance of previous comorbidities (AOR 1.67, 95% CI 1.04 to 2.68), driven mainly by malnutrition (AOR 2.50, 95% CI 1.08 to 5.78).
Discussion
In this multicentre surveillance study, we found that only 4.5% of BC samples for hospitalised children under 18 years old were positive for pathogens, with a large variation between countries (2–13%). S. aureus was the most common BC pathogen in all age groups, though less prevalent in Asian countries where Gram-negative bacteria predominated. The main factors associated with a positive BC were age (infants and 5–18 year-olds), presence of clinical severity signs, HAI and having a suspected source other than respiratory or CNS infection. Among those with a suspected respiratory infection, associated comorbidities, especially malnutrition, also increased the rates of BC positivity.
Comparison with previous studies
The observed large variability in BC positivity rate (2–13%) found in our study has been reflected previously in children. However, our overall BC yield (4.5%) is still lower than the 19% pooled BC positivity rate (range 4–54%) reported in a LMIC 2011 meta-analysis including six Asian and six African paediatric studies.11 The meta-analysis included studies from the pre-pneumococcal conjugate and H. influenzae vaccines’ introduction, including children hospitalised for any reason (even without fever) and from both rural and tertiary urban hospitals11 which may explain the observed difference. Also, two thirds of the paediatric infection episodes in ACORN2 had a linked BC, a higher proportion than the under 50% reported in other studies from various settings4 15, which may have reduced BC yield in our study. However, as previously reported, BC positivity by site did not correlate with the proportion of infection episodes with a linked BC in ACORN2.11 The way BCs are performed (timing, volume and sterility) is not always optimal and this may affect BC yield and contamination rates.51 High contamination rates could lead to missing pathogens; however, the 9% contamination rate in our study was similar to other reports from LMICs (range 2–13%).2 6 38 52 53 Continuous adequate training to those performing BC may improve its yield, especially in settings with high staff turnover. All in all, the low BC yield and large variability highlight the opportunity to optimise BC sampling.
HAI was the strongest independent factor associated with BC positivity. Most previous studies did not analyse predictors for BC positivity among both community and HAI in the same population, hampering a comparison with our study. Risk factors for HAIs have been well described in children, including prolonged hospitalisation and PICU stay, comorbidities, invasive ventilation, central catheters, parenteral nutrition, blood transfusions and carbapenem use.5458 There is a critical lack of data on paediatric HAI risk factors from LMICs. In our study, the presence of medical devices, mainly CVC and urinary catheters, was more frequently reported in children with HAI and a positive BC (online supplemental table 2). Our findings highlight the relevant role of BCs for identifying the causative bacteria during HAIs in children. In settings where BCs are billed to patients and are not performed for patients who cannot pay, these data suggest that other billing models should be explored, in particular considering BC for in-patients as an overhead since the institution’s infection prevention and control programme benefits considerably from performing BCs for patients that may have HAIs.
Clinical severity signs were also associated with BC yield. Temperature, heart rate, mental status and peripheral perfusion may be combined into a clinical severity score, showing a steady increase of the odds for a positive BC with each added clinical sign, with no relevant difference in the size of the effect of each individual sign. Clinical signs have been previously reported as predictors of BC positivity in children, both in high and LMICs.56 5966 Abnormal temperature6 60 66 and altered mental status5 6 59 61 are the signs more frequently associated. The Yale Observation Scale (YOS) is a clinical score containing six observational items (quality of cry, reaction to parent, state variation, colour, hydration and response to social overtures), developed to identify febrile under 2-year-olds with bacterial infections.24 67 The YOS has been studied as a predictor for BC positivity, mainly in 3–36 month-olds with fever without a source, with varying results depending on cut-off used and study population characteristics,63 64 68 69 but with poor discrimination ability for invasive bacterial infections in infants <2 months old.25 In contrast, in our neonatal subgroup analysis, the additional three WHO general danger signs increased the probability of a positive BC, both when used individually and as a composite clinical severity score together with the previous four clinical signs, confirming the robustness of the association between the chosen clinical signs and BC positivity. Altogether, we showed that simple clinical signs that require no equipment other than a watch may be used in children of different ages to identify those with a higher BC yield.
Neonates, 1–12 month-olds and 5–18 year-olds had a higher BC positivity proportion than 1–4 year olds in our study, though only 1–12 months old and 5–18 year olds showed an association when adjusting for other factors. Age is rarely reported as being associated with BC yield, as most previous studies were targeted at specific age groups.3 5 6 63 Even though high BC positivity has been reported in some neonatal and infant studies,38 39 it may still be limited by the reduced sensitivity associated with a smaller blood sample (1–2 mL of blood),70 despite using appropriate BC bottle sizes. The higher positivity rate in 5–18 year-olds may be explained by the larger proportion of typhoid fever in this age group (26%), as older age has been previously identified as a predictor for BC positivity in children with typhoid fever.27
BC utility for respiratory infections has been questioned3336 despite some international guidelines’ recommending them for children admitted for moderate or severe community-acquired pneumonia (CAP).12 In our study, suspected respiratory and CNS infections had the lowest BC yield (2.5% and 2.8%, respectively) compared with other suspected infections, a difference that remained in the final adjusted model. This low yield for CAP (1–3%) has been repeatedly reported,15 16 71 but BCs are still obtained in 30–50% of cases.15 16 71 Among children with a suspected respiratory infection, we found that those with clinical severity signs and other comorbidities, especially malnutrition, have a higher BC yield. Malnutrition has been associated with BC positivity in children irrespective of the suspected infection.3 6 61 72 73 Our study supports previous authors suggesting that BCs are not indicated in healthy children admitted for non-critical CAP.16 36 Non-culture-based diagnostics may prove useful in this population, though with lack of evidence for reducing antibiotic use in children,74 75 and limited availability in LMICs.
Strengths and limitations
ACORN2 is a multicentre study that included a large number of children from nine LMICs with a high burden of infection. It was embedded into routine clinical care, resulting in real-life clinical setting data, where BC specimens were requested according to the treating physician’s criteria. We therefore feel our findings are relevant to other tertiary hospitals with BC access in LMICs in the African and Asian regions. To ensure completeness and reduce bias, information on sociodemographic and clinical factors was recorded prospectively via standardised case record forms. In addition, we performed a mixed-effects model with study site as the random effect to adjust for potential differences between the sites that could act as uncounted confounders. Sites included in ACORN2 underwent laboratory assessments and continuous laboratory quality monitoring, diagnostic stewardship and site-specific surveillance trainings. This ensured a minimum diagnostic quality across sites. This study also presents some limitations. First, we lacked information on birth parameters such as gestational age and birth weight for neonates, factors that have been associated with BC positivity.76 Second, the observed differences in BC yield between sites may be due to differences in clinical criteria for suspected diagnosis and in microbiological sampling, introducing selection bias despite diagnostic stewardship. Third, on occasions, there was more than one infection episode per child, but this was not accounted for in the analysis as it was not reliably collected. Fourth, while CAIs were enrolled daily, HAIs were enrolled once a week; therefore, suspected HAIs with negative BCs where antibiotics had already been stopped on the day of recruitment were not enrolled in the study, which may have biased BC positivity for HAIs towards a higher proportion. Finally, baseline information on exposures, including previous antibiotics exposure, was patient (or parent) reported, a potential source of information bias.
Implications for practice and future research
Increasing cost-effectiveness of diagnostic methods is crucial, especially in resource-limited settings. The low BC yield reported in this multi-centre study should encourage public health entities and health centres to develop protocols to optimise BC indications. The findings from our study may be used to identify children hospitalised with a suspected infection, for which diagnostic stewardship efforts to increase BC uptake should be prioritised, and others in which it could be limited in times of financial or logistic constraints. Not performing BCs in children with suspected infections requiring hospitalisation may lead to missing bacteraemias caused by pathogens not covered by empiric antibiotic treatment. However, among those with the lowest risk, only 1% of BCs were positive. Another consideration is the impact of avoiding BCs for non-critical respiratory infections on invasive pneumococcal disease surveillance, and strategies to maintain adequate surveillance would be required. Finally, researchers may wish to take our work one step further by developing a prediction score for BC positivity to be used directly by healthcare workers.
Future research should also focus on improving culture-based, and on developing culture-independent, diagnostic tools for BSI. BC costs are partly due to expensive and not easily available consumables, such as BC bottles.21 Efforts should focus on developing cheaper alternatives for BC consumables. Existing blood collection diversion devices may reduce BC contamination rates,77 but new technologies are needed to overcome other limitations, mainly low sensitivity and slow turnaround time (24–72 hours).51 78 79 In addition, limiting access to over-the-counter antibiotics would reduce the proportion of children who had already received antibiotics at admission to healthcare (26% in the current study), increasing BC positivity yield. Culture-independent diagnostics that are fast, accurate, require low volumes and skills and are accessible for both high and LMICs are urgently needed,78 79 and healthcare settings should be actively preparing for these new technologies through education and digitalisation.79 These culture-independent diagnostics may be especially relevant for cases where BC yield is the lowest, such as respiratory infections. Finally, our findings using the international ACORN2 network data stress the need for microbiological surveillance collaboration networks which provide real-life international microbiological data.
Conclusion
BC yield in children hospitalised for suspected infection is low. We identified specific groups where efforts to enhance BC testing should be prioritised, and others where it could be restricted during times of financial or logistical limitations. We highlight the relevant role of BC testing as part of the septic screening for HAI in children.
Supplementary material
10.1136/bmjgh-2025-020448online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Astete JA Batlle A Hernandez-Bou S et al Blood culture diagnostic yield in a paediatric emergency department Eur J Emerg Med 2014213364010.1097/MEJ.000000000000009924300246 · doi ↗ · pubmed ↗
- 2Crichton H O’Connell N Rabie H et al Neonatal and paediatric bloodstream infections: Pathogens, antimicrobial resistance patterns and prescribing practice at Khayelitsha District Hospital, Cape Town, South Africa S Afr Med J 20181089910.7196/SAMJ.2018.v 108i 2.1260129429440 · doi ↗ · pubmed ↗
- 3Droz N Hsia Y Ellis S et al Bacterial pathogens and resistance causing community acquired paediatric bloodstream infections in low- and middle-income countries: a systematic review and meta-analysis Antimicrob Resist Infect Control 2019820710.1186/s 13756-019-0673-531893041 PMC 6937962 · doi ↗ · pubmed ↗
- 4Mukhula VT Harawa PP Phiri C et al Evaluating blood culture collection practice in children hospitalized with acute illness at a tertiary hospital in Malawi J Trop Pediatr 202370 fmad 04310.1093/tropej/fmad 04338055837 PMC 10699738 · doi ↗ · pubmed ↗
- 5Ogunkunle TO Adedoyin TO Ernest SK et al A Prospective Cohort Study of the Clinical Predictors of Bacteremia in Under-Five Children With Acute Undifferentiated Fever Attending a Secondary Health Facility in Northwestern Nigeria Front Pediatr 2021973008210.3389/fped.2021.73008235242726 PMC 8885983 · doi ↗ · pubmed ↗
- 6Reddy EA Shaw AV Crump JA Community-acquired bloodstream infections in Africa: a systematic review and meta-analysis Lancet Infect Dis 2010104173210.1016/S 1473-3099(10)70072-420510282 PMC 3168734 · doi ↗ · pubmed ↗
- 7Sard B Bailey MC Vinci R An analysis of pediatric blood cultures in the postpneumococcal conjugate vaccine era in a community hospital emergency department Pediatr Emerg Care 20062229530010.1097/01.pec.0000215137.51909.1616714955 · doi ↗ · pubmed ↗
- 8Tsai C-M Lin C-HR Zhang H et al Using Machine Learning to Predict Bacteremia in Febrile Children Presented to the Emergency Department Diagnostics (Basel)20201030710.3390/diagnostics 1005030732429293 PMC 7277905 · doi ↗ · pubmed ↗